Endoscopic septotomy for symptomatic bariatric surgical complications: a new frontier of endoluminal surgery
Abdulrahman Qatomah, Daryl Ramai, Christopher C. Thompson

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
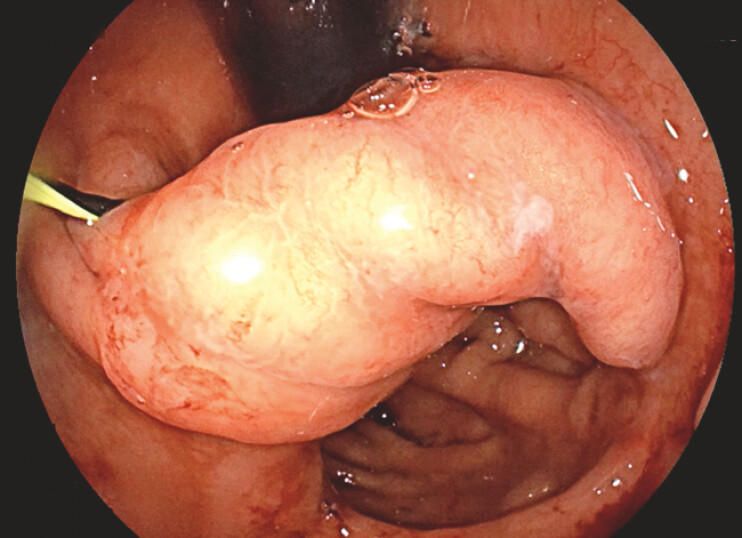 Fig. 1
Fig. 1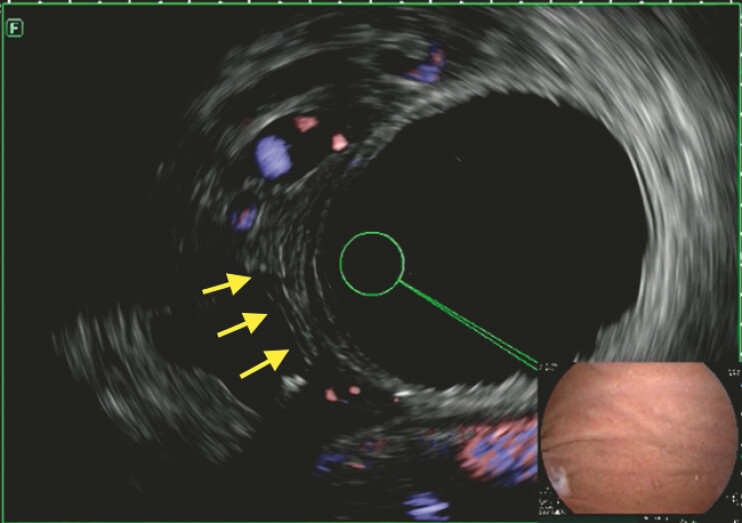 Fig. 2
Fig. 2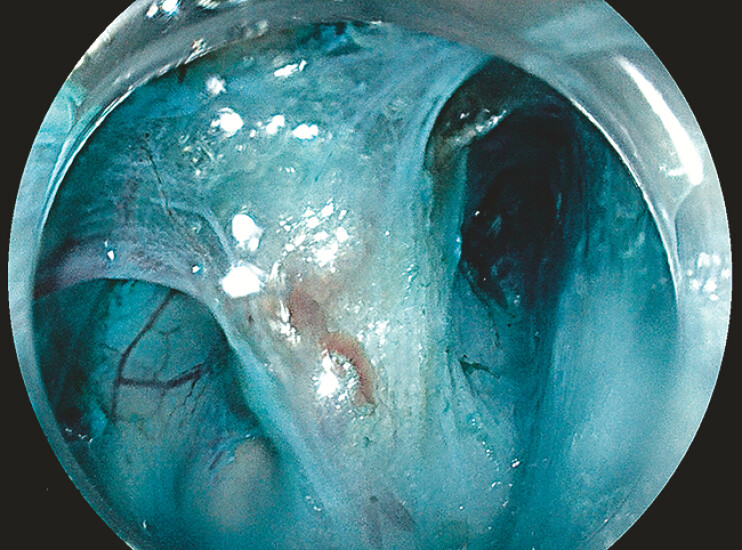 Fig. 3
Fig. 3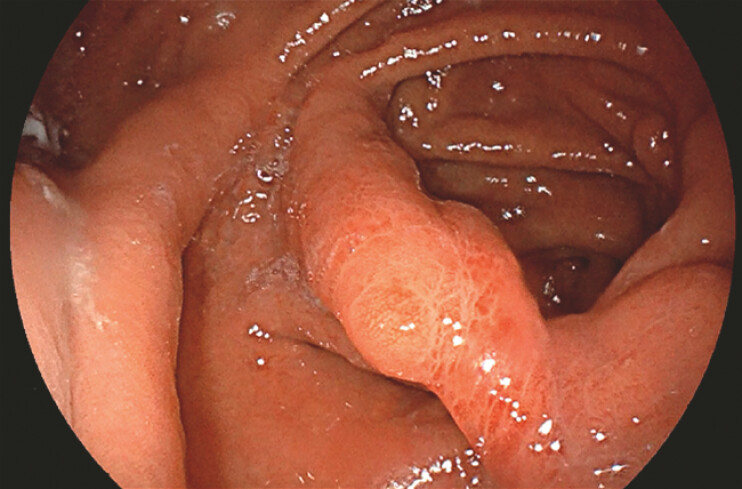 Fig. 4
Fig. 4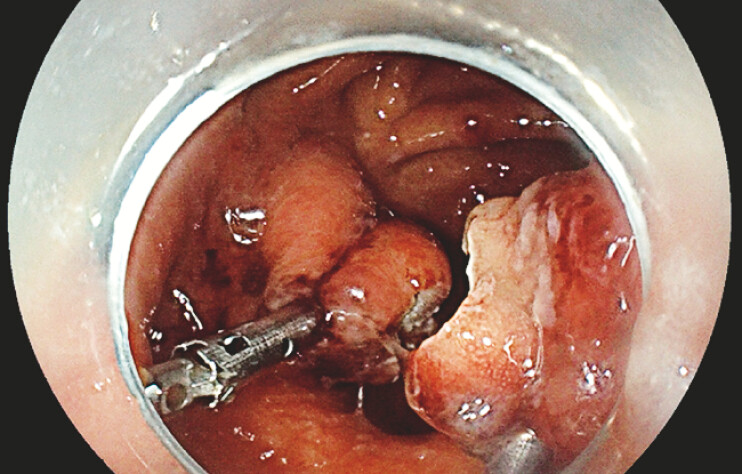 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBariatric Surgery and Outcomes · Gastroesophageal reflux and treatments · Esophageal Cancer Research and Treatment
Laparoscopic adjustable gastric banding (LAGB) and vertical band gastroplasty (VBG) are bariatric procedures that have declined in popularity due to long-term complications, including dysphagia secondary to esophageal dysmotility. Both procedures are associated with significant rates of reoperation or removal. Additionally, band erosion, though rare, is an established complication of LAGB that often manifests as chronic abdominal pain, dysphagia, and emesis 1 2 3 .
A 40-year-old man with a history of LAGB performed 20 years ago for weight loss which resulted in an eroded band, subsequently treated by surgical band removal and conversion to VBG due to weight regain. The patient developed gastric and esophageal dysmotility resulting in chronic abdominal pain and dysphagia that were not responsive to medical therapy. Upper endoscopy revealed post-VBG anatomy with a wide intragastric septum just distal to the LES causing an esophageal obstruction ( Fig. 1 ). Given the complexity of the surgical history, a multidisciplinary team determined that endoscopic therapy would be a feasible alternative to surgery.
Intragastric septum on an endoscopic examination (with wire guidance) on retroflexion view.
Partial septotomy was initially attempted. Careful endoscopic ultrasound (EUS) ( Fig. 2 ) and tissue oxygenation assessment demonstrated normal oxygenation with no significant vascular structures within the septum. Submucosal incision and tunneling were performed to expose inter-septal tissue ( Fig. 3 ) followed by septotomy using a needle-type knife. Mucosal flaps were successfully closed with an endoscopic suturing device with a single running suture consisting of eight bites ( Video 1 ).
EUS examination with Doppler without major Doppler activity within septum. Abbreviation: EUS, endoscopic ultrasound.
(video image): Inter-septal muscle exposed post submucosal tunneling.
Inter-septal muscle exposed post submucosal tunneling.Video 1
The patient experienced encouraging results, with some remaining symptoms, and wished to proceed with the completion septotomy. Repeat endoscopic and EUS examination demonstrated a reduced septal diameter without doppler-detectable vascular flow ( Fig. 4 ). Two large hemostatic clips were placed on the edges of the septum to prevent bleeding and perforation, followed by a successful complete septotomy using an insulated tip needle knife ( Fig. 5 ). To reinforce the edges and minimize bleeding risk, ligations were applied ( Video 1 ).
Follow-up endoscopy with a significant reduction in septum diameter.
Appearance post complete septotomy.
Endoscopic septotomy represents a technically feasible and minimally invasive intervention for managing complications arising after bariatric surgery. The procedure demonstrates a favorable safety profile, contingent upon strict adherence to cautionary protocols, including vascular mapping and measures to mitigate the risk of perforation.
Endoscopy_UCTN_Code_TTT_1AO_2AN
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Altieri MS Yang J Telem DA Lap band outcomes from 19,221 patients across centers and over a decade within the state of New York Surg Endosc 2016301725173210.1007/s 00464-015-4402-826201412 · doi ↗ · pubmed ↗
- 2Gamagaris Z Patterson C Schaye V Lap-band impact on the function of the esophagus Obes Surg 2008181268127210.1007/s 11695-008-9601-018663546 · doi ↗ · pubmed ↗
- 3Froylich D Abramovich TS Fuchs S Long-Term (over 13 Years) Follow-Up of Vertical Band Gastroplasty Obes Surg 2020301808181310.1007/s 11695-020-04448-w 32048151 · doi ↗ · pubmed ↗