Dermatology (Beau’s Lines) and Forensic Pathology (Harris Lines and Linear Enamel Hypoplasia) Signs of Growth Arrest: A Case Report and Literature Review
Philip R Cohen

TL;DR
This paper discusses how trauma and systemic issues can cause growth arrest in nails, bones, and teeth, using a case study and literature review.
Contribution
The paper connects dermatological, forensic, and dental signs of growth arrest through a case report and literature review.
Findings
Beau’s lines in nails can appear 10 weeks after trauma.
Growth arrest signs like Harris lines and linear enamel hypoplasia are linked to systemic issues.
Diagnostic signs of growth arrest can be identified through skin, radiologic, and oral exams.
Abstract
Dermatology encompasses the evaluation and management of localized conditions that affect the nail plate, including trauma, primary dermatoses involving the nail bed and nail matrix, and systemic disorders with manifestations that impact the nail unit. In addition to traumatic events that can alter the nail unit, localized conditions such as periungual dermatitis and infections, as well as generalized diseases, can affect the nail matrix, resulting in temporary growth arrest of the nail plate. This can present as a groove (Beau’s line) in the nail plate that progressively grows out as the nail continues to grow. Forensic pathology includes forensic anthropology. Disease and starvation are the most common etiologies associated with growth arrest of the long bones near the epiphyseal plate; the radiolucent horizontal bands (Harris lines) are only observable on the roentgenogram. Localized…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
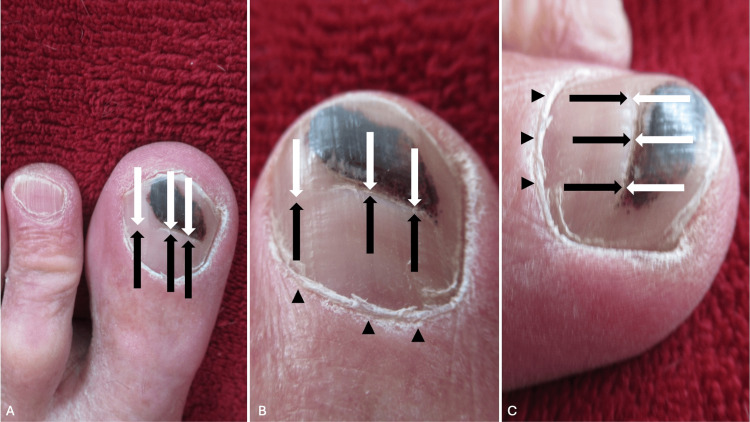 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3| Feature | Beau’s lines | Harris lines | Linear enamel hypoplasia |
| Location | One or more fingernails and/or toenails | Epiphyseal end of long bones | Permanent teeth |
| Etiology | Multiple nails: chemotherapy administration, diabetes mellitus, drug ingestion and medication allergies (antibiotics, antiepileptic agents, and retinoids), dysmenorrhea, febrile episodes with high fevers, infections (erythema nodosum leprosum, hand-foot-mouth disease, and syphilis), Kawasaki’s disease, intrauterine stress, myocardial infarction, nutritional deficiencies, renal failure, surgery, and surgical anesthesia Single nails: periungual dermatitis, psoriasis, and trauma | Disease and diet. Anthropological (deprivation of living conditions, famine, illness and plague), endocrinologic (Cushing syndrome, diabetes, and psychosocial short stature), medication (bisphosphonates, chemotherapy, and immunotherapy), metabolic (ethanol, heavy metal intoxication, and vitamin abnormalities), posttraumatic (nonaccidental trauma and Salter-Harris fracture), physiologic (saltation and stasis), and systemic (chronic anemia, infection, and hematologic neoplasm) | Childhood illnesses, injuries, and malnutrition. In addition, children with exposure to cigarette smoking and low socioeconomic status were at increased risk of developing enamel hypoplasia. The nutritional deficiencies include minerals, proteins, and vitamins. Also, infections (measles, otitis, respiratory, rubella, syphilis, tetanus, urinary tract, and varicella) and metabolic disorders (asthma, diabetes, and diseases of the following glands: adrenal, parathyroid, pituitary, and thyroid) |
| Age estimation when the injury occurred | Appears one to three months after a finger injury or two to six months after a toe injury | Several methods have been used to estimate the age, with significant intra-observer and interobserver variability | The methods are imprecise and do not conform to the current concepts of the enamel formation process |
| Symptoms | None | None | Carious teeth and their sequelae, inability to chew food, repeated or failing restorations, and sensitivity to air, cold, warm, and mechanical stimuli |
| Morphologic presentation | Transverse groove across nail plate forms lateral nail fold on one side to opposite side of digit; may be associated with proximal shedding of the nail plate | Linear radiolucent line (of increased bone density) at the distal epiphyseal area of a long bone visualized on the roentgenogram of the affected long bone of the arm and/or leg; the lines temporally correspond to the period when the etiology is active | Single or multiple pits, grooves, and/or white bands around the circumference of the tooth’s crown that are approximately parallel to the cementoenamel junction and perpendicular to the tooth’s long axis; the lines correspond to periods of active etiology |
| Treatment | Remove the causative etiology and stress-related event. Allow trauma to heal; thereafter, a normal nail plate will continue to grow distally from the nail matrix beneath the proximal nail fold | Resolve causative etiology; restore adequate nutrition in a person with malnutrition | Early diagnosis and risk recognition, adequate nutrition and good oral hygiene, attrition prevention, anticipation of caries and post eruption breakdown, desensitization, maintenance of dental care, mineralization of teeth, pit and fissure sealants, restorations, and appropriate extractions |
| Sequalae | Once the causative etiology resolves, a normal nail plate grows proximal to Beau’s line, and Beau’s line is no longer present once the nail plate has completely regrown | Some of the lines (which have been formed) may be removed by subsequent bone remodeling | Malocclusion, poor esthetics, predisposition to dental caries, and tooth sensitivity |
| Pathogenesis | Growth arrest of the nail plate because of the temporary cessation of nail matrix activity | Growth arrest of long bones near the epiphyseal plate | Growth arrest of tooth enamel formation |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrological Disorders and Treatments · Forensic Anthropology and Bioarchaeology Studies · Bone and Dental Protein Studies
Introduction
Dermatology is the study of skin, hair, and nails. Changes observed may reflect localized conditions or systemic disorders. A horizontal line across the nail plate (Beau’s line) is an indication of a temporary growth arrest of the nail plate [1-7].
Forensic pathology encompasses several subspecialties, including ballistics, entomology, odontology, osteology, and anthropology. Forensic anthropology involves the evaluation of skeletal remains of decedents to provide a biological profile, which may include information regarding the age, sex, stature, and ancestry of the individual. Distinctive features indicative of periods of growth arrest may be observed on the long bones (Harris lines) and teeth (linear enamel hypoplasia) [8-17].
A 65-year-old man who experienced a traumatic injury to the proximal nail fold of his left great toenail is described. The injury was painful, and within two weeks, he developed a subungual hematoma that presented as black discoloration of the proximal nail fold and the proximal nail. A Beau’s line appeared, within three months, as a transverse groove at the proximal nail fold and progressively moved distally as the nail plate grew. The dermatology-related features of temporary growth arrest affecting the nail plate (Beau’s line) of the reported patient are presented, and the forensic pathology-associated features affecting the epiphyseal region of the long bones (Harris lines) and the teeth (linear enamel hypoplasia) are summarized.
Case presentation
A 65-year-old man traumatically injured his distal left great toe when he accidentally dropped a heavy plastic container from a 3-foot height onto the proximal nail fold of his toe. The acute pain was severe, and the distal digit remained tender for nearly a day. The left proximal toenail fold developed a black discoloration (pseudo-Hutchinson sign), and the proximal nail appeared black within two weeks following the incident. During the subsequent weeks, the black discoloration of the subungual hematoma continued to expand to a maximum length of nine millimeters and a width of 15 mm. The normal-appearing nail plate of 3-4 mm was noted proximal to the subungual hematoma 18 weeks after the injury had occurred, which confirmed the diagnosis of pseudo-Hutchinson sign; the details and images of this patient’s subungual hematoma and transient proximal nailfold discoloration have previously been published [18].
A horizontal groove (Beau’s line) appeared distal to the proximal nailfold approximately 10 weeks after the injury occurred. As the nail continued to grow, the nail plate proximal to the linear groove was thickened. Examination 9½ months after the accident occurred showed that the transverse groove on the left great toenail plate was 9 mm distal to the left great toe proximal nailfold (Figure 1). The Beau’s line continues to move toward the free end of the nail plate on follow-up evaluations.
Beau’s line on the left great toenail of a 65-year-old manDistant top view (A), closer top view (B), and closer lateral view (C) of the left great toe. Beau’s line appears as the horizontal groove (between the black and the white arrows) and extends transversely across the nail plate from the lateral nailfolds on each side of the toe. The trauma to the proximal nail fold, when a plastic container dropped onto the proximal nailfold (black triangles), was the etiology of Beau’s line; the appearance of the subungual hematoma (black discoloration of the distal nail plate) occurred prior to the presentation of Beau’s line.
Discussion
The nail plate can be an indication of systemic disease or localized conditions. Koilonychia (spoon-shaped nails) can be an indication of iron-deficiency anemia, and Hutchinson sign (black pigmentation of the proximal nail fold) associated with longitudinal melanonychia striatum (a black band extending from the proximal nail fold toward the free edge of the nail plate) can be the clinical stigmata of a subungual malignant melanoma. Beau’s line (a transverse depression of the nail plate extending from the lateral nail fold on one side of the nail to the opposite side) can affect either a single nail as the result of injury to the nail matrix and temporary cessation of nail plate growth or multiple nails when it occurs as the result of a generalized condition (e.g., severe systemic disease) occurring in the individual and causing simultaneous growth arrest of more than one nail [1-5].
The evolution of transverse grooves in the nail plate was commented upon in an article that was published in 1846. The author was a French cardiologist from Paris, Joseph Honoré Siméon Beau (1806-1865). Beau described the appearance of the horizontal nail plate grooves in patients who had typhoid fever; indeed, he postulated that the duration of the disease was proportional to the width of the furrow or depression [3,6].
Beau’s lines occurring on multiple nails have been observed, which is associated with several conditions, including chemotherapy administration, diabetes mellitus, drug ingestion (e.g., antibiotics, antiepileptic agents, and retinoids) and medication allergies, dysmenorrhea, febrile episodes with high fevers, infections (e.g., erythema nodosum leprosum, hand-foot-mouth disease, and syphilis), Kawasaki’s disease, intrauterine stress, myocardial infarction, nutritional deficiencies, renal failure, surgery, and surgical anesthesia. One or more individual nails may be affected by Beau’s line in an individual who has an adverse event occurring on the distal aspect of a specific digit, such as periungual dermatitis, psoriasis, or trauma (Table 1) [1-17]. The patient described experiencing a traumatic event that only involved his left great toenail.
Fingernails and toenails grow at different rates. Nail growth on the fingers is typically three times faster than on the toes. Therefore, fingernails grow approximately three millimeters per month, and toenails grow one millimeter per month. In general, Beau’s lines are recognized four to eight weeks after the associated incident on the fingernails and three to even six months after the causative etiology on the toenails [3,6]. Beau’s line on the patient’s left great toenail was initially noticed about 10 weeks after the associated traumatic incident.
Beau’s lines can be associated with transverse leukonychia; this is a horizontal white band that is also present in the nail plate groove [6]. If the etiology was traumatic and associated with bleeding beneath the nail plate, an associated subungual hematoma may precede the appearance of Beau’s line, as in the man described in this report [6]. If the duration of the adverse event is prolonged, complete discontinuation of nail plate growth can result in proximal shedding of the nail plate (onychomadesis) [3,6,7].
Beau’s lines result from nail matrix growth arrest. However, the mechanism of pathogenesis that results in the retardation of normal nail growth when it occurs in the setting of drug exposure, fever, infection, and systemic disease remains to be determined. Four, not necessarily mutually exclusive, etiologies have been speculated [3].
The first etiology is that cellular proliferation may be inhibited; this would be a plausible explanation for Beau’s lines that occur when patients are receiving chemotherapeutic drugs with antimitotic activity. A second possibility is that the quality of the nail plate is altered (such that the nail becomes thinner and dystrophic); however, during this alteration, the activity of the nail matrix and growth rate of the nail plate remain intact. A third alternative is that nail injury or dysfunction causes nail growth retardation; this could occur in the setting of median nerve damage, reflex sympathetic dystrophy in children, and trauma to the hand. Finally, as in the reported patient, direct damage to the nail matrix resulting from trauma or inflammation that affects the periungual and/or matrix regions of the distal digit can lead to a horizontal groove or proximal shedding of the nail [3].
Harris lines are transverse sclerotic radiopaque lines within the metaphases and proximal diaphysis of long bones. They are most often noticed in the distal femur and the proximal tibia; however, they can also occur in the distal portions of the long bones of the upper extremity (Figure 2). They represent a temporary arrest of the longitudinal growth of the long bone [8-12].
Harris lines on the distal radius and ulnaRadiopaque Harris growth arrest lines are present on the right distal radius and ulna (demonstrated by orange arrows with black outlines) in a 13-year-old boy with an underlying bone disease.The photograph was provided on April 13, 2017, by James Heilman, MD. Permission for free republishing is granted; the file is licensed under the Creative Commons Attribution-Share Alike 4.0 International license.
Herbert Albert Harris (1886-1968) was a professor of anatomy at the University of Cambridge. In 1926, he reported his research on diabetic children, including the causative factors and the formation of transverse lines in their long bones. In 1927, Edwards A. Parks (1877-1969), a pediatrician, co-authored a paper describing similar observations. Similar lines were observed earlier by Wegner (1874) in the setting of rickets, by Ludloff (1903) from physiologic development around the knees, and by Stettner in healthy and sick children (1920 and 1921). Although the long bone growth arrest lines are occasionally referred to as Park-Harris lines, they are most commonly designated as Harris lines [8-12].
Harris lines have historically been attributed to juvenile malnutrition (starvation), diseases, and psychogenic stress. However, Harris lines can be associated with endocrinopathies, medications, metabolic derangements, systemic illnesses, and trauma (Table 1) [1-17]. The lines are transverse bands of increased radiodensity (which histologically consist of zones of increased thickness of trabecular bone) that can be observed on plain radiographs, computerized axial tomography scans, magnetic resonance images, or positron-emitting tomography bone scans (by increased uptake of 18-fluorodeoxyglucose) [8-12].
Investigators claim to be able to determine the age of the patient or the decedent when the etiologic event caused the Harris lines. However, the evaluation of Harris lines is characterized not only by significant intra-observer variability and high inter-observer biases but also by at least three different methods to determine age. The lines can be noted as early as six weeks following an injury. However, as the individual ages, dynamic bone remodeling occurs, and the previously formed Harris lines may disappear [8-12].
Several mechanisms of the pathogenesis of Harris lines have been postulated. Longitudinal growth arrest of the long bone is a required component in the formation of the transverse line; however, some investigators propose that the appearance of the lines is caused by the recovery of the bone and its regrowth. Associated etiologies that may influence the pathogenesis of the retardation of bone growth include childhood illnesses, hematologic neoplasms, malnutrition syndromes, medications (such as bisphosphonate, immunotherapy, isotretinoin, methotrexate, and other systemic chemotherapy), metabolic disorders (such as endocrinopathies), prolonged immobility, and trauma [8-12].
Linear enamel hypoplasia is an environmentally associated hypoplasia of the permanent teeth [13-17]. It typically affects multiple teeth; one or more symmetric white bands develop around the circumference of the tooth’s crown (Figure 3). The bands are perpendicular to the tooth’s long axis and approximately parallel to the cementoenamel junction. Each band corresponds to an episode of the causative etiology (Table 1) [1-17].
Linear enamel hypoplasiaThe teeth show white-appearing horizontal lines of linear enamel hypoplasia (demonstrated by the white arrows) on their surfaces. The enamel hypoplasia lines demonstrate the defects of enamel that form during crown development because of either nutritional stress or disease during infancy and childhood.The photograph was provided by Brian Spatola on October 22, 2007, from the Otis Historical Archives National Museum of Health & Medicine. Permission for free republishing is granted; the file is licensed under the Creative Commons Attribution 2.0 Generic license.
In contrast to Beau’s lines and Harris lines, linear enamel hypoplasia may be symptomatic. Affected individuals may experience sensitivity to air, cold, warmth, and mechanical stimuli. In addition, some individuals with linear enamel hypoplasia experience carious teeth, difficulty chewing food, and repeated or failing restorations [13-17].
Linear enamel hypoplasia occurs when there is a temporary interruption of the matrix secretion by the ameloblasts. Ameloblasts are the enamel-forming cells; they begin secreting enamel shortly after the dentin-forming cells (odontoblasts) lay down a dentin matrix platform. The enamel is laid down in a series of layers, beginning with the cuspal enamel and subsequently the lateral enamel of the tooth’s crown. Stressful events to the individual are observed as defects in the enamel of the crown (such as pits, grooves, or lines of enamel loss) when they occur during the lateral enamel formation [13-17].
Environmental stresses associated with linear enamel hypoplasia predominantly include childhood illnesses, injuries, and malnutrition. Children from low socioeconomic status and who have been exposed to cigarette smoking are at increased risk of developing enamel hypoplasia. Several other factors that have been associated with linear enamel hypoplasia include infections (such as measles, otitis, respiratory infections, rubella, syphilis, tetanus, urinary tract infections, and varicella), metabolic disorders (such as asthma, diabetes, and diseases of the following glands: adrenal, parathyroid, pituitary, and thyroid), mineral deficiencies (such as calcium, fluorine, magnesium, and phosphorus), protein deficiencies (such as amelogenin, enamelin, and tuftelin), and vitamin deficiencies (such as vitamins A, C, D, and K) [13-17].
The treatment of linear enamel hypoplasia is the prevention of future episodes and monitoring for adverse sequelae. Good oral hygiene and providing adequate nutrition are of paramount importance. In addition to early diagnosis and risk recognition, management of linear enamel hypoplasia includes maintenance of dental care (including anticipation of caries and post-eruption breakdown), desensitization, prevention of attrition (by using acrylic jigs and custom-made bite blocks), mineralization (with fluoride and calcium phosphate agents), sealants for pits and fissures, restorations (including glass ionomer cement, composite, stainless steel crowns, full veneer metal-ceramic crowns, fixed-removable partial dentures, and implants), and extractions (if the teeth are non-restorable). Malocclusion, poor esthetics, predisposition to dental caries, and tooth sensitivity are potential adverse outcomes for individuals who develop linear enamel hypoplasia [13-17].
Conclusions
Growth arrest of nail plates can present as Beau’s lines, of long bones can appear as Harris lines, and of enamel formation of teeth can result in the development of linear enamel hypoplasia. Identification of the stigmata of growth arrest in a patient or a decedent can provide insight into the occurrence of a prior adverse event, such as systemic illness, malnutrition, trauma, or the effects of medications. The case report of a dermatology-related presentation of growth arrest in a 65-year-old man with a subungual hematoma associated with trauma to the proximal nail fold of his left great toe was described, and a narrative review of forensic pathology-associated manifestations of growth arrest was presented. In conclusion, morphologic clues to localized trauma or generalized disease in an individual can be observed by the astute clinician during the evaluation of the nails, long bones, or teeth.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Beau's lines QJM Lin X Wu S 66967011020172901693010.1093/qjmed/hcx 122 · doi ↗ · pubmed ↗
- 2Beaus lines Indian Pediatr Khemani C Khubchandani R 47442007 https://pubmed.ncbi.nlm.nih.gov/1727743417277434 · pubmed ↗
- 3Nail matrix arrest following hand-foot-mouth disease: a report of five children Pediatr Dermatol Clementz GC Mancini AJ 7111720001072098010.1046/j.1525-1470.2000.01702.x · doi ↗ · pubmed ↗
- 4Chemotherapy-induced transverse ridging of the nails Cutis Requena L 129130481991 https://pubmed.ncbi.nlm.nih.gov/19352371935237 · pubmed ↗
- 5Mees lines and Beau lines after chemotherapy CMAJ Huang TC Chao TY 149182201010.1503/cmaj.090501 PMC 282648220008502 · doi ↗ · pubmed ↗
- 6What do Beau's lines mean?Int J Dermatol De Berker D 545546331994796034610.1111/j.1365-4362.1994.tb 02890.x · doi ↗ · pubmed ↗
- 7Onychomadesis: literature review Br J Dermatol Hardin J Haber RM 59259617220152513219810.1111/bjd.13339 · doi ↗ · pubmed ↗
- 8Harris lines revisited: prevalence, comorbidities, and possible etiologies Am J Hum Biol Papageorgopoulou C Suter SK Rühli FJ Siegmund F 3813912320112138745910.1002/ajhb.21155 · doi ↗ · pubmed ↗