Combination of Neoadjuvant Gemcitabine‐Cisplatin and Anti‐Tuberculosis Therapy for a Patient With Muscle‐Invasive Bladder Cancer and Renal Granulomatosis That Progressed After Intravesical Bacillus Calmette‐Guérin Therapy
Takahiro Tsumori, Seiji Hoshi, Kei Yaginuma, Satoru Meguro, Kanako Matsuoka, Junya Hata, Yuichi Sato, Hidenori Akaihata, Soichiro Ogawa, Yoshiyuki Kojima

TL;DR
A patient with bladder cancer and kidney granulomatosis was successfully treated with a combination of chemotherapy and anti-tuberculosis therapy before surgery.
Contribution
Demonstrates the safe use of gemcitabine-cisplatin alongside anti-tuberculosis therapy in a complex clinical case.
Findings
Combining neoadjuvant gemcitabine-cisplatin with anti-tuberculosis therapy was feasible and safe.
Radical cystectomy was successfully performed after the combination therapy.
No complications or recurrence of granulomatosis were observed during treatment.
Abstract
A case of muscle‐invasive bladder cancer and renal granulomatosis that developed after intravesical Bacillus Calmette‐Guérin therapy, in which a combination of neoadjuvant gemcitabine‐cisplatin and anti‐tuberculosis therapy was safely administered, and radical cystectomy was ultimately performed, is reported. A 64‐year‐old man with non‐muscle‐invasive bladder cancer underwent transurethral resection and intravesical Bacillus Calmette‐Guérin therapy every time bladder cancer recurred. However, the patient developed left renal granulomatosis during treatment. Anti‐tuberculosis therapy was prioritized since there was no bladder cancer progression. However, local bladder cancer progression was observed during the anti‐tuberculosis therapy. To successfully cure the renal granulomatosis and suppress tumor progression, neoadjuvant gemcitabine‐cisplatin was combined with anti‐tuberculosis…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
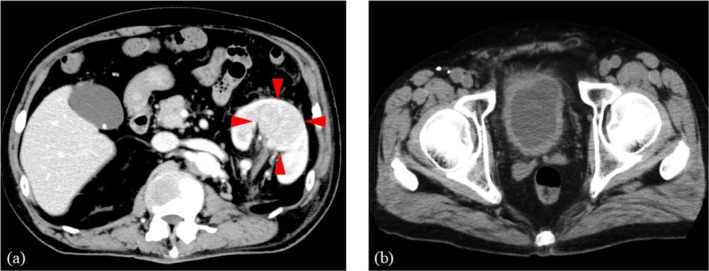 FIGURE 1
FIGURE 1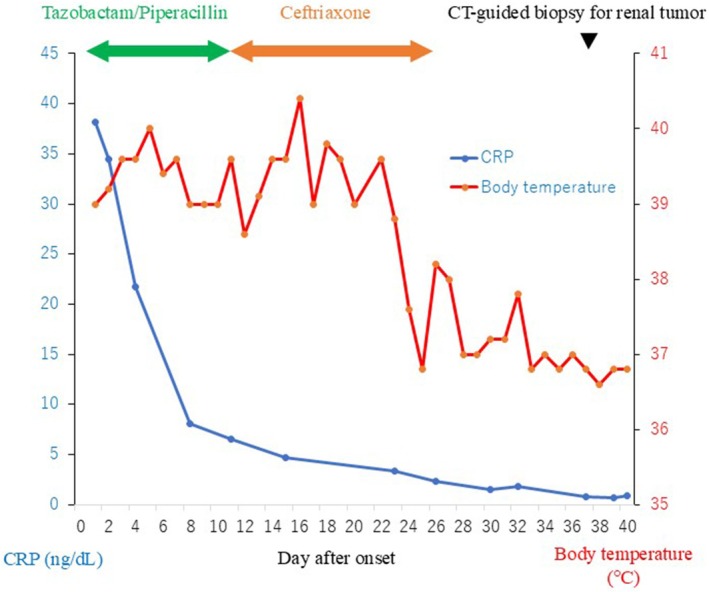 FIGURE 2
FIGURE 2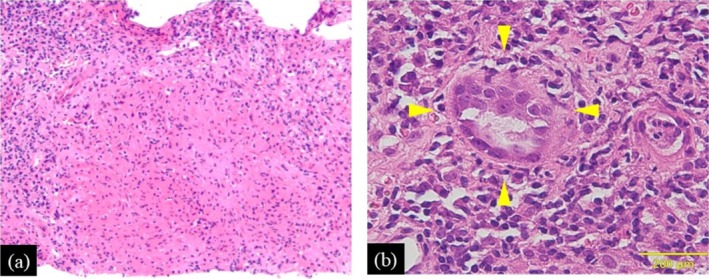 FIGURE 3
FIGURE 3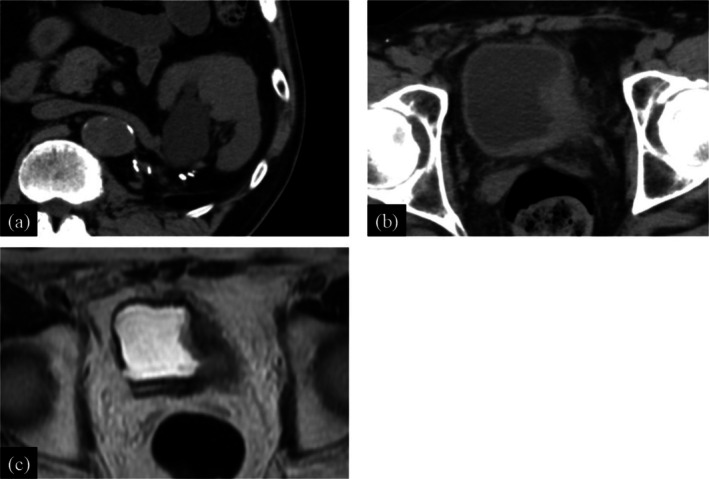 FIGURE 4
FIGURE 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBladder and Urothelial Cancer Treatments · Urinary and Genital Oncology Studies · Infectious Disease Case Reports and Treatments
Summary
- Renal granulomatosis is a rare complication of intravesical Bacillus Calmette‐Guérin therapy, and treatment strategies for patients with bladder cancer progression during treatment with anti‐tuberculosis therapy are unclear.
- We report a case of muscle‐invasive bladder cancer and renal granulomatosis that developed after intravesical Bacillus Calmette‐Guérin therapy, in which a combination of neoadjuvant gemcitabine‐cisplatin and anti‐tuberculosis therapy was safely administered.
AbbreviationsATTanti‐tuberculosis therapyBCabladder cancerBCGBacillus Calmette‐GuérinCRPC‐reactive proteinCTcomputed tomographyGCgemcitabine‐cisplatinMRImagnetic resonance imagingRCradical cystectomy
Introduction
1
Renal granulomatosis is a rare complication of intravesical Bacillus Calmette‐Guérin (BCG) therapy, and treatment strategies for patients with bladder cancer (BCa) progression during treatment with anti‐tuberculosis therapy (ATT) are unclear. A case of a patient with advanced BCa who safely received neoadjuvant gemcitabine‐cisplatin (GC) in combination with ATT for renal granulomatosis caused by BCG infection and underwent radical cystectomy (RC) successfully is reported.
Case Presentation
2
A 64‐year‐old man with BCa (urothelial carcinoma, pT1, high grade) was started on postoperative intravesical BCG therapy in February 2020. The patient underwent six induction BCG therapy sessions, followed by maintenance therapy every three sessions. Intravesical BCG therapy was effective, although the BCa recurred three times when it was discontinued due to painful urination. We recommended RC, but the patient strongly preferred bladder preservation. Therefore, transurethral resection was performed in May 2022, and intravesical BCG therapy was subsequently resumed. However, during the therapy, the patient presented with persistent fever in July 2022. Laboratory examination showed significantly elevated C‐reactive protein (CRP) (38.2 mg/dL), but interferon‐γ release assay was negative. Computed tomography (CT) showed a 48 × 40 mm^2^ abscess in the left kidney (Figure 1a). There was no obvious bladder tumor on CT (Figure 1b), and the urinary cytology was negative, indicating no BCa recurrence. Antibiotic therapy (tazobactam/piperacillin and ceftriaxone) was initiated for a left renal abscess. Although the CRP levels improved gradually, the fever was prolonged (Figure 2). A positive urine mycobacterial culture suggested renal granulomatosis due to BCG infection. Consequently, CT‐guided biopsy of the renal abscess was performed. Histological examination with hematoxylin and eosin staining showed granulomatous lesions (Figure 3a) and Langhans giant cells (Figure 3b), which were diagnosed as renal granulomatosis caused by BCG infection.
Contrast‐enhanced CT when the patient presented with persistent fever. (a) CT shows a 48 × 40 mm2 abscess in the left kidney. (b) CT shows no obvious bladder tumor.
The course of treatment until CT‐guided biopsy for renal abscess. Although the CRP levels improved gradually after the start of antibiotic therapy, the fever persisted.
Hematoxylin and eosin staining of the renal abscess. Histological examination shows a granulomatous lesion (a) and Langhans giant cells (b).
A 6‐month ATT regimen (rifampicin 600 mg/day + isoniazid 300 mg/day + levofloxacin 500 mg/day) was planned. However, at the time of starting the therapy, urine cytology became positive, suggesting BCa recurrence, but CT showed no bladder tumor. ATT was prioritized with careful follow‐up for BCa, and RC was planned after the ATT was completed. ATT was initiated in December 2022 and continued until May 2023. Four months after starting ATT, CT showed a reduction in the size of the left renal abscess to 30 × 31 mm^2^ (Figure 4a), and urine mycobacterial culture turned negative. However, CT and magnetic resonance imaging showed BCa progression on the left lateral wall of the bladder without metastases (Figure 4b,c). There was concern about renal granulomatosis recurrence if ATT was interrupted to perform an immediate RC, due to the insufficient duration of treatment completed at that point. Therefore, from April 2023 to May 2023, two cycles of neoadjuvant GC (gemcitabine 1000 mg/m^2^ on days 1, 8, 15, and cisplatin 25 mg/m^2^ on day 2) were administered every 3 weeks combined with ATT for 2 months. During the GC, the patient experienced Grade 2 neutropenia and Grade 1 thrombocytopenia, as defined by the Common Terminology Criteria for Adverse Events version 5.0. Based on WHO criteria [1], the resolution of renal granulomatosis was confirmed by the completion of the planned ATT and the negativity of urine mycobacterial cultures, followed by robot‐assisted RC and ileal conduit construction in June 2023. Histopathological examination showed urothelial carcinoma, ypT3aN0, RM0, ly1, v1. This patient has continued to show no recurrence of renal granulomatosis, and there has been no BCa recurrence for 6 months.
Plain CT images (a, b) and plain MRI image (c) 4 months after the start of anti‐tuberculosis therapy. (a) The size of the left kidney tumor has decreased, but hydronephrosis has appeared. (b) The size of the tumor on the left lateral wall of the bladder has increased. (c) The tumor on the left wall of the bladder shows extramural invasion.
Discussion
3
To the best of our knowledge, there have been no reports of chemotherapy, such as GC for BCa, while treating BCG infection, and its efficacy and safety have not been established. This is the first report in which the combination of neoadjuvant GC and ATT was safely administered, and RC was ultimately performed for the patient with muscle‐invasive BCa and renal granulomatosis that developed after intravesical BCG therapy.
Intravesical BCG therapy is an effective treatment for non‐muscle‐invasive BCa, but it is occasionally associated with serious complications such as renal infection [2, 3]. The incidence of renal infection after intravesical BCG therapy is 0.2%–2%, and renal granulomatosis occurred in < 0.1% of patients [4]. Therefore, the appropriate management of renal granulomatosis caused by BCG infection is unclear [5]. In general, for renal granulomatosis caused by BCG infection, 6 months of anti‐tuberculosis drugs were recommended in accordance with tuberculosis treatment, though the optimal duration of therapy has not been clarified [6], but shortening treatment duration may lead to renal granulomatosis recurrence [7]. In this case, since there was no evidence of BCa progression when renal granulomatosis developed, to cure the BCG infection, ATT was planned for a period of 6 months before performing the RC for BCG‐intolerant non‐muscle‐invasive BCa. However, 4 months into ATT, combining GC with ATT was considered necessary because the BCa had progressed. Although there are no reports of the safety of GC for BCa patients with renal granulomatosis caused by BCG infection, the safety and efficacy of combining chemotherapy and ATT have been reported in other cancers with tuberculosis [8, 9, 10]. When combining chemotherapy, neutropenia and thrombocytopenia, as well as liver dysfunction, are cited as adverse events associated with ATT. Although rifampicin induces CYP3A4 and CYP2C8, which may reduce the efficacy of some chemotherapies, this does not affect GC. In addition, because of the renal mass shrinkage that indicated improvement in renal granulomatosis, it was considered that the risk of renal granulomatosis recurrence became lower even if GC were introduced after 4 months of ATT.
Although the combination of GC and ATT was given safely in this case, it does not always apply to all patients. Because ATT generally requires 6 months, there is a risk of BCa progressing during treatment. Moreover, GC may cause immunosuppression [11], which increases the risk of BCG infection relapsing. Adverse events such as neutropenia and thrombocytopenia may necessitate a dose reduction of GC. Therefore, the combination therapy should be determined individually according to the symptoms of BCG infection and BCa progression. In this case, GC was safely administered 4 months after ATT when the BCG infection was under control. Regarding BCa, the present patient could wait to undergo RC because there was no obvious BCa progression at the start of ATT. This case suggests that the combination of GC and ATT may be safe after 4 months of ATT. Further research is needed to determine the efficacy and safety of the combination of GC and ATT.
Conclusion
4
This case, in which GC for BCa and ATT for renal granulomatosis caused by BCG infection were safely combined, suggests that this combination therapy may be safe when BCG infection is under control.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1N. N. Linh , K. Viney , M. Gegia , et al., “World Health Organization Treatment Outcome Definitions for Tuberculosis: 2021 Update,” European Respiratory Journal 58 (2021): 2100804.34413124 10.1183/13993003.00804-2021 · doi ↗ · pubmed ↗
- 2D. L. Lamm , B. A. Blumenstein , J. D. Crissman , et al., “Maintenance Bacillus Calmette‐Guerin Immunotherapy for Recurrent TA, T 1 and Carcinoma In Situ Transitional Cell Carcinoma of the Bladder: A Randomized Southwest Oncology Group Study,” Journal of Urology 163, no. 4 (2000): 1124–1129.10737480 · pubmed ↗
- 3R. J. Sylvester , M. A. Brausi , W. J. Kirkels , et al., “Long‐Term Efficacy Results of EORTC Genito‐Urinary Group Randomized Phase 3 Study 30911 Comparing Intravesical Instillations of Epirubicin, Bacillus Calmette‐Guérin, and Bacillus Calmette‐Guérin Plus Isoniazid in Patients With Intermediate‐ and High‐Risk Stage ta T 1 Urothelial Carcinoma of the Bladder,” European Urology 57, no. 5 (2010): 766–773.20034729 10.1016/j.eururo.2009.12.024PMC 2889174 · doi ↗ · pubmed ↗
- 4K. Tran‐Harding , R. T. Nair , and H. Ganesh , “Renal Granulomatosis Post Intravesical Bacillus Calmette‐Guerin Therapy for Non‐Muscle‐Invasive Bladder Cancer,” Journal of Clinical Imaging Science 8 (2018): 18.29770266 10.4103/jcis.JCIS_83_17PMC 5939034 · doi ↗ · pubmed ↗
- 5I. Tsuru , M. Nakamura , T. Izumi , et al., “Asymptomatic Renal Granuloma Diagnosed 3 Years After Bacillus Calmette‐Guérin Intravesical Injection: A Case Report and a Literature Review,” IJU Case Reports 6, no. 6 (2023): 377–381.37928297 10.1002/iju 5.12627 PMC 10622208 · doi ↗ · pubmed ↗
- 6M. A. Pérez‐Jacoiste Asín , M. Fernández‐Ruiz , F. López‐Medrano , et al., “Bacillus Calmette‐Guérin (BCG) Infection Following Intravesical BCG Administration as Adjunctive Therapy for Bladder Cancer: Incidence, Risk Factors, and Outcome in a Single‐Institution Series and Review of the Literature,” Medicine 93, no. 17 (2014): 236–254.25398060 10.1097/MD.0000000000000119 PMC 4602419 · doi ↗ · pubmed ↗
- 7WHO Guidelines Approved by the Guidelines Review Committee , WHO Consolidated Guidelines on Tuberculosis: Module 4: Treatment—Drug‐Susceptible Tuberculosis Treatment (World Health Organization, 2022).35727905 · pubmed ↗
- 8T. Hirashima , Y. Tamura , Y. Han , et al., “Efficacy and Safety of Concurrent Anti‐Cancer and Anti‐Tuberculosis Chemotherapy in Cancer Patients With Active Mycobacterium tuberculosis : A Retrospective Study,” BMC Cancer 18, no. 1 (2018): 975.30314434 10.1186/s 12885-018-4889-1PMC 6186130 · doi ↗ · pubmed ↗