A Case of Interstitial Cystitis With Hunner Lesions Involving Bilateral Ureters
Satoki Otsuka, Yoshiyuki Akiyama, Daichi Maeda, Aya Niimi, Kenichi Hashimoto, Jun Kamei, Satoru Taguchi, Yuta Yamada, Yusuke Sato, Daisuke Yamada, Tomonori Minagawa, Tetsuo Ushiku, Yukio Homma, Haruki Kume

TL;DR
A rare case of interstitial cystitis with Hunner lesions affecting the upper urinary tract in a 51-year-old woman is reported.
Contribution
This case highlights the unusual involvement of bilateral ureters in interstitial cystitis with Hunner lesions.
Findings
The patient developed bilateral ureteral stenosis and hydronephrosis linked to IC/HL.
Histological findings in the ureters matched chronic inflammatory changes seen in bladder lesions.
Corticosteroid treatment did not resolve ureteral stenosis despite improvement in bladder symptoms.
Abstract
Interstitial cystitis with Hunner lesion (IC/HL) is an enigmatic, chronic inflammatory disease of the urinary bladder. Few documented cases have reported the IC/HL involving the upper urinary tract. A 51‐year‐old Japanese woman with IC/HL developed bilateral ureteral stenosis and associated hydronephrosis, resulting in increased serum creatinine concentrations. Cystography showed no evidence of bilateral vesicoureteral reflux or bladder deformity. Ureteroscopy showed severe ureteral stenosis due to mucosal hyperplasia at the mid/upper levels of both ureters, leading to the insertion of bilateral ureteral stents. Histological examination of the ureteral lesions showed similar chronic inflammatory changes to the bladder lesions, which were compatible with IC/HL. Bilateral ureteral stenosis persisted after a two‐year corticosteroid treatment (prednisolone, 7.5 mg/day), while IC/HL…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
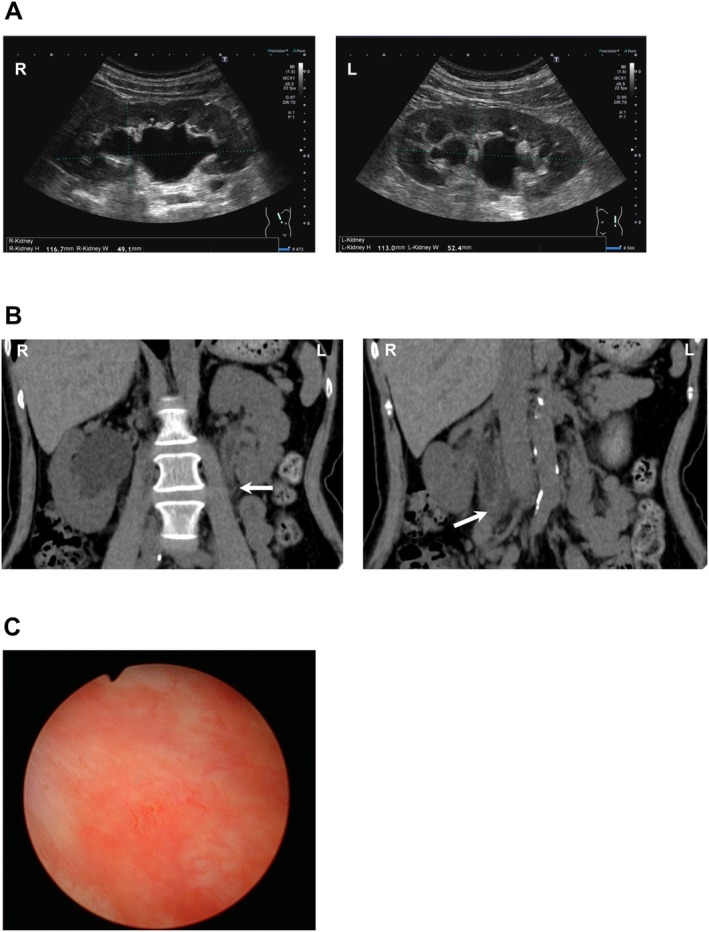 FIGURE 1
FIGURE 1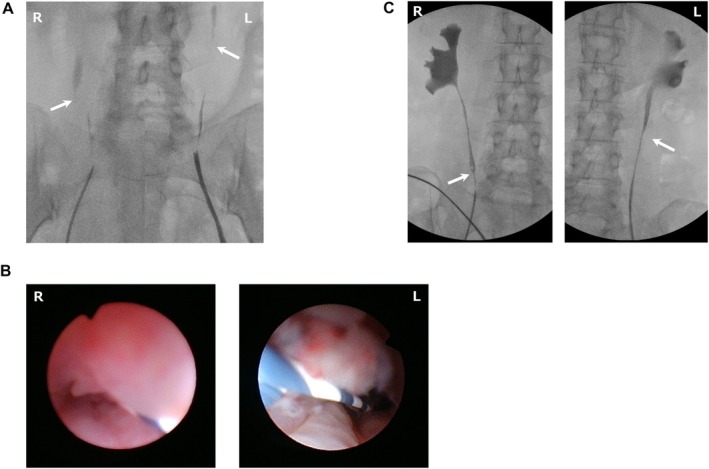 FIGURE 2
FIGURE 2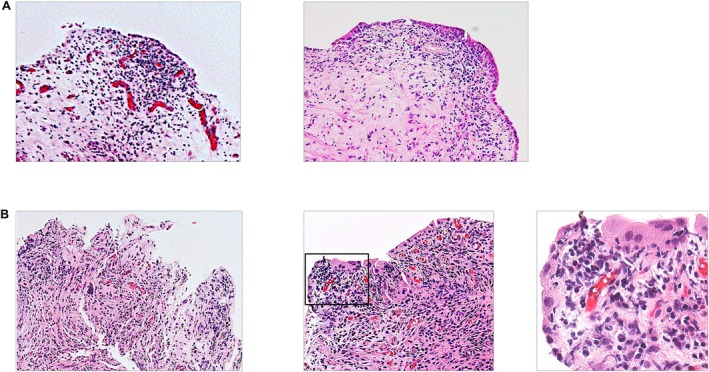 FIGURE 3
FIGURE 3| Hematology | |
| WBC | 2.8 × 103/μL |
| Hb | 12.5 g/dL |
| Plt | 45.0 × 106/μL |
| Blood chemistry | |
| Cre | 1.24 mg/dL |
| Estimated GFR | 36.3 mL/min/1.73m2 |
| CRP | 0.42 mg/dL |
| Blood coagulation | |
| Fibrinogen | 497 mg/dL |
| D‐dimer | 1.7 μg/mL |
| Urine analysis | |
| WBC | > 100/HPF |
| RBC | 50–99/HPF |
| Urine cultures and cytology | |
| Bacterial culture | No growth |
| Mycobacterial culture | No growth |
| Cytology | Class II |
| Others | |
| Anti‐ds‐DNA antibody | 1.7 U/mL |
| Anti‐ss‐DNA antibody | 14.1 U/mL |
| Anti‐SS‐A antibody | 75.8 U/mL |
| Anti‐SS‐B antibody | 0.9 U/mL |
| C3 | 136 mg/mL |
| C4 | 23 mg/mL |
| sIL‐2R | 631 U/mL |
| TSH | 2.49 μIU/mL |
| FT4 | 0.92 ng/dL |
| IgG | 1737 mg/dL |
| IgG4 | 50.8 mg/dL |
- —Japan Society for the Promotion of Science10.13039/501100001691
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrinary Bladder and Prostate Research · Urological Disorders and Treatments · Pediatric Urology and Nephrology Studies
Summary
- The present report describes a rare case of IC/HL which developed bilateral ureteral IC/HL‐like inflammation and stenosis in addition to the bladder lesions despite the preservation of bladder capacity, suggesting that IC/HL inflammation could extend to the upper urinary tract.
Introduction
1
Interstitial cystitis with Hunner lesion (IC/HL) is an enigmatic, chronic inflammatory disease of the urinary bladder, characterized histologically by pancystitis, epithelial denudation, stromal fibrosis and edema, and dense subepithelial lymphoplasmacytic infiltration [1, 2, 3, 4]. IC/HL occurs usually in the urinary bladder, with few documented cases involving the upper urinary tract, although the extremely contracted end‐stage IC/HL bladder has been found to cause vesicoureteral reflux (VUR) with or without hydronephrosis [5]. The present report describes the rare case of a Japanese woman with IC/HL who simultaneously developed IC/HL‐like bilateral ureteral inflammation, which led to ureteral stenosis and associated hydronephrosis.
Clinical Summary
2
A 51‐year‐old woman with no previous history of pelvic organ diseases presented to a local urology clinic in 2019 with intractable bladder/urethral pain that worsened at bladder filling. Clinical examination excluded other bladder diseases that possibly cause similar symptoms such as acute cystitis and bladder calculi. Cystoscopy showed a Hunner lesion (HL) at the posterior bladder wall, which was electrocauterized, and the patient was subsequently treated with intravesical dimethyl sulfoxide at the local clinical providers, but her symptoms did not resolve. Computed tomography (CT) after a series of these treatments showed the development of bilateral upper/mid ureteral narrowing accompanied by hydronephrosis. Her serum creatinine levels increased gradually over the next 2 years, and she was referred in 2021 to our department for further causal investigations and treatment of her refractory IC/HL symptoms and bilateral ureteral strictures. Demographic data at her initial visit are shown in the Table 1.
The frequency volume chart showed that the maximum voided urine volume was 200 mL, consistent with a well‐preserved bladder capacity for a Japanese woman. Blood tests showed a serum creatinine concentration of 1.24 mg/dL and an estimated glomerular filtration rate (eGFR) of 36.3 mL/min/1.73 m^2^, suggestive of mildly impaired renal function. Concentrations of anti‐double stranded DNA and anti‐SS‐A antibodies were slightly elevated, but there was no evidence of comorbid systemic autoimmune disorders, such as systemic lupus erythematosus (SLE) and Sjogren's syndrome after a thorough examination by specialists in rheumatology and nephrology including histological analysis of renal biopsied tissue. Ultrasonography and CT imaging showed bilateral proximal ureteral narrowing and associated dilation of the upper ureters and pelvis, but no obvious mass forming lesions in the retroperitoneal space. Cystoscopy revealed the presence of a HL on the posterior bladder wall (Figure 1). She underwent endoscopic fulguration of the HL with simultaneous bladder hydrodistension, retrograde pyelography, ureteroscopy, and implantation of bilateral ureteral stents under general anesthesia. Bladder capacity at a pressure of 80 cm H_2_O was 350 mL. A retrograde pyelogram showed bilateral proximal ureteral narrowing and associated hydronephrosis, with subsequent ureteroscopy revealing hyperplasia of the ureteral mucosa at the narrowing sites (Figure 2). Neither a bladder deformity nor VUR was observed. After surgery, the patient's irritable IC/BPS symptoms were resolved, and bilateral hydronephrosis disappeared, leading to the normalization of her renal function. Then, her ureteral lesions were treated with oral prednisolone (7.5 mg/day) for 2 years, followed by retrograde pyelography and ureteroscopy to evaluate these lesions. Despite the relief of IC/HL symptoms after endoscopic surgery, her bilateral ureteral stenosis and associated hydronephrosis were not resolved after 2 years of corticosteroid therapy and the ureteral stents in both ureters were left in place (Figure 2).
(A) Ultrasound imaging showing hydronephrosis of the (left image) right kidney and (right image) left kidney. (B) Computed tomography showing bilateral ureteral stenosis, as well as proximal ureteral strictures (arrows) with associated hydronephrosis in the bilateral upper urinary tract. (C) A Hunner lesion in the bladder.
(A) Retrograde pyelography before corticosteroid therapy. Arrows indicate the bilateral proximal ureteral strictures. (B) Ureteroscopy before corticosteroid therapy, showing mucosal hyperplasia and luminal narrowing in the (left image) right ureter and (right image) left ureter. (C) Retrograde pyelography after 2 years of corticosteroid therapy. Arrows indicate the remaining bilateral ureteral stenosis and associated hydronephrosis.
Pathological Findings
3
Histological examination of the bladder biopsy specimens obtained from both the HL and an area outside the HL showed chronic inflammatory changes compatible with IC/HL, such as subepithelial infiltration of inflammatory cells, primarily lymphoplasmacytic cells, stromal edema and fibrosis, hyperemia, and epithelial denudation (Figure 3A) [6, 7]. Biopsy specimens obtained from the narrowing sites of bilateral ureters showed chronic inflammatory changes similar to those of the bladder specimens, including epithelial denudation and infiltration of lymphoplasmacytic cells into the subepithelial layer (Figure 3B). These findings suggest that the pathomechanisms responsible for the pathophysiology of the bladder and ureteral lesions were similar in this case.
(A) Histology of bladder mucosal biopsies; (left image) the Hunner lesion, (right image) area outside the Hunner lesion. (B) Histology of ureteral lesions. Left image: Left ureter (original magnification, ×200), Middle image: Right ureter (original magnification, ×200), Right image: Enlarged image of the rectangular box in the middle image (original magnification, ×400).
Discussion
4
IC/HL has been reported to affect the entire bladder [8, 9], but the involvement of the upper urinary tract remains unclear. Results in the present patient, who developed bilateral ureteral IC/HL‐like inflammation and stenosis in addition to the bladder lesions despite the preservation of bladder capacity, suggest that IC/HL inflammation has involved the upper urinary tract.
IC/HL is an immune‐mediated inflammatory disease with a possible autoimmune nature [2, 3]. Epidemiologically, IC/HL is frequently accompanied by systemic autoimmune diseases such as SLE, Sjögren's syndrome, and Hashimoto's disease [4]. The elevated serum concentrations of autoantibodies, including anti‐SS‐A and anti‐double stranded DNA antibodies, in the present patient suggested the occurrence of other systemic autoimmune diseases. However, a thorough examination of this patient by specialists in rheumatology and nephrology resulted in no evidence of concurrent systemic autoimmune diseases, including SLE. Normal concentrations of the serum IgG4 antibodies and the absence of retroperitoneal fibrotic mass can negate the possible association of IgG4‐related disorders with ureteral stricture in this case. Taken together, these findings indicate that IC/HL alone was responsible for the elevated levels of serum autoantibodies and bilateral ureteral lesions in this case.
End‐stage IC/HL bladder can lead to bladder atrophy and deformity, with many of these patients experiencing bilateral/unilateral VUR and associated hydronephrosis [5]. To our knowledge, however, few studies have utilized ureteroscopy or histology to evaluate sporadic ureteral lesions potentially associated with IC/HL in bladders that were neither atrophied nor deformed. Findings in the present patient suggest that IC/HL could involve the upper urinary tract and impair kidney function at an earlier disease stage. Regular ultrasonographic or CT imaging follow‐up of upper urinary tracts in patients with IC/HL is warranted.
Low‐dose corticosteroid therapy was not effective in treating the ureteral lesions, although it sustained symptom relief after endoscopic elimination of the bladder lesions. Other immunosuppressants, including cyclosporine and tacrolimus, or more intensified prednisolone treatment, may be tested for the ureteral lesions of this case.
In conclusion, the present report describes a patient with IC/HL accompanied by bilateral ureteral stenosis and associated hydronephrosis. Histological assessment revealed chronic inflammatory changes in both the bladder and ureteral lesions compatible with those in typical IC/HL, suggesting that IC/HL inflammation had involved the upper ureters. Further investigations of additional patients are needed to clarify the pathomechanisms of unusual ureteral involvement in IC/HL.
Ethics Statement
The present study was approved by the Institutional Review Board of the University of Tokyo (approval no. 3124). Written informed consent for participation was obtained from the patient. All procedures were performed according to the principles of the Declaration of Helsinki.
Consent
All authors have read the entire manuscript and agreed to publication.
Conflicts of Interest
Tomonori Minagawa and Yusuke Sato are Editorial Board members of the International Journal of Urology and co‐authors of this article. To minimize bias, they were excluded from all editorial decision‐making related to the acceptance of this article for publication. Other authors declare no conflicts of interest with respect to the authorship and publication of this article.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Y. Homma , Y. Akiyama , J. H. Kim , et al., “Definition Change and Update of Clinical Guidelines for Interstitial Cystitis and Bladder Pain Syndrome,” Lower Urinary Tract Symptoms 16 (2024): e 12532.39267358 10.1111/luts.12532 · doi ↗ · pubmed ↗
- 2Y. Akiyama , K. Harada , J. Miyakawa , et al., “Th 1/17 Polarization and Potential Treatment by an Anti‐Interferon‐Gamma DNA Aptamer in Hunner‐Type Interstitial Cystitis,” i Science 26 (2023): 108262.38026177 10.1016/j.isci.2023.108262 PMC 10663743 · doi ↗ · pubmed ↗
- 3Y. Akiyama , K. Sonehara , D. Maeda , et al., “Genome‐Wide Association Study Identifies Risk Loci Within the Major Histocompatibility Complex Region for Hunner‐Type Interstitial Cystitis,” Cell Reports Medicine 4 (2023): 101114.37467720 10.1016/j.xcrm.2023.101114 PMC 10394254 · doi ↗ · pubmed ↗
- 4Y. Akiyama , Y. Luo , P. M. Hanno , D. Maeda , and Y. Homma , “Interstitial Cystitis/Bladder Pain Syndrome: The Evolving Landscape, Animal Models and Future Perspectives,” International Journal of Urology: Official Journal of the Japanese Urological Association 27 (2020): 491–503.32246572 10.1111/iju.14229 PMC 7768977 · doi ↗ · pubmed ↗
- 5Y. Akiyama , A. Niimi , Y. Igawa , et al., “Cystectomy for Patients With Hunner‐Type Interstitial Cystitis at a Tertiary Referral Center in Japan,” Lower Urinary Tract Symptoms 14 (2022): 102–108.34704374 10.1111/luts.12416 · doi ↗ · pubmed ↗
- 6S. L. Johansson and M. Fall , “Clinical Features and Spectrum of Light Microscopic Changes in Interstitial Cystitis,” Journal of Urology 143 (1990): 1118–1124.2342171 10.1016/s 0022-5347(17)40201-1 · doi ↗ · pubmed ↗
- 7Y. Akiyama , Y. Homma , and D. Maeda , “Pathology and Terminology of Interstitial Cystitis/Bladder Pain Syndrome: A Review,” Histology and Histopathology 34 (2019): 25–32.30015351 10.14670/HH-18-028 · doi ↗ · pubmed ↗
- 8D. Maeda , Y. Akiyama , T. Morikawa , et al., “Hunner‐Type (Classic) Interstitial Cystitis: A Distinct Inflammatory Disorder Characterized by Pancystitis, With Frequent Expansion of Clonal B‐Cells and Epithelial Denudation,” P Lo S One 10, no. 11 (2015): e 0143316, 10.1371/journal.pone.0143316.26587589 PMC 4654580 · doi ↗ · pubmed ↗