Navigating Diagnostic Challenges: An Uncommon Case of Jejunal Leiomyoma With Intussusception and Acute Gastrointestinal Bleeding
Pedro Popoutchi, Pedro Averbach, Caroline Cirenza, Marcelo Averbach

TL;DR
A rare case of jejunal leiomyoma causing acute gastrointestinal bleeding and intussusception is reported, emphasizing the need for thorough investigation in similar cases.
Contribution
This case report highlights the diagnostic challenges and clinical presentation of an uncommon jejunal leiomyoma.
Findings
A 48-year-old male presented with acute gastrointestinal bleeding due to a jejunal leiomyoma.
Diagnostic imaging and endoscopy were essential in identifying the subepithelial lesion.
Histopathology confirmed the lesion as a jejunal leiomyoma following enterectomy.
Abstract
This case report aims to describe an uncommon occurrence of jejunal leiomyomas, highlighting the clinical presentations, diagnostic challenges and therapeutic interventions. A 48-year-old male patient with a history of a jejuno-jejunal intussusception treated conservatively presented two years later with dark, maroon-colored stools and a hemoglobin of 6.8 g/L. Gastrointestinal upper endoscopy and colonoscopy showed no alterations that could justify the event. Endoscopic capsule revealed an ulcerated subepithelial lesion in the proximal jejunum. Abdominal CT scan indicated a 4.6-cm mesenchymal lesion (likely gastrointestinal stromal tumor (GIST) or leiomyoma) in the jejunum. It was chosen to proceed with enterectomy due to the severity of the bleeding. At the time of the operation, the histopathological characteristics of the jejunal lesion were not definitively known but histopathology…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2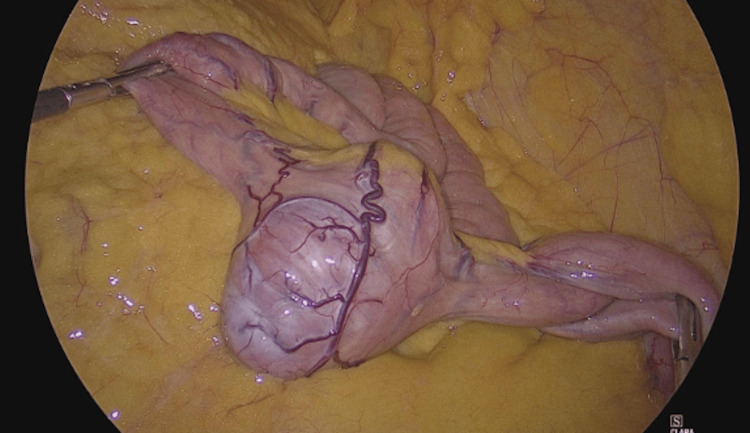 Figure 3
Figure 3 Figure 4
Figure 4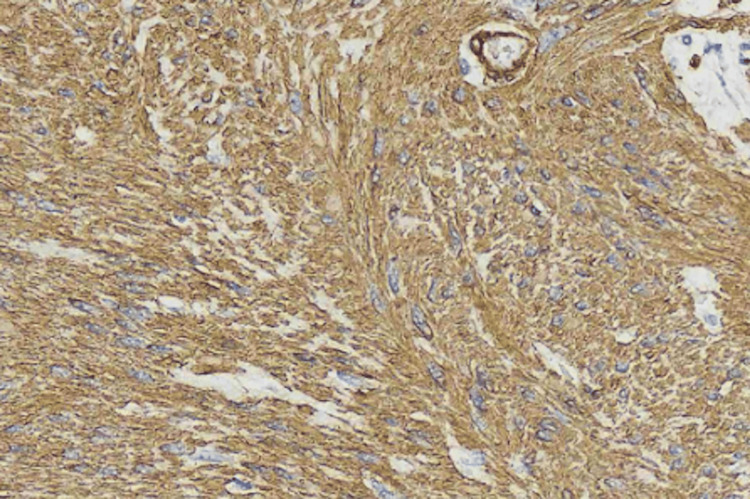 Figure 5
Figure 5| Material | Marker | Antibody | Result |
| Tumor/mucosae | Anti-C-KIT | EP 10 clone / Ventana | Negative |
| Tumor/mucosae | Anti-DOG1 | SP31 clone / Ventana | Negative |
| Tumor/mucosae | Anti-smooth muscle actin | HUC1-1 clone / Ventana | Positive |
| Tumor/mucosae | Anti-desmin | DE-R-11 clone / Ventana | Positive |
| Tumor/mucosae | Anti-S100 | Policlonal / Ventana | Negative |
| Tumor/mucosae | Anti-CD34 | QBEnd /10 clone / Ventana | Negative |
| Tumor/mucosae | Anti-Ki-67 | MIB-1 clone / Dako | Positive in 1%-2% of the neoplastic cells |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal disorders and treatments · Gastrointestinal Tumor Research and Treatment
Introduction
Leiomyomas, benign smooth muscle tumors, are rarely found in the small intestine, with jejunal leiomyomas being particularly uncommon [1]. This case report describes an unusual presentation of a jejunal leiomyoma, initially manifesting as jejuno-jejunal intussusception and later as acute gastrointestinal bleeding - a clinical scenario not typically associated with this tumor type [2, 3]. The rarity of such a presentation presents diagnostic challenges and highlights the importance of maintaining a high index of suspicion in cases of unexplained gastrointestinal bleeding. This report aims to explore the clinical, diagnostic, and therapeutic aspects of managing jejunal leiomyomas, particularly when presenting with acute bleeding, and to contribute to the limited literature on this rare condition.
Case presentation
A 48-year-old male patient from São Paulo, Brazil, presented to the emergency department in December 2023, with a one-month history of dark maroon stools occurring twice daily, fatigue, and pallor. He denied fever, chills, nausea, vomiting, chest pain, or shortness of breath.
His medical history included a 2021 bicycle accident, resulting in multiple fractures and cranial trauma. He underwent surgical reduction of a clavicular fracture and subsequently developed nausea and vomiting, initially attributed to post-traumatic gastroparesis. An abdominal CT scan with contrast at that time revealed jejuno-jejunal intussusception, which was managed conservatively. He was also on medications for depression, attention-deficit hyperactivity disorder (ADHD), and dyslipidemia, and had a history of renal calculi. His family history included a paternal grandfather with intestinal cancer and a father with esophageal cancer.
On examination, he was hemodynamically stable and had a normal abdominal exam. Lab results showed a hemoglobin of 6.8 g/dL (reference value 11.7 to 14.9 g/dL) and a hematocrit of 23.9% (reference value 35.1% to 44.1%), compared to 16.6 g/dL five months prior. White blood cell count, renal function, electrolytes, and urinalysis were normal.
The patient received fluids and one unit of packed red blood cells. Upper endoscopy and colonoscopy were unremarkable. Capsule endoscopy identified an ulcerated subepithelial lesion in the proximal jejunum occupying nearly the entire lumen (Figure 1). A CT scan revealed a 4.6 cm mesenchymal lesion in the jejunum, suggestive of a gastrointestinal stromal tumor (GIST) or leiomyoma (Figure 2).
Ulcerated subepithelial lesion in the proximal jejunum.
Rounded 4.6-cm jejunal nodule with well-defined limits compatible with a mesenchymal lesion (likely gastrointestinal stromal tumor (GIST) or leiomyoma).
Over five days, the patient required five units of packed red blood cells for ongoing rectal bleeding and symptomatic anemia. Due to the severity of the bleeding (hemoglobin varied from 6.8 g/dL to 7.4 g/dL.), a laparoscopic enterectomy with extracorporeal anastomosis was performed. Intraoperatively, a hypervascular, round tumor measuring approximately 5x4 cm was found 70 cm distal to the ligament of Treitz (Figure 3). The tumor had caused a jejuno-jejunal intussusception distal to its site.
Laparoscopic view of jejunum (approximately 70 cm distal to the Treitz angle) showing a prominent, hypervascularized, round tumor measuring approximately 5x4 cm.
Given the urgency and uncertain histopathology at the time, an extensive dissection of the adjacent meso was performed as a precautionary oncologic measure. The patient recovered uneventfully and remains asymptomatic at follow-up.
Histopathology confirmed a jejunal leiomyoma - a nodular lesion involving the muscularis mucosae, submucosa, and muscularis propria - composed of spindle cells without mitotic figures, necrosis, or hemorrhage (Figure 4). Immunohistochemistry was negative for c-KIT, DOG1, S100, and CD34, but positive for smooth muscle actin and desmin (Figure 5 and Table 1).
Enterectomy of the jejunum consistent with leiomyoma - nodular lesion with intramural growth and bulging of the intestinal mucosa.
Immunohistochemistry - anti-smooth muscle actin and anti-desmin markers.
Discussion
This case of jejunal leiomyoma presenting with acute gastrointestinal bleeding highlights several important aspects of small bowel tumors. The jejuno-jejunal intussusception observed in 2021, initially treated conservatively, was likely an early manifestation of the leiomyoma. In adult patients, intussusception often suggests an underlying pathology, unlike the more commonly idiopathic cases in children [4, 5].
Here, the intussusception was likely caused by the tumor serving as a lead point. This underscores the importance of a thorough diagnostic workup in adult intussusception cases. Earlier, more comprehensive imaging or endoscopic studies might have identified the tumor sooner (only CT scan was perfomerd during the intussuscepction episode).
Jejunal leiomyomas often present with nonspecific or no symptoms, making early diagnosis challenging. They are typically discovered after conservative treatments for conditions like duodenal ulcers or diverticulosis fail [3]. The acute gastrointestinal bleeding in this case deviates from the usual presentations, which more commonly involve mild bowel obstruction or pain [2].
The tumor’s hypervascularity and its role in intussusception are significant surgical findings. Only a few cases of jejuno-jejunal intussusception caused by leiomyomas have been reported in the English-language literature - seven in total, with five jejuno-jejunal and two being duodenojejunal [6-12]. This case thus contributes valuable insights into the diverse presentations and surgical implications of jejunal leiomyomas.
Conclusions
This case underscores the diagnostic challenges posed by rare small bowel tumors like jejunal leiomyomas. It highlights the importance of including such tumors in the differential diagnosis of adult intussusception and unexplained gastrointestinal bleeding. Early and comprehensive diagnostic evaluations are critical in such atypical presentations to ensure timely and appropriate management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gastrointestinal stromal tumors, intramural leiomyomas, and leiomyosarcomas in the duodenum: a clinicopathologic, immunohistochemical, and molecular genetic study of 167 cases Am J Surg Pathol Miettinen M Kopczynski J Makhlouf HR 6256412720031271724710.1097/00000478-200305000-00006 · doi ↗ · pubmed ↗
- 2Bleeding jejunal leiomyoma: a new approach Am J Gastroenterol Beajow M Singh HK Wiese DA Pandyan JR 131133901995 https://pubmed.ncbi.nlm.nih.gov/7801914/7801914 · pubmed ↗
- 3Acute GI bleed due to leiomyoma of the jejunum: a case report J Surg Case Rep Smith LE 020172017 https://doi.org/10.1093/jscr/rjx 13810.1093/jscr/rjx 138PMC 553401728775836 · doi ↗ · pubmed ↗
- 4Adult intussusception: a retrospective review World J Surg Honjo H Mike M Kusanagi H Kano N 1341383920152519284610.1007/s 00268-014-2759-9PMC 4273082 · doi ↗ · pubmed ↗
- 5Failed intussusception reduction in children: correlation between radiologic, surgical, and pathologic findings AJR Am J Roentgenol Ntoulia A Tharakan SJ Reid JR Mahboubi S 42443320720162722463710.2214/AJR.15.15659 · doi ↗ · pubmed ↗
- 6Adult intussusception due to enteric neoplasms Dig Dis Sci Yamada H Morita T Fujita M Miyasaka Y Senmaru N Oshikiri T 7647665220071726883610.1007/s 10620-006-9161-x · doi ↗ · pubmed ↗
- 7A rare cause of adult ileocolic intussusception: ileal leiomyoma BJR Case Rep Zhou KZ Mautone M Naidoo P 20170094420183093113110.1259/bjrcr.20170094 PMC 6438405 · doi ↗ · pubmed ↗
- 8An intraluminal leiomyoma of the small intestine causing invagination and obstruction: a case report Mt Sinai J Med Sunamak O Karabicak I Aydemir I Aydogan F Guler E Cetinkaya S Korman MU 10791081732006 https://pubmed.ncbi.nlm.nih.gov/17285198/17285198 · pubmed ↗