Prevalence of and Risk Factors for Extremely Low Birth Weight Infants in Saudi Arabia: A Four-Year Single-Center Experience
Mohammad Alhasoon

TL;DR
This study examines the prevalence and risk factors for extremely low birth weight infants in Saudi Arabia over four years, identifying key factors like multiple births and maternal age.
Contribution
The study provides new insights into specific risk factors for ELBW infants in Saudi Arabia using a four-year single-center dataset.
Findings
The prevalence of ELBW infants was 0.71% over four years at King Abdulaziz Medical City.
Twin and triplet births were significant risk factors for birth weight less than 750 grams.
Lower gestational age and prolonged rupture of membranes were linked to birth weights of 750-1000 grams.
Abstract
Introduction Globally, extremely low birth weight (ELBW) infants present a distinct challenge for neonatologists, representing a significant portion of the most vulnerable and high-risk cases admitted to the neonatal intensive care units (NICUs). Saudi Arabia has a high prevalence of ELBW, which leads to a significant risk of morbidity and mortality, as many of these extreme preterm infants who are admitted to NICUs may not survive till discharge. This study aimed to evaluate the prevalence of ELBW infants and associated risk factors over a four-year period. Methods Two study designs were used in this research: a cross-sectional retrospective design was used for estimating the prevalence rate over four years, and a case-control study with a retrospective chart review for the risk factor correlation. The study was conducted at King Abdulaziz Medical City (KAMC), Riyadh, Kingdom of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
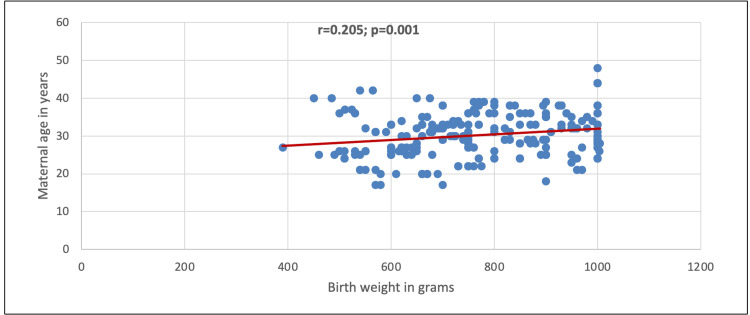 Figure 1
Figure 1| Study variables | Total, n (%) | Gender | P-value § | |
| Male (n=145), n (%) | Female (n=111), n (%) | |||
| Gestational age | ||||
| 23 - 26 weeks | 58 (22.7%) | 32 (22.1%) | 26 (23.4%) | 0.469 |
| 27 - 29 weeks | 43 (16.8%) | 28 (19.3%) | 15 (13.5%) | |
| 30 - 33 weeks | 155 (60.5%) | 85 (58.6%) | 70 (63.1%) | |
| Maternal age | ||||
| ≤30 years | 133 (52.0%) | 77 (53.1%) | 56 (50.5%) | 0.674 |
| >30 years | 123 (48.0%) | 68 (46.9%) | 55 (49.5%) | |
| Parity | ||||
| None | 56 (21.9%) | 30 (20.7%) | 26 (23.4%) | 0.772 |
| 1 – 2 | 154 (60.2%) | 90 (62.1%) | 64 (57.7%) | |
| >2 | 46 (18.0%) | 25 (17.2%) | 21 (18.9%) | |
| Mode of delivery | ||||
| NSVD | 51 (19.9%) | 23 (15.9%) | 28 (25.2%) | 0.063 |
| Cesarean section | 205 (80.1%) | 122 (84.1%) | 83 (74.8%) | |
| Antenatal steroid use | ||||
| No | 32 (12.5%) | 21 (14.5%) | 11 (09.9%) | 0.539 |
| Incomplete course | 37 (14.5%) | 21 (14.5%) | 16 (14.4%) | |
| Complete course | 187 (73.0%) | 103 (71.0%) | 84 (75.7%) | |
| Maternal comorbities | ||||
| Maternal hypertension/preeclampsia | 27 (10.5%) | 15 (10.3%) | 12 (10.8%) | 0.904 |
| Maternal diabetes | 40 (15.6%) | 23 (15.9%) | 17 (15.3%) | 0.905 |
| PPROM (>18 hours) | 45 (17.6%) | 28 (19.3%) | 17 (15.3%) | 0.704 |
| Chorionicity | ||||
| Singleton | 27 (10.5%) | 14 (09.7%) | 13 (11.7%) | 0.758 |
| Dizygotic DC DA | 114 (44.5%) | 66 (45.5%) | 48 (43.2%) | |
| Monozygotic DC DA | 38 (14.8%) | 23 (15.9%) | 15 (13.5%) | |
| Monozygotic MC DA | 03 (01.2%) | 01 (0.70%) | 02 (01.8%) | |
| Monozygotic MC MA | 56 (21.9%) | 30 (20.7%) | 26 (23.4%) | |
| Triplets | 12 (04.7%) | 06 (04.1%) | 06 (05.4%) | |
| Spontaneous or assisted conception | ||||
| Spontaneous | 140 (54.7%) | 74 (51.0%) | 66 (59.5%) | 0.180 |
| Assisted | 116 (45.3%) | 71 (49.0%) | 45 (40.5%) | |
| Number of fetuses | ||||
| Twins | 34 (13.3%) | 20 (13.8%) | 14 (12.6%) | 0.692 |
| Triplets | 148 (57.8%) | 84 (57.9%) | 64 (57.7%) | |
| Quadruplets | 56 (21.9%) | 30 (20.7%) | 26 (23.4%) | |
| Quintuplets | 12 (04.7%) | 06 (04.1%) | 06 (05.4%) | |
| Sextuplets | 06 (02.3%) | 05 (03.4%) | 01 (0.90%) | |
| Outcome | ||||
| Death* | 33 (12.9%) | 16 (11.0%) | 17 (15.3%) | 0.311 |
| Alive | 223 (87.1%) | 129 (89.0%) | 94 (84.7%) | |
| Study Variables | Birth weight | P-value § | |
| 750-1000 g (n=147), n (%) | <750 g (n=109), n (%) | ||
| Sex | |||
| Male | 76 (51.7%) | 69 (63.3%) | 0.064 |
| Female | 71 (48.3%) | 40 (36.7%) | |
| Gestational age | |||
| 23 - 26 weeks | 45 (30.6%) | 13 (11.9%) | <0.001 ** |
| 27 - 29 weeks | 12 (08.2%) | 31 (28.4%) | |
| 30 - 33 weeks | 90 (61.2%) | 65 (59.6%) | |
| Maternal age | |||
| ≤30 years | 69 (46.9%) | 64 (58.7%) | 0.062 |
| >30 years | 78 (53.1%) | 45 (41.3%) | |
| Parity | |||
| None | 27 (18.4%) | 29 (26.6%) | 0.148 |
| 1 – 2 | 89 (60.5%) | 65 (59.6%) | |
| >2 | 31 (21.1%) | 15 (13.8%) | |
| Mode of delivery | |||
| NSVD | 29 (19.7%) | 22 (20.2%) | 0.928 |
| Cesarean section | 118 (80.3%) | 87 (79.8%) | |
| Maternal comorbidities | |||
| Maternal hypertension/preeclampsia | 15 (10.2%) | 12 (11.0%) | 0.836 |
| Maternal diabetes | 26 (17.7%) | 14 (12.8%) | 0.291 |
| PPROM (>18 hours) | 32 (21.8%) | 13 (11.9%) | <0.001 ** |
| Antenatal steroids use | |||
| No | 20 (13.6%) | 12 (11.0%) | 0.825 |
| Incomplete course | 21 (14.3%) | 16 (14.7%) | |
| Complete course | 106 (72.1%) | 81 (74.3%) | |
| Chorionicity | |||
| Singleton | 27 (18.4%) | 0 | <0.001 ** |
| Dizygotic DC DA | 52 (35.4%) | 62 (56.9%) | |
| Monozygotic DC DA | 16 (10.9%) | 22 (20.2%) | |
| Monozygotic MC DA | 02 (01.4%) | 01 (0.90%) | |
| Monozygotic MC MA | 38 (25.9%) | 18 (16.5%) | |
| Triplets | 12 (08.2%) | 0 | |
| Quintuplets | 0 | 06 (05.5%) | |
| Spontaneous pregnancy or assisted conception | |||
| Spontaneous | 80 (54.4%) | 60 (55.0%) | 0.921 |
| Assisted | 67 (45.6%) | 49 (45.0%) | |
| Number of fetuses | |||
| Twins | 34 (23.1%) | 0 | <0.001 ** |
| Triplets | 63 (42.9%) | 85 (78.0%) | |
| Quadruplets | 38 (25.9%) | 18 (16.5%) | |
| Quintuplets | 12 (08.2%) | 0 | |
| Sextuplets | 0 | 06 (05.5%) | |
| Outcome | |||
| Death | 24 (16.3%) | 09 (08.3%) | 0.057 |
| Alive | 123 (83.7%) | 100 (91.7%) | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeonatal Respiratory Health Research · Child Nutrition and Water Access · Infant Nutrition and Health
Introduction
Around the world, extremely low birth weight (ELBW) accounts for a total of 1.2-1.5% of all live births and 15-20% of admissions to neonatal intensive care units (NICUs) [1]. Prematurity accounts for approximately 11.1% of all pregnancies and births; however, the survival rates of ELBW infants have significantly increased over the past half-century [2,3]. Improvements in neonatal intensive care helped to lower the rates of morbidity and death.
Nonetheless, the high rate of ELBW births in Saudi Arabia poses significant mortality risks, as nearly one-third of preterm infants admitted to NICUs do not survive to discharge [4]. There is a dearth of trustworthy quantitative data highlighting the prevalence of ELBW newborns in Saudi Arabia and the risk factors that are linked to them. A study analysed the differences in survival rates between 1994 and 2019 [1]; however, few recent studies have investigated which specific intervention strategies for preterm newborns are most effective in reducing prevalence rates or mitigating the associated risks [5-7]. Performance standards could be set that obstetricians can use to track changes in local institutions' rates of morbidity and death. However, while analyzing the immediate and long-term health consequences of premature births [8], researchers must also examine the number of preterm births resulting in ELBW. Given that ELBW frequently leads to major health issues after birth, its epidemiological ramifications are so great that there is a dire need for additional empirical data to assess the maternal and perinatal factors influencing ELBW. Also, the paucity of literature indicates that there must be more evidence-based suggestions for better clinical judgment. More focus on regional and local differences in ELBW prevalence rates is necessary to close these gaps. To record how Saudi Arabian women manage the risks of preterm and mortality, survey or interview data must be gathered.
Materials and methods
The study was conducted at King Abdulaziz Medical City (KAMC), Riyadh, Kingdom of Saudi Arabia, covering four years, from January 2017 to December 2020. KAMC is a single hospital with one NICU that includes three levels of care: Level III with 40 beds, Level II (also referred to as the Intermediate Care Nursery) with 36 beds, and Level I, which is the regular nursery. The hospital has an average of approximately 9,000 deliveries per year, including both newborns needing care and admitted to the NICU and healthy newborns who room-in with their mothers. Two study designs were used in this study: (i) a cross-sectional retrospective design was used to estimate the prevalence rate over the four years, and (ii) a case-control design with retrospective chart review for correlating the associated risk factors.
All live-born infants weighing 1000 g or less at birth, delivered at KAMC, were included in the study. Infants born outside KAMC and those with fatal anomalies like Trisomies 13, 18, and major congenital anomalies like anencephaly were excluded from the study. The pregnancy notes on the mothers were reviewed blindly without knowledge of the newborn outcome.
More than 10 variables were assessed, including demographic data and perinatal events such as maternal age, parity, maternal diabetes, maternal hypertension/preeclampsia, prolonged premature rupture of membranes (PPROM) defined as “rupture of membranes more than 18 hours before delivery”, the use of antenatal steroids, spontaneous pregnancy or assisted conception, number of fetuses, birth weight, gestational age, and sex of newborn.
Statistical analysis
The data were analyzed using IBM SPSS Statistics for Windows, version 26 (Released 2019; IBM Corp., Armonk, New York, United States). Descriptive statistics were given as numbers and percentages (%) for all categorical variables. The association of sex and birth weight with other measured variables was analyzed using the Chi-square test. In addition, the Pearson correlation coefficient was performed to determine the correlation between maternal age and gestational age according to birth weight. A p-value of less than 0.05 was considered significant.
Ethical concerns
The King Abdullah International Medical Research Centre (KAIMRC) institutional review board approved the study (approval number: RC20/283/R) and waived the patient consent as the study design was a retrospective chart review and no identifiable patient data were used. The study was carried out in accordance with relevant guidelines and regulations and the Declaration of Helsinki.
Results
Out of a total of 36,000 newborns over the study period of four years, 256 were classified as ELBW. The prevalence of ELBW during this period was 0.71%. As seen in Table 1, 22.7% of the pregnancies had a gestational age between 23 and 26 weeks. More than half (52%) had a maternal age of 30 years or less. Approximately 60.2% had 1-2 parities. The most preferred mode of delivery was cesarean section (80.1%). A total of 187 (73.0%) underwent the complete course of antenatal steroids. The most common maternal factor was PPROM (17.6%). Chorionicity was mostly dizygotic dichorionic diamniotic (44.5%). Spontaneous conception was recorded in 54.7%. Triplet fetuses constituted 57.8% of the ELBW births, and mortality rates accounted for 12.9%. When comparing male and female newborns, it was observed that the difference between sexes did not reach statistical significance for any of the measured characteristics (p>0.05 for all variables).
Table 2 presents a comparison of various maternal, fetal, and perinatal characteristics between two groups of neonates with extremely low birth weights: those weighing 750-1000 g and those weighing less than 750 g. Several statistically significant associations were observed. It shows that increasing gestational age (p<0.001) and PPROM (p<0.001) were more strongly associated with birth weight of 750-1000 g, whereas birth weight under 750 g was more closely linked to dizygotic DC DA (p<0.001) and triplet pregnancies (p<0.001). Other variables such as sex, maternal age, parity, mode of delivery, maternal comorbidities (hypertension, diabetes), use of antenatal steroids, and method of conception (spontaneous vs. assisted) were not significantly associated with differences in birth weight between the two groups. Though a higher proportion of male infants was observed in the <750 g group (63.3% vs. 51.7% in the 750-1000 g group), this did not reach statistical significance (p=0.064). Finally, while a higher mortality rate was observed in the 750-1000 g group (16.3%) compared to the <750 g group (8.3%), this difference was not statistically significant (p=0.057), possibly due to improved survival rates with intensive neonatal care.
*Table 2: Association of study variables with birth weight (N=256)§ P-value was calculated using Chi-square test; outcome of death was defined as the baby passing away before hospital discharge; ** Significant at p<0.05 levelDC: dichorionic; DA: diamniotic; MC: monochorionic; MA: monoamniotic; ELBW: extremely low birth weight; PPROM: prolonged premature rupture of membranes; NSVD: normal spontaneous vaginal delivery
In Figure 1, a statistically significant positive correlation between birth weight and maternal age was observed (r=0.205; p=0.001).
Correlation between birth weight and maternal age
Discussion
This study investigated the prevalence of ELBW and the risk factors for it in a tertiary healthcare setting. The prevalence of ELBW in the four-year study period was found to be 0.71% (256 out of 36000 baby births). This is almost consistent with a study conducted in Bahrain, which reported an incidence of very low birth weight (VLBW) of 0.52% over a 10-year period (August 1986 to July 1996) [9]. Similarly, a study done in Jeddah found that the prevalence of very low birth weight (VLBW) in three maternity and children hospitals in Jeddah City was 3.3% [10], which was also in accordance with the VLBW incidence rate in Canada [11] and in India [12]. Furthermore, we noted that 57.4% of infants were considered to have a birthweight of 750-1000 g, and the rest were <750 g (42.6%). In a study from Spain, 37 children (21.8%) were classified as having ELBW (birth weight less than 1000 g), while 18.8% were classified as extremely preterm (gestational age less than 28 weeks) [13]. These findings indicate that even though the prevalence of ELBW is not high in many countries, it still exists. Improvements in perinatal care in recent years have significantly reduced the mortality and morbidity of ELBW infants.
Data from this study suggests that birthweight <750 g was more likely to be a product of multiple gestation and had a direct association with either twin or triplet fetuses. However, no significant link was observed between mortality and birth weight groups (750-1000 g vs. <750 g) (p=0.057). Contradicting this, Tchamo et al. found an increased risk for death, growth retardation, and delayed neurodevelopmental among surviving VLBW and ELBW infants [14]. In a study published in 2014, weight, height, and head circumference at the time of discharge were positively correlated with VLBW infants (p<0.001) [10].
Moreover, the lowest gestational age (23-26 weeks) and PPROM (>18 hours) had direct associations with birthweight 750-1000 g (p<0.001) but found no significant association between birth weight and other maternal factors, such as maternal age, number of parity, mode of delivery, maternal hypertension/preeclampsia, and maternal diabetes (p>0.05). This is not consistent with the study of Berger et al. [15]. Based on their accounts, a higher risk for preterm birth with early gestational age was positively associated with pre-pregnancy hypertension and pre-eclampsia. In contrast, preterm birth with late gestational age was correlated positively with maternal diabetes. This corroborated a study done in Germany by Spiegler et al., who reported that, based on regression estimates, hypertension and advanced maternal age increased the risk for preterm birth [16]. Also, they found that maternal hypertension was predicted to suffer a clinically specified preterm delivery, which may increase the chance of more VLBW infants with a modest growth restriction and fewer intraventricular hemorrhage in grades 3 or 4. Notwithstanding these reports, Anil et al. documented that maternal weight gain, preterm birth, and comorbidity during pregnancy were the significant risk factors for low birth weight [17].
Incidentally, we noted that increasing birthweight was positively correlated with maternal age, but increasing gestational age was inversely correlated with birthweight. This further suggests that every increase in maternal age will also likely increase infant birth weight; however, every increase in gestational age is directly correlated with a decrease in birth weight. Corroborating these reports, according to the adjusted regression model documented in Canada [18], late maternal age was found to be directly associated with preterm birth, and maternal age between 30 and 34 years was significantly associated with a lower risk of prematurity. In Nepal, the risk of low birth weight was more likely exhibited by mothers who had four or more antenatal (ANC) visits [19]. However, this was opposed by a study done in Burkina Faso by Lingani et al., wherein the frequency of ANC visits carried out by the mother during pregnancy was not identified as a protective factor for low birth weight [20].
This study has some limitations. First, the results of this study are not generalizable to the general population because it is a single-hospital-based study, and the data reflect the experience of a single institution. Therefore, extrapolations and interpretations of our results must be made with caution. Second, this study was retrospective in nature, with data for both mothers and infants extracted from charts and medical records. As a result, the study depended on the accuracy of existing documentation, and some maternal and infant information was unavailable for certain participants.
Conclusions
Over the four-year period, the prevalence of ELBW was found to be relatively low in this study. Reduced gestational age and PPROM emerged as key risk factors for infants with birth weights of 750-1000 g, while multiple pregnancies, such as twins and triplets, were notably linked to birth weights below 750 g. Further investigation is warranted to better understand the prevalence of ELBW and to identify its contributing risk factors.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Survival rate of very low birth weight infants over a quarter century (1994-2019): a single-institution experience J Neonatal Perinatal Med Al Qurashi MA 2532601420213307419910.3233/NPM-200595 · doi ↗ · pubmed ↗
- 2Prospective study of early and late outcomes of extremely low birthweight in Central Saudi Arabia BMC Pediatr Abolfotouh MA Al Saif S Altwaijri WA Al Rowaily MA 2801820183013486510.1186/s 12887-018-1248-y PMC 6106812 · doi ↗ · pubmed ↗
- 3Epidemiological aspects of prematurity in the Eastern region of Saudi Arabia Saudi Med J Al-Qurashi FO Yousef AA Awary BH 4144193720162705228410.15537/smj.2016.4.14309 PMC 4852019 · doi ↗ · pubmed ↗
- 4Prevalence of adverse birth outcomes and associated factors in Jazan, Saudi Arabia: a cross-sectional study Medicine (Baltimore) Dallak FH Gosadi IM Haidar WN 0101202210.1097/MD.0000000000031119 PMC 957580536254006 · doi ↗ · pubmed ↗
- 5Association between platelet transfusion and mortality rate among preterm neonates in the Eastern Province, Saudi Arabia Med Arch Alhamad FA Hussien A Alqahtani F 2782827620223631394310.5455/medarh.2022.76.278-282PMC 9559875 · doi ↗ · pubmed ↗
- 6Mortality and major morbidities of very low birth weight infants at a teaching hospital in Saudi Arabia: a comparison of two periods Dubai Med J Altirkawi K Alyousef N Sobaih B Alhadid AJ Shaiba L Banoo R Fariss A 10010642021
- 7Decisions and outcome for infants born near the limit of viability Int J Pediatr Adolesc Med Al Hazzani F Al Alaiyan S Jabr MB 98101820213408488010.1016/j.ijpam.2020.03.008PMC 8144851 · doi ↗ · pubmed ↗
- 8Short- and long-term outcomes for extremely preterm infants Am J Perinatol Patel RM 3183283320162679996710.1055/s-0035-1571202 PMC 4760862 · doi ↗ · pubmed ↗