Balancing risks of surgical complications and positive margins for patients with invasive lobular carcinoma of the breast and elevated BMI: An institutional cohort study
Israel Falade, Kayla Switalla, Astrid Quirarte, Molly Baxter, Daniel Soroudi, Harriet Rothschild, Shoko Emily Abe, Karen Goodwin, Merisa Piper, Michael Alvarado, Bao-Quynh Julian, Cheryl Ewing, Jasmine Wong, John Rose, Laura Esserman, Robert Foster, Rita A. Mukhtar

TL;DR
This study examines how to balance surgical complication risks and positive margin rates in breast cancer patients with high BMI and invasive lobular carcinoma.
Contribution
The study identifies optimal surgical approaches for ILC patients with elevated BMI by analyzing complication and margin rates.
Findings
Oncoplastic surgery reduced positive margin rates in breast-conserving surgery (BCS) for ILC patients.
Simple mastectomy had the lowest complication rate among surgical approaches analyzed.
BCS had significantly higher positive margin rates compared to mastectomy.
Abstract
The risks of postoperative complications in breast cancer patients vary by patient and tumor characteristics. Elevated BMI and invasive lobular carcinoma (ILC) increase risks of surgical complications and positive margins, respectively. We retrospectively analyzed patients with BMI ≥30 kg/m2 from an institutional ILC database. The primary outcome was surgical complication rate by procedure type. The secondary outcome was positive margin rates by surgical approach, stratified by T stage. Of 154 analyzed patients, standard BCS, lumpectomy with oncoplastic closure, and simple mastectomy had the lowest complication rates (18.2 %, 17.0 %, 11.8 %). Oncoplastic reduction mammoplasty and mastectomy with aesthetic closure had the highest rates (35.5 %, 33.3 %). The overall positive margin rate was 28.5 %, significantly higher in BCS vs. mastectomy (37.4 % vs. 15.0 %, p = 0.003). Oncoplastic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
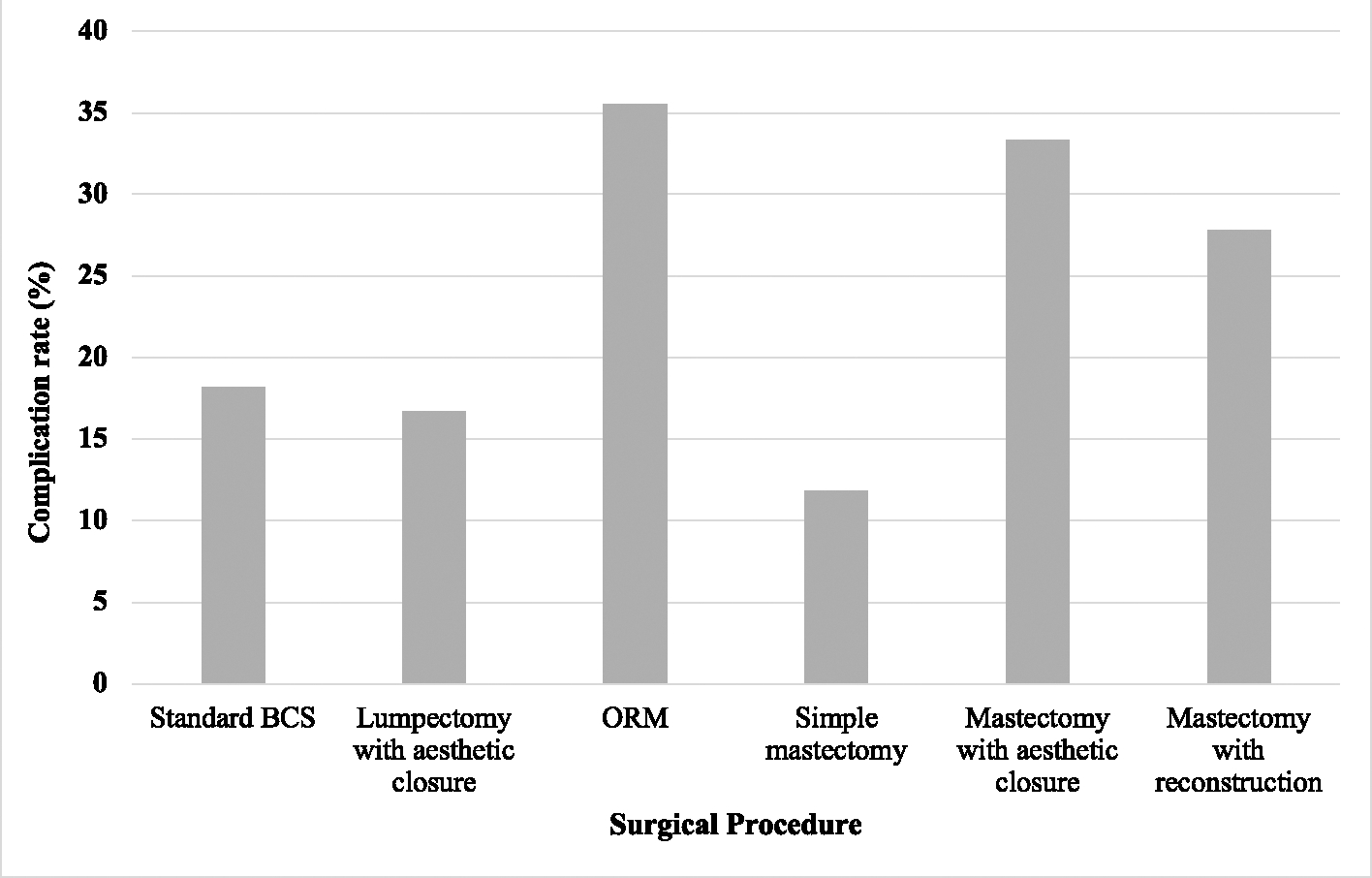 Figure 1
Figure 1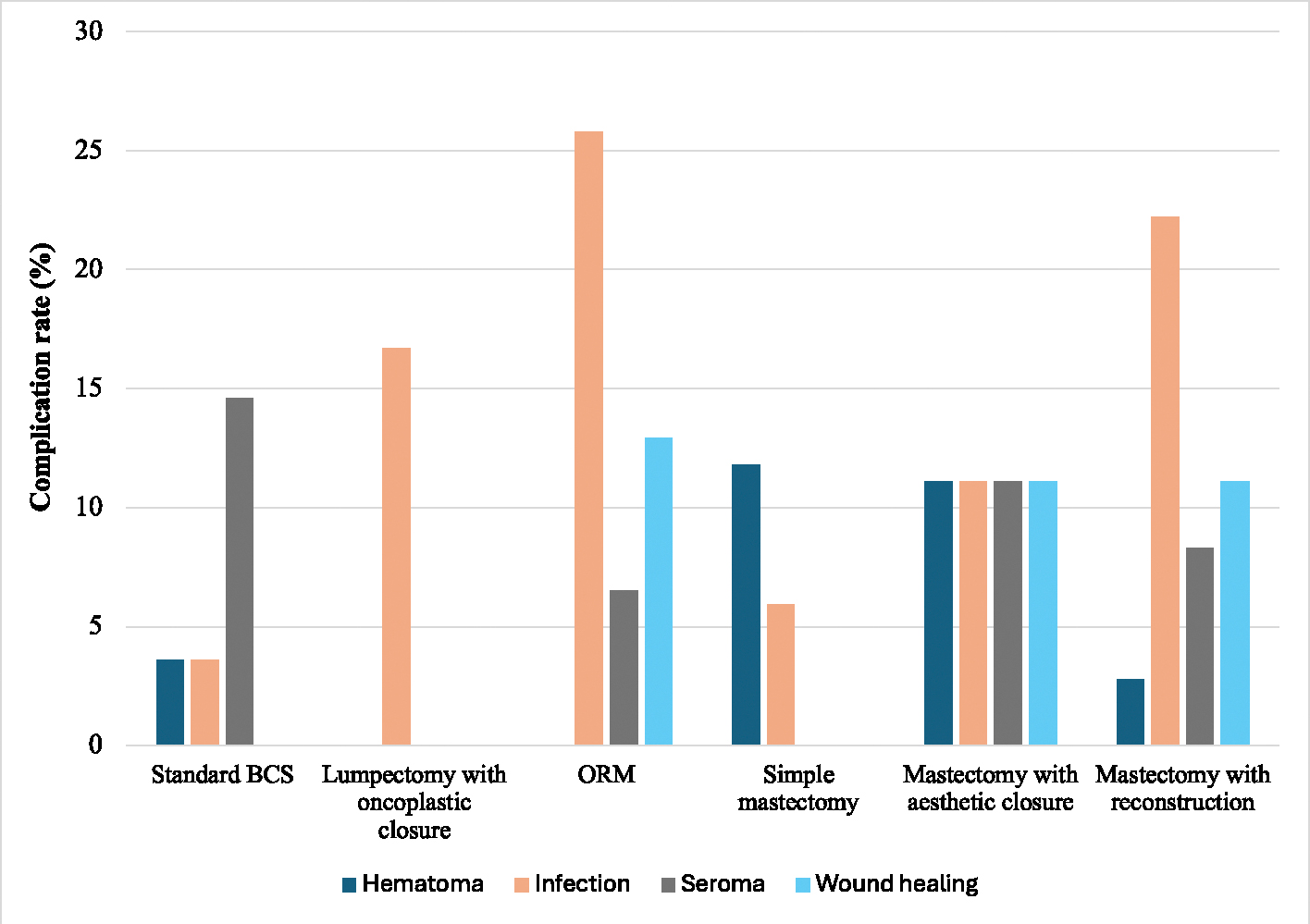 Figure 2
Figure 2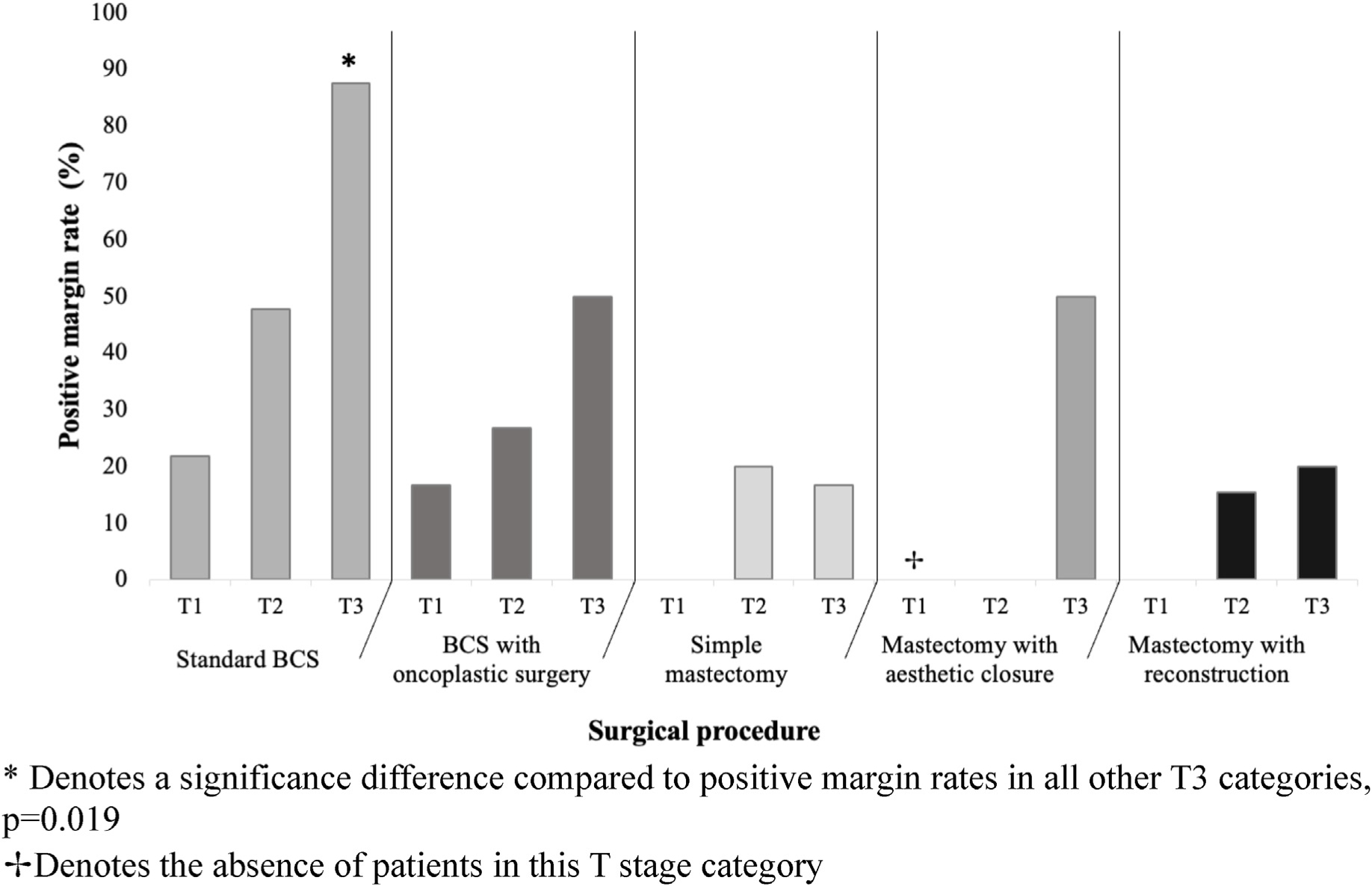 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreast Cancer Treatment Studies · Cancer Risks and Factors · Breast Implant and Reconstruction
Introduction
Patients diagnosed with breast cancer must make several decisions regarding treatment, including selecting the type of surgery to undergo. Surgical resection of the primary tumor remains an important component of breast cancer treatment, with the two main surgical options being breast conservation (also known as lumpectomy), or mastectomy.^1^ Within these broad categories exist additional variations: patients can undergo standard breast conserving surgery (BCS), or alternatively combine BCS with oncoplastic approaches to improve the aesthetic outcome. For those undergoing mastectomy, options include simple mastectomy without reconstruction, mastectomy with aesthetic flat closure, or mastectomy with reconstruction (which may be implant or tissue based).^2^(see Table 1 )
Two of the main early outcomes to consider when gauging the effectiveness of breast cancer surgery include positive margin rates, and surgical complication rates.^3^ While more extensive surgery such as mastectomy can reduce the risk of positive margins, it may result in increased risk of other surgical complications.^4^ The pros and cons of each surgical choice vary based on both patient factors and tumor specific factors.
For patients with elevated body mass index (BMI), which impacts approximately 42 % of the population, the risk of surgical complications across a wide array of procedures is elevated.^5^ Indeed, many reconstructive procedures are not offered above certain BMI thresholds due to data showing increased surgical complications.^6^ Data show that breast cancer patients with BMI above 30 kg/m^2^ are less likely to undergo reconstruction after mastectomy, and obesity has been viewed as a potential contraindication to breast reconstruction.^7,8^
Tumor type can also influence surgical outcomes. For example, patients with the second most common type of breast cancer, invasive lobular carcinoma (ILC), face elevated risk of positive margins at surgical resection.^9^ Comprising 10–15 % of all breast cancer diagnoses, ILC grows in a diffuse pattern due to its characteristic absence of the adhesion protein E-cadherin.^10^ Several studies report that the risk of positive margins following BCS can exceed 40 % in patients with ILC.^11–14^ We and others have shown that the addition of oncoplastic surgery to BCS may reduce the risk of positive margins in those with ILC, but the impact of adding such techniques on other surgical complications for these patients is unknown.^15,16^
For these reasons, surgical decision making for women with ILC and elevated BMI is especially challenging, with no published data to our knowledge reporting outcomes in this group specifically. We therefore evaluated an institutional cohort of patients with ILC and BMI ≥30 kg/m^2^ and determined the incidence of surgical complications and positive margin rates by type of breast surgery performed. The goal of this analysis is to provide data for surgeons and patients that may help inform surgical decision making when balancing the risks and benefits of various surgical approaches.
Methods
Study design and data collection
2.1.
We retrospectively selected a cohort of consecutive patients with a BMI ≥30 kg/m^2^ from a prospectively maintained institutional database of patients undergoing surgical treatment for ILC between 1995 and 2023. The BMI threshold was selected based on the World Health Organization definition of obesity.^17^ Patients were excluded if they had de novo stage IV disease, lacked BMI data at the time of surgery, or did not undergo surgical treatment. This retrospective study was approved by the University of California, San Francisco Institutional Review Board (IRB).
Clinicopathological information including tumor size, tumor (T) category, BMI, type of surgical operation, use of oncoplastic surgery, use of shave margins, and rate of positive surgical margins were collected from the database. Patients were grouped by initial breast surgery procedure performed, as either BCS or mastectomy. Within the BCS group, patients were further categorized as undergoing standard BCS, or BCS with oncoplastic surgery (either oncoplastic closure or oncoplastic reduction mammoplasty [ORM]). Within the mastectomy group, patients were categorized as undergoing simple mastectomy (mastectomy without reconstruction), mastectomy with aesthetic flat closure, or mastectomy with reconstruction (skin sparing [SSM] or total/nipple sparing [TSSM]) with either implant based or autologous reconstruction. Mastectomy with aesthetic flat closure was defined as the removal of extra skin and fat after the mastectomy, followed by shaping and smoothing the remaining tissue to create a flat chest contour (performed by a plastic surgeon in this cohort). Procedure type was determined by review of operative reports. The use of shave margins was determined by review of pathology reports, with resection of any additional margin being considered a shave margin. Of note, routine cavity shave margin use has been recommended at our institution for patients with ILC undergoing BCS since 2018; use of shave margins at the time of mastectomy is performed selectively per preference of the treating surgeon.
The primary outcome was the rate of surgical complications for each procedure type overall and stratified by T category. Surgical complications included any of the following occurrences diagnosed within 6 months of primary breast surgery: infection, seroma, hematoma, poor wound healing, or unplanned return to the operating room. The presence of surgical complications was determined from review of the medical record and provider notes. Infection was defined by documentation in the medical record of “infection,” “abscess,” “breast cellulitis,” “infected implant,” or “donor site infection” and treatment with antibiotics.
Seroma and hematoma were defined as complications if a healthcare provider documented seroma or hematoma as a clinical diagnosis, irrespective of subsequent interventions for management. Poor wound healing included documentation of “skin flap necrosis,” “muscle flap necrosis,” “incisional breakdown,” “non-healing wound,” or “wound dehiscence” in post-operative hospital visit records. An unplanned return to the operating room was defined as any additional procedure required for a complication resulting directly or indirectly from the primary operation.
The secondary outcome was positive margin rate by type of surgical procedure. Margins were considered positive if pathologic evaluation of final margins indicated “ink on tumor.” Additional outcomes evaluated included total number of oncologic operations performed for primary tumor and their associated complication rates.
Statistical analysis
2.2.
Patient and tumor characteristics were compared by procedure type using t-tests and Pearson’s chi-square tests. We used summary statistics to evaluate complication rates and positive margin rates. Chi-square tests were used to analyze the associations between surgical procedure type and complication rates, as well as positive margin rates. Averaged total number of operations and complications for each patient were compared across surgical procedures using ANOVA. Logistic regression models were developed to evaluate predictors of surgical complications and positive margins. All analyses were performed using STATA 18.0 (Stata Corp., College Station, TX, USA), with two-tailed p < 0.05 indicative of statistical significance.
Results
Overall demographics
3.1.
Of 804 ILC patients in the institutional database, we identified a cohort of 154 patients with stage I-III ILC and BMI ≥30 kg/m^2^. Patients in this cohort underwent their initial surgical procedures between 1999 and 2023. Average age was 62.9 α 11.6 years and average BMI was 34.9 kg/m^2^ (range 30.0–61.4 kg/m^2^). Most patients (55.6 %) had stage 2 disease, 86.0 % had hormone receptor (HR) positive and human epidermal growth factor receptor-2 (HER2) negative tumors, and 68.9 % had grade 2 tumors.
Overall, 92 patients (59.7 %) underwent BCS and 62 (40.3 %) underwent mastectomy as their first oncologic operation. Specifically, 35.7 % (n = 55) underwent standard BCS, 24.0 % (n = 37) underwent BCS with oncoplastic surgery (6 with oncoplastic closure and 31 with ORM), 11.0 % (n = 17) underwent simple mastectomy, 5.8 % (n = 9) underwent mastectomy with aesthetic flat closure, and 23.4 % (n = 36) underwent mastectomy with reconstruction (19 with SSM and 17 with TSSM). Among those who underwent SSM or TSSM, 75.0 % (n = 27) had tissue expanders and 25 % (n = 9) had immediate autologous reconstruction. Patients who underwent BCS as their first operation had significantly smaller tumor size compared to those who underwent mastectomy (mean 3.0 cm versus 5.1 cm, p < 0.01), but did not otherwise significantly differ in age, BMI, or ILC tumor grade. Shave margin use was common in this study cohort, with shave margins utilized in 76.5 % of patients undergoing BCS and 43.5 % of patients undergoing mastectomy. The use of oncoplastic and reconstructive approaches increased over time (p = 0.004), but there was no difference in complication rates or positive margins rates by time period.
Complication rates by procedure type
3.2.
In this cohort of 154 patients with ILC and elevated BMI, 20.8 % of patients had one complication after their first oncologic procedure, while 9.1 % had more than one complication. Of these, the most common complication was infection, occurring in 13.6 % of patients, followed by seroma (9.1 %), poor wound healing (5.8 %), unplanned return to the operating room (5.8 %), and hematoma (3.9 %). Of those with seromas, 20 % required aspiration while the remaining were managed expectantly; for those with hematomas, 66.7 % underwent intervention. The overall complication rates in the BCS and mastectomy groups were 23.9 % and 24.2 % respectively.
Among BCS patients, while the complication rate was numerically higher in those undergoing ORM, there was no significant difference in overall complication rates between standard BCS, BCS with oncoplastic closure, and ORM (18.2 %, 16.7 %, and 35.5 %, p = 0.259) (Fig. 1). In the ORM group, surgical site infection was the most common complication, occurring in 25.8 % of cases, with wound healing complications being the second most common at 12.9 % (Fig. 2).
Among mastectomy patients, there was no statistically significant difference in overall complication rate between simple mastectomy, mastectomy with aesthetic flat closure, and mastectomy with reconstruction (11.8 %, 33.3 %, and 27.9 % respectively, p = 0.064) (Fig. 1). When further stratifying the cohort of patients with mastectomy with reconstruction, SSM had a higher overall complication rate compared to TSSM, simple mastectomy, and mastectomy with aesthetic closure (42.1 % vs 11.8 %, 11.8 %, and 33.3 %, p = 0.085). Of note, autologous reconstruction was more common in the SSM group than the TSSM group (42.1 % versus 5.9 %). Notably, one patient with autologous reconstruction experienced tissue flap necrosis following mastectomy with reconstruction, and one patient with implant-based reconstruction experienced skin flap necrosis following mastectomy with reconstruction. Both of these complications were categorized as “wound healing” complications. Furthermore, among SSM and TSSM patients, immediate placement of a tissue expander was associated with a numerically but not significantly lower overall complication rate compared to those who underwent immediate autologous reconstruction (22.2 % versus 44.4 %, p = 0.197).
Across all procedures, 15 patients required at least one unplanned reoperation due to surgical complications. Among these patients, the average number of reoperations was 1.75 (range 1–6 reoperations). Patients who underwent BCS as their initial oncologic procedure were significantly less likely to require subsequent reoperations compared to patients who underwent mastectomy (3.3 % versus 19.4 %, p = 0.001). In particular, patients who initially underwent mastectomy with reconstruction accounted for 66.7 % of all unplanned reoperations.
Patients who underwent standard BCS, lumpectomy with oncoplastic closure, or simple mastectomy had the lowest complication rates (18.2 %, 16.7 %, and 11.8 %, respectively), while patients undergoing ORM, mastectomy with aesthetic closure, and SSM had the highest complication rates (35.5 %, 33.3 %, and 42.1 % respectively). Overall complication rates between procedures did not significantly differ by T stage. There was a significantly higher complication rates in patients who underwent any type of oncoplastic surgery or immediate reconstruction compared to those who did not undergo oncoplastic or reconstructive surgery (30.5 % versus 16.7 %, p = 0.045).
In a multivariate logistic regression model adjusting for age, shave margins, tumor stage, type of breast surgery (mastectomy versus BCS), use of oncoplastic surgery, presence of diabetes mellitus, and BMI, increased BMI was associated with a higher likelihood of post-operative complications (odds ratio = 1.84, 95 % confidence interval [1.21–2.8], p = 0.004).
Positive margin rates by procedure type and T category
3.3.
Margin data was available in 151 of 154 initial oncologic procedures. Of those, 43 cases (28.5 %) had positive margins. Across all procedure types, standard BCS had the highest rate of positive margins (42.6 %). The positive margin rate was significantly higher in patients who underwent standard BCS compared to those who underwent BCS with oncoplastic surgery, simple mastectomy, mastectomy with aesthetic flat closure, or mastectomy with immediate reconstruction (42.6 % versus 29.7 %, 13.3 %, 22.2 %, and 13.9 % respectively, p = 0.027). This difference was most notable among patients with T3 tumor category (Fig. 3). Overall, positive margin rates were significantly higher in patients who underwent any type of BCS compared to any type of mastectomy (37.4 % vs 15.0 %, p = 0.003). Shave margin use was not associated with lower positive margin rates among BCS patients.
On multivariate analysis of patients undergoing BCS, the use of oncoplastic surgery was significantly associated with reduced odds of positive margins when adjusting for patient age and tumor stage (odds ratio for oncoplastic surgery 0.3, 95 % confidence interval [0.1–0.9], p = 0.035).
Rates of subsequent oncologic procedures and associated complications
3.4.
A total of 41 patients (26.6 %) underwent a second oncologic procedure. Among BCS patients, 34 (37.0 %) underwent a second oncologic procedure, and 5 patients required a third. Among mastectomy patients, only 7 patients (11.3 %) underwent a second oncologic operation, with none proceeding to a third.
The overall complication rate for all second oncologic operations was 14.6 %, with no significant difference in complication rates between patients who underwent BCS and those who had a mastectomy for their second oncologic procedure (7.7 % versus 26.7 %, p = 0.098).
Infection was the most common complication, occurring in 12.2 % of all second operations. Seroma and wound healing complications each accounted for 2.4 % of complications across all second operations, while hematoma did not occur in any cases. Among the 5 cases requiring a third operation, 1 case (20.0 %) was complicated by infection.
Of all BCS patients who underwent a second or third operation, 18 (52.9 %) ultimately underwent completion mastectomy for their final procedure, while 16 (47.1 %) underwent re-excision as their final procedure. For all mastectomy patients who underwent second operation, 6 (85.7 %) underwent re-excision, and 1 (14.3 %) underwent re-excision of nipple areolar complex with conversion to mastectomy and aesthetic flat closure due to residual disease.
Total number of operations
3.5.
On average, patients underwent 1.7 total operations, encompassing all oncologic and additional reconstructive operations. The average number of oncologic operations was 1.3, and was significantly higher in the BCS group compared to the mastectomy group (1.4 versus 1.1, p < 0.001). The average number of oncoplastic/reconstructive operations was 0.4, and was lower in the BCS group compared to the mastectomy group (0.2 versus 0.7, p < 0.001). When evaluating the proportion of patients who had three or more total operations of any type, this proportion was significantly higher in those whose initial oncologic procedure was a mastectomy with reconstruction, in comparison to those who had standard BCS, lumpectomy with oncoplastic closure/ORM, simple mastectomy, or mastectomy with aesthetic flat closure (36.1 % versus 18.2 %, 8.1 %, 0 %, and 0 %, respectively, p = 0.002).
Discussion
These results demonstrate significant challenges with surgical management of ILC for those with BMI≥30 kg/m^2^, a group representing a high proportion of the population. Standard BCS was associated with lower risk of early surgical complications compared to BCS with oncoplastic approaches, but higher rates of positive margins. For those undergoing mastectomy, surgical complications were more common in patients undergoing mastectomy with reconstruction, particularly in the SSM group, where the higher rate of autologous reconstruction most likely contributed to the increased complication rates.
Patients with obesity who are diagnosed with breast cancer face undergoing oncologic surgery without time for pre-operative weight optimization. Because of increased risks of surgical complications in the setting of BMI≥30 kg/m^2^, surgical choices may be more limited. Indeed, the literature is replete with studies showing the association between elevated BMI and surgical complications, most notably after reconstructive procedures.^7,18–27^
Our rate of complications in this population of patients with stage I-III breast cancer and BMI≥30 kg/m^2^ is similar to those reported in the literature. In the setting of BCS, we found that 23.9 % had complications. Although data are limited, one study reported a 40 % complication rate among 199 patients with a BMI over 30 kg/m^2^ who underwent oncoplastic breast reduction. Similarly, another study of 182 patients that received bilateral reduction mammoplasty reported an overall complication rate of 51 %.^28,29^
For those undergoing mastectomy, our overall complication rate of 22.6 % is also consistent with prior studies. Complication rates for those undergoing mastectomy in the setting of BMI ≥30 kg/m^2^ range from as low as 7.5 % for simple mastectomy, to 26.5 % in those undergoing reconstruction.
Interestingly, the small number of patients in our series who underwent aesthetic flat closure had a higher complication rate than we expected, as well as a higher positive margin rate. This is a procedure in which there is growing interest, which involves de-epithelialization and rotation of skin flaps to create an aesthetic chest wall contour. In our population, 33 % of patients experienced a post-operative complication; in a previously published series of 10 patients with morbid obesity who underwent this procedure 40 % had wound healing complications.^30^ The high positive margin rate seen in patients with T3 ILC raises the question of the oncologic safety of this procedure in this population, and whether preservation of skin for chest wall contouring inadvertently resulted in retained breast tissue; with only 9 patients we cannot draw conclusions, but our results suggest the need for further study into aesthetic flat closure for patients with large ILC tumors.
Although we found that oncoplastic and reconstructive procedures were associated with higher rates of surgical complications compared to standard BCS or simple mastectomy, these findings must be balanced with the risk of positive margins. For patients undergoing BCS, there was a strong association between oncoplastic surgery and lower risk of positive margins. Among those undergoing mastectomy, however, simple mastectomy (without aesthetic closure or reconstruction) was associated with the lowest risk of positive margins. There are limited data in the literature to compare these findings; our prior analysis of this ILC database (including all BMI groups) found no difference in positive margin rates by type of mastectomy.^31^ However, in that analysis we did not identify patients who had aesthetic flat closure specifically, but rather grouped them with mastectomy without reconstruction. Whether the preservation of skin and soft tissue in aesthetic flat closure leads to increased risk of positive margins for those with ILC deserves further attention and study.
In our study, a high proportion of patients had shave margins taken during both BCS and mastectomy procedures. While we previously showed that shave margin use was associated with reduced positive margins in patients with ILC, we did not observe this relationship in this analysis.^32^ The high rates of positive margins despite the use of shave margins reflect the challenges of surgical resection for diffusely growing tumors like ILC where imaging often underestimates tumor size. Studies have reported positive margin rates as high as 60 % following BCS for ILC, with one study by Wanis et al. demonstrating re-excision rates around 35.1 % for positive or close margins.^9,13,14,33,34^ In mastectomy cases, the literature suggests positive margin rates ranging from 3 to 27 % depending on the definition of margin width utilized.^35–40^ In our study, patients who underwent BCS had a positive margin rate of 37.4 %, compared to 15.0 % in those who underwent mastectomy. Notably, 19.6 % of the BCS population had T3 tumors, a tumor size which is traditionally considered a contraindication to breast conservation. This may have contributed to higher positive margin rates.
When evaluating surgical complications and positive margin rates in isolation, our study would suggest that simple mastectomy may be the optimal surgical procedure for patients with ILC and BMI ≥30 kg/m^2^. However, several other factors influence surgical decision making, including patient preference.
Advantages of BCS include avoidance of mastectomy, and the impact of post-mastectomy radiotherapy on a reconstructed breast, which is associated with risk of complications particularly for those undergoing implant-based reconstruction. Additionally, we saw that unplanned returns to the operating room were less common in those undergoing BCS.
While these surgical complications are unlikely to be related to the histologic subtype of breast cancer, the risk of positive margins is known to be elevated in ILC specifically. As such, for those with this tumor type, surgical decision making must include considerations of patient preferences for breast conservation, risk of positive margins associated with each surgical approach, as well as risk of surgical complications. Despite the risk of surgical complications, with post-operative infection requiring antibiotics being the most common, we feel that BCS with oncoplastic approaches still provides a reasonable choice for patients with ILC and BMI ≥30 kg/m^2^ given its association with lower positive margin rates and avoidance of mastectomy.
Our study showed an increased risk for positive margins across all procedure types for patients with higher T stage, particularly pronounced for those undergoing BCS. However, we observed a significant reduction in the risk of positive margins among BCS patients when ORM or oncoplastic approach was used. Previous research from our institution has also demonstrated that ORM yields comparable positive margin rates and overall outcomes compared to mastectomy.^32^ This suggests that employing an oncoplastic approach with BCS may be a preferable option for patients with T1-T2 ILC, especially those with elevated BMI. Conversely, we found that T3 stage disease exhibited the highest positive margin rates with BCS procedures, ranging from 50 to 87.5 % for lumpectomy and lumpectomy with oncoplastic approaches. These findings align with existing literature, which have consistently demonstrated the high likelihood of positive margins when attempting BCS in patients with T3 disease.^41^ Thus, for T3 cases, some may consider mastectomy a more suitable choice but the high risk of positive margins still persists, reflecting the growth pattern of these tumors. Accordingly, well-informed patients may still opt for BCS with oncoplastic surgery over mastectomy even in setting of T3 tumor.
While we were unable to evaluate the impact of radiation on outcomes, the growing indications for post-mastectomy radiation should also be considered for those with larger tumors, who may experience higher rates of complications if radiotherapy is received after mastectomy with reconstruction versus after BCS with oncoplastic surgery.
Limitations and future directions
4.1.
Given the retrospective nature of this study we recognize the inherent potential for selection bias and incomplete data capture. The single institution design may also limit the generalizability of our findings to broader populations. Furthermore, the limited sample size in certain subgroups may have reduced our ability to detect statistical differences. Another potential limitation of this study is the extended data collection period, which may capture evolving surgical practices. At our institution, oncoplastic techniques were primarily adopted after 2000, with an increase over time in its use. Although the large time period introduces heterogeneity, these operations were performed by a small group of plastic surgeons, with no major changes to the institutional approach during the study period. Lastly, the absence of a comparison group of patients with lower BMI in our study design prevents direct comparisons, limiting our ability to explore distinctions between individuals with elevated and lower BMI. However, given the lack of research on surgical complications specifically in ILC patients with elevated BMI, we believe that our results represent an important piece of evidence to assist in optimizing outcomes for this patient population.
Conclusion
In this cohort of ILC patient with elevated BMI, we found that 23.4 % experienced a surgical complication after their first oncologic surgery, with a higher risk in those who underwent oncoplastic surgery or immediate reconstruction. Although BCS procedures had the highest positive margin rates, these rates were significantly reduced when ORM was utilized as the BCS procedure. Simple mastectomy had the lowest overall complication rate and positive margin rate, yet this procedure may not align with patient goals for breast conservation or reconstruction. Finally, patients who underwent mastectomy with immediate reconstruction as their first oncologic surgery had significantly more subsequent operations and unplanned reoperations on average compared to other initial procedures. These findings should be used for shared decision making to help patients with ILC and elevated BMI select the surgical procedure that most aligns with their goals and preferences.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Czajka ML, Pfeifer C. Breast cancer surgery. In: Stat Pearls. Stat Pearls Publishing; 2024. http://www.ncbi.nlm.nih.gov/books/NBK 553076/. Accessed March 13, 2024.31971717 · pubmed ↗
- 2Hammer C, Fanning A, Crowe J. Overview of breast cancer staging and surgical treatment options. Cleve Clin J Med. 2008;75(Suppl 1):S 10–S 16. 10.3949/ccjm.75.suppl_1.s 10.18457192 · doi ↗ · pubmed ↗
- 3Mohamedahmed AYY, Zaman S, Zafar S, Comparison of surgical and oncological outcomes between oncoplastic breast-conserving surgery versus conventional breast-conserving surgery for treatment of breast cancer: a systematic review and meta-analysis of 31 studies. Surg Oncol. 2022;42:101779. 10.1016/j.suronc.2022.101779.35567982 · doi ↗ · pubmed ↗
- 4de Boniface J, Szulkin R, Johansson ALV. Medical and surgical postoperative complications after breast conservation versus mastectomy in older women with breast cancer: Swedish population-based register study of 34 139 women. Br J Surg. 2023;110(3):344–352. 10.1093/bjs/znac 411.36511352 PMC 10364521 · doi ↗ · pubmed ↗
- 5Bryan S, Afful J, Carroll M, NHSR 158. National Health and Nutrition Examination Survey 2017–March 2020 Pre-pandemic Data Files. National Center for Health Statistics (U.S.); 2021. 10.15620/cdc:106273.PMC 1151374439380201 · doi ↗ · pubmed ↗
- 6Lee K, Kruper L, Dieli-Conwright CM, Mortimer JE. The impact of obesity on breast cancer diagnosis and treatment. Curr Oncol Rep. 2019;21(5):41. 10.1007/s 11912-019-0787-1.30919143 PMC 6437123 · doi ↗ · pubmed ↗
- 7Srinivasa DR, Clemens MW, Qi J, Obesity and breast reconstruction: complications and patient-reported outcomes in a multicenter, prospective study. Plast Reconstr Surg. 2020;145(3):481e–490e. 10.1097/PRS.0000000000006543.32097295 · doi ↗ · pubmed ↗
- 8Cevallos P, Berry C, Lipman KJ, Breast reconstruction after mastectomy in patients with obesity: a narrative review. Ann Transl Med. 2023;11(12):413. 10.21037/atm-23-1599.38213816 PMC 10777214 · doi ↗ · pubmed ↗