Inadvertent portal vein stenting during endoscopic retrograde cholangiopancreatography for distal bile duct cancer: endoscopic rescue and spontaneous resolution of thrombosis
Seong-Hun Kim, Hyung Ku Chon

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
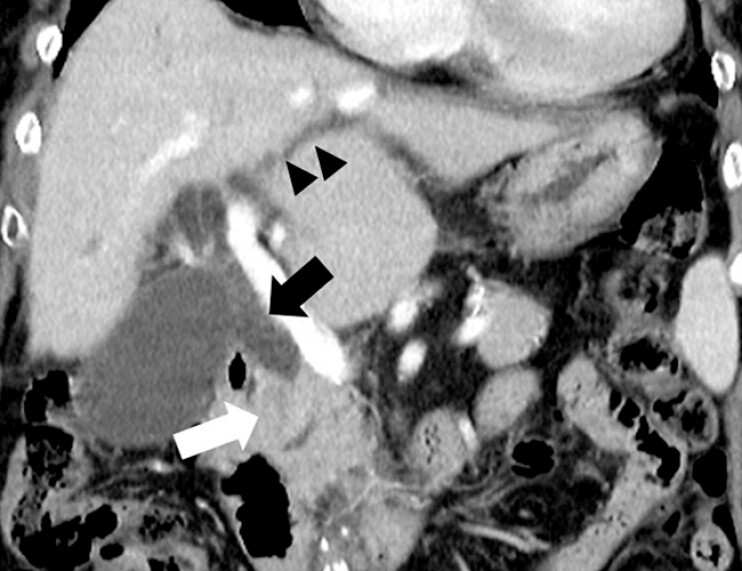 Fig. 1
Fig. 1 Fig. 2
Fig. 2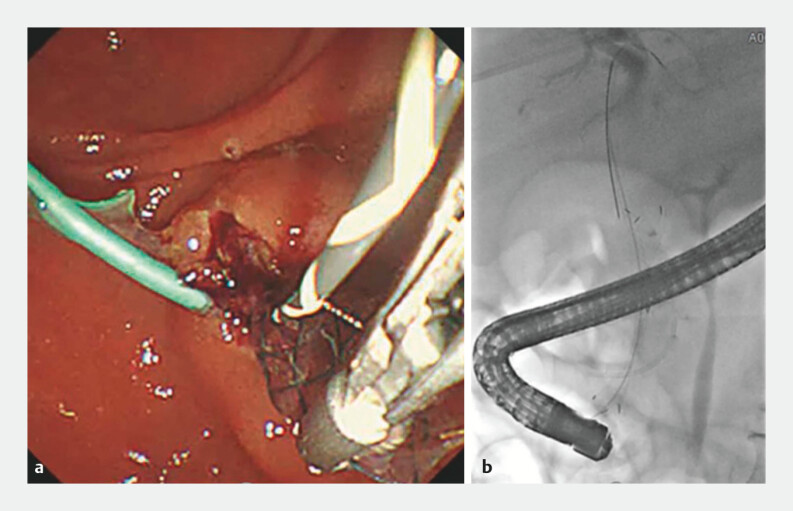 Fig. 3
Fig. 3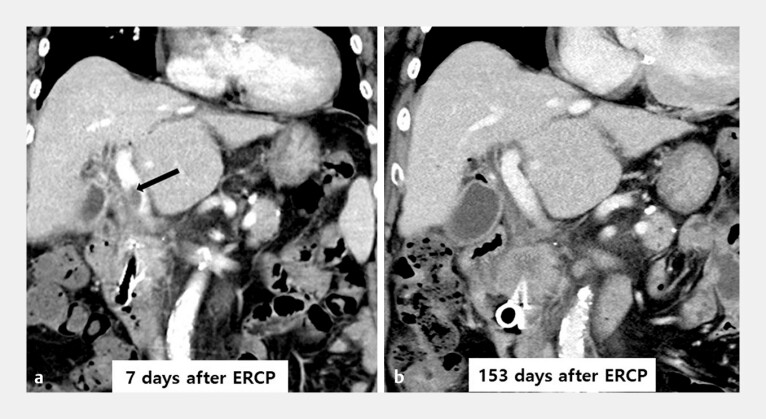 Fig. 4
Fig. 4- —Wonkwang University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Cholangiocarcinoma and Gallbladder Cancer Studies · Esophageal and GI Pathology
An 86-year-old woman with distal bile duct cancer and obstructive cholangitis presented with jaundice and a 5-kg weight loss over 1 month. She underwent endoscopic retrograde cholangiopancreatography (ERCP) for biliary decompression ( Fig. 1 ). Initial selective biliary cannulation failed, prompting placement of a plastic pancreatic duct stent followed by transpancreatic septotomy. A guidewire was advanced in the presumed direction of the bile duct and contrast injection suggested biliary opacification. Assuming correct guidewire placement, a fully covered self-expandable metal stent (FCSEMS) (HANAROSTENT Biliary Full Cover Benefit, 8 mm × 6 cm; M.I. Tech, Pyeongtaek, South Korea) was deployed. Substantial resistance was encountered during stent deployment, and the contrast rapidly washed out, raising suspicion of extrabiliary placement. A contrast-enhanced computed tomography (CECT) performed 2 hours later revealed that the FCSEMS had traversed the distal bile duct mass and had been inadvertently placed in the portal vein, resulting in acute portal vein thrombosis ( Fig. 2 ).
Coronal contrast-enhanced computed tomography images showing an enhancing mass (white arrow) in the distal common bile duct with upstream dilation of the intrahepatic (black arrow heads) and extrahepatic bile ducts (black arrow), suggestive of distal bile duct cancer.
Contrast-enhanced computed tomography obtained 2 hours post-endoscopic retrograde cholangiopancreatography showing maldeployed fully covered self-expandable metal stent (white arrow) in the portal vein via the distal bile duct mass, with associated portal vein thrombosis (black arrow).
An emergency ERCP was performed, during which selective biliary cannulation was achieved via needle-knife precutting. The misplaced stent was retrieved, and a new FCSEMS (HANAROSTENT Biliary Lasso Full covered, 10 mm × 6 cm; M.I. Tech) and plastic stents were successfully deployed into the bile duct ( Fig. 3 , Video 1 ). The patient recovered uneventfully and was discharged 10 days later. Follow-up CECT 7 days later showed portal vein thrombosis, which had resolved spontaneously by Day 153 without anticoagulation ( Fig. 4 ).
Retrieval and replacement of the fully covered self-expandable metal stent (FCSEMS). a Endoscopic image showing selective bile duct cannulation with subsequent retrieval of the maldeployed FCSEMS using forceps during emergency endoscopic retrograde cholangiopancreatography. b Fluoroscopic image demonstrating correct placement of a new FCSEMS within the bile duct.
Endoscopic rescue and spontaneous resolution of thrombosis after inadvertent portal vein stenting during endoscopic retrograde cholangiopancreatography for distal bile duct cancer.Video 1
Contrast-enhanced computed tomography. a At 7 days post- endoscopic retrograde cholangiopancreatography, demonstrating portal vein thrombosis (black arrow). b The portal vein thrombosis had spontaneously resolved by follow-up imaging on Day 153 without anticoagulant therapy.
Portal vein injury is a rare but potentially fatal complication of ERCP 1 2 . This case underscores the importance of recognizing signs of vascular misplacement, such as rapid contrast washout and deployment resistance. Early recognition and prompt endoscopic management are critical to avoiding serious complications. Notably, the spontaneous resolution of portal vein thrombosis without anticoagulation suggests that conservative management may be appropriate in selected patients with localized, nonocclusive thrombosis.
Endoscopy_UCTN_Code_TTT_1AR_2AZ
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Christensen SH Roga NF Kirkegaard J Nygaard J Migrated biliary stent into the portal vein: a case report J Surg Case Rep 20242024 rjae 06510.1093/jscr/rjae 065PMC 1087176438370583 · doi ↗ · pubmed ↗
- 2Tasar P Kilicturgay SA Portal vein injury following endoscopic retrograde cholangiopancreatography: a case report Ulus Travma Acil Cerrahi Derg 20232944344710.14744/tjtes.2022.2892336880609 PMC 10225845 · doi ↗ · pubmed ↗