Outpatient treatment of varicose veins with endolaser in clinic vs. hospital: cost-benefit and safety assessment
Camila Biedler Giordani, Mateus Picada Correa, Luiza Brum Borges, Vitória Cerbaro Farias, Renan Camargo Puton, Jaber Nashat Saleh, Rafael Stevan Noel, Julio Cesar Bajerski, Camila Biedler Giordani, Mateus Picada Correa, Luiza Brum Borges, Vitória Cerbaro Farias

TL;DR
This study compares the safety and cost of outpatient versus hospital-based laser treatment for varicose veins, finding outpatient treatment is safe and cost-effective despite higher clinic fees.
Contribution
Demonstrates the safety and cost-benefit of outpatient endolaser treatment for varicose veins in Brazil.
Findings
Outpatient treatment had a statistically higher cost (R$1593.40) compared to hospital treatment (R$1391.99).
No intraoperative or postoperative complications were observed in either group.
Outpatient treatment is safe and offers positive cost-benefit for patients despite higher costs.
Abstract
Varicose disease is a common pathology among the population, with an incidence of about 38%. In Brazil, it affects 45% of women and 30% of men. Currently, endovenous thermal ablation (EVTA) of the saphenous vein is the method of choice in the treatment of varicose veins. As a minimally invasive procedure that promotes quick recovery and does not require hospitalization, it can be performed on an outpatient basis. To evaluate the safety and cost-benefit of outpatient varicose vein treatment in a clinic compared to the same procedure performed in a hospital environment. A uncontrolled retrospective transversal study of case series evaluated a random group of 50 patients undergoing EVTA for the treatment of varicose disease by the same group of vascular surgeons. Twenty-five underwent the procedure in a tertiary hospital environment and 25 on an outpatient basis. The average costs of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1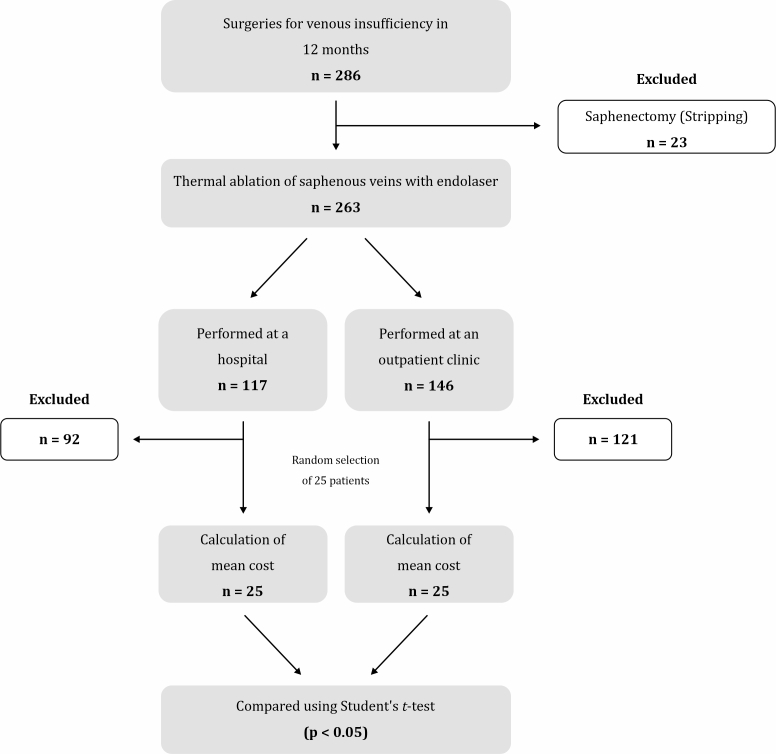 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiagnosis and Treatment of Venous Diseases · Venous Thromboembolism Diagnosis and Management · Central Venous Catheters and Hemodialysis
INTRODUCTION
Varicose veins are superficial veins, generally located in the lower limbs, that become twisted and dilated > 3 mm.^1-3^ This condition is quite common, with a worldwide prevalence ranging from 29.5 to 39.0% in women and from 10.4 and 23.0% in men.^2,3^ In Brazil, estimates are similar. According to the Sociedade Brasileira de Angiologia e de Cirurgia Vascular (Brazilian Society of Angiology and Vascular Surgery), 38% of Brazilians have varicose veins (45% of women and 30% of men) and, in people aged over 70 years, the prevalence can reach 70%.^4^
Endovenous thermal ablation (ETA) of saphenous veins is progressively replacing conventional surgery as a treatment for saphenous reflux, being strongly recommended in the guidelines.^5^ This procedure is performed percutaneously under tumescent local anesthesia guided by ultrasound.^6^ This allows for a more precise procedure and faster recovery, reducing postoperative hospitalization time and allowing the procedure to be performed on an outpatient basis.^6^
ETA has better results and a lower complication rate than traditional surgery,^3,6^ mainly due to the quick recovery, less pain, and an early return to daily activities.^7^ Although the cost-benefit of outpatient ETA is positive in Europe, it is still unclear in Brazil.^8-10^ Therefore, this study was a safety and cost-benefit assessment of varicose vein treatment in outpatient and hospital settings in Brazil.
METHODOLOGY
This cross-sectional, retrospective, uncontrolled case series study included 50 patients who were randomly selected based on their medical records by a person who did not otherwise participate in the study. All patients had undergone ETA of saphenous veins and phlebectomy of tributaries by a team with 15 years’ experience in treating venous insufficiency.
The inclusion criterion was endolaser surgery, and the exclusion criterion was saphenectomy (stripping). In total, 25 procedures were performed at a tertiary hospital and 25 were performed at an outpatient clinic equipped to perform procedures with local anesthesia and conscious sedation, meeting all regional and national health standards (Figure 1). The study design is outlined in Figure 2.
Private outpatient clinic in which the surgeries were performed.
Study design diagram.
Although the ideal sample was calculated at n = 32 in each group, due to restrictions imposed by the Lei Geral de Proteção de Dados (General Data Protection Law), the operating costs of only 25 patients per group could be obtained. Patients were selected through the hospital’s electronic medical records based on the medical record number, which hid their identity. System filters were used to identify patients who underwent the procedures in the clinic or the hospital, and 25 individuals were randomly selected from each group.
To assess the procedures’ safety in hospital and clinical settings, patient records were retrospectively investigated for intra- or postoperative complications. The cost of the inpatient procedure for each patient was provided by a health insurance company, excluding physician fees, i.e., only the hospital cost was provided. The cost of the outpatient procedure, charged directly to the patient, was provided by the private clinic, also excluding physician fees. Neither estimate included the cost of the fiber used in the procedure, since it was identical for both groups. The cost included room rental, anesthesia, and materials (micropore tape, bandages, sutures, etc.). After collecting the data, the mean cost was determined for each treatment setting, and the results were compared statistically using Student's t-test. P-values < 0.05 were considered statistically significant. The CHEERS guidelines were followed throughout the development of this study.^11^
The study protocol was approved by the Universidade de Passo Fundo Ethics Committee (certificate 52368120.7.0000.5342; opinion 5,065,505). All patients provided written informed consent.
RESULTS
Between January 2023 and February 2024, the medical team performed 286 procedures to treat varicose veins, 263 of which were laser thermoablation of saphenous veins. Of these, 117 were performed at the hospital and 146 at the private clinic, and 25 from each group were randomly selected. The mean total cost of the procedure (room fee and material cost, without physician fees), was BRL 1,391.99 (SD, 280.8) at the hospital and BRL 1,593.40 (SD, 99.53) at the clinic, which was a significant difference according to Student's t-test (p = 0.02).
Of the 25 patients who underwent in-hospital treatment, 18 were women and seven were men. Of the 25 outpatients, 20 were women and five were men. In both groups, 15 patients underwent bilateral procedures and underwent 10 unilateral procedures. No intra- or postoperative complications occurred.
DISCUSSION
The ETA method uses heat to occlude the veins. In other words, it induces collagen shrinkage followed by fibrotic sealing of the vessel lumen.^12^ Thermal ablation of the great saphenous vein is the focus of the technique, which can be performed in an outpatient setting under local anesthesia. Residual varicosities can be treated either by sclerotherapy or by multiple phlebectomies at the beginning of treatment.^7^ Due to these factors, the number of ETA procedures in outpatient settings is gradually increasing, and the procedure has been shown to be safe and effective for varicose vein treatment,^6^ with success rates of up to 92%.^13^ The 2023 Brazilian Society of Angiology and Vascular Surgery guidelines on chronic venous disease recommend thermal ablation without ligating the saphenofemoral junction to treat great and small saphenous vein insufficiency, with a strong level of evidence (A) and a Class I recommendation.^13^
Outpatient surgery using minimally invasive procedures is becoming the method of choice among a significant portion of the medical community. In addition, many patients and family members prefer outpatient surgery due to the infrastructure and familiarity with the health care team, producing a relationship of greater trust and ease between the parties.^8^ The possibility of personalizing patient care in a private clinic is another advantage to consider. This is in line with the philosophy of outpatient surgery, in which trusted hands manage treatment and promote patient-centered, integrated, and interdisciplinary medicine.^8^
In addition to patient benefits, outpatient procedures also benefit the healthcare system.^8^ The decentralization of care alleviates overload in hospitals by reducing the number of less complex cases, allowing them to focus on surgeries and procedures that require a hospital environment.
A 2018 prospective cohort study by Varetto et al. compared ETA performed in hospital and outpatient settings, finding no significant differences in clinical success or perioperative complications. However, patients over 65 years of age preferred the outpatient setting, probably because it involved less emotional stress.^6^ Another important advantage of outpatient surgery is the reduced risk of surgical site infections. Nosocomial infections occur in 25% of hospital-based procedures^14,15^ but in only 3% of outpatient procedures.^10^
Careful selection of outpatient candidates is necessary.^8^ In individuals with higher levels of anxiety and severe varicose vein disease, sedation and spinal anesthesia may facilitate the procedure. Because anesthesiologists are available in the hospital setting, deeper sedation can be performed, which relieves anxiety, and spinal anesthesia can be used in cases of multiple varicose veins, where tumescence alone would be insufficient to eliminate the patient's pain. In individuals with a higher risk of intraoperative complications, it may be more prudent to perform the procedure in a hospital setting.^8^
This study raised a number of important points. First, safety was equivalent in outpatient and inpatient surgery, since no complications were observed in either group.
Second, although the cost difference between the treatment settings was statistically significant, it was quantitatively small, possibly with little budgetary impact. It is important to note that fiber was excluded from the cost analysis. In some centers, when the material is added to the hospital cost, the cost difference may favor outpatient surgery. More thorough cost studies are needed to clarify this issue. This factor may explain the different results of European studies, in which the cost of outpatient procedures was lower than inpatient procedures.^6,8-10^
In addition to the cost of fiber, the cause of this discrepancy requires further investigation. Input costs are another hypothesis: when negotiated in large quantities through contracts, as is done by large hospital chains, lower prices are possible. In the present study, the hospital where the procedures were performed is philanthropic, resulting in lower operating costs that can be passed on to patients.
Guillaumon and Rocha^16^ conducted a cost analysis study of outpatient and inpatient saphenectomy procedures performed at a university hospital, finding that the outpatient procedure was a better value, unlike our findings. However, this study was published in 2003, with the data having been collected between 1992 and 1998, a period far removed from the current economy. Furthermore, it is worth noting that the present study analyzed saphenous vein treatment using endolaser, and not stripping, which may also explain the divergent results.
Although the ideal sample was calculated at 32 participants per group, legal restrictions prevented us from obtaining data directly from the hospital via the health insurance company, limiting the sample to 25 patients. This limitation should be considered when interpreting the results, since the reduced sample size could have affected the study power. Regarding study randomization, this is a simple and practical method in retrospective studies, in which the medical record number functions as a neutral identifier. The non-participation of the researchers in selection process strengthened its impartiality.^17^
More robust studies with larger sample sizes conducted at several vascular health centers throughout the country are needed to assess the increase in ETA in Brazil. Therefore, understanding how the procedure is organized throughout Brazil is of utmost importance for vascular surgeons who seek to provide the best treatment for their patients.
To the best of our knowledge, this is the first study to compare inpatient and outpatient ETA in Brazil, although it has some limitations. It was a single-center study from one region of the country and included few patients. Furthermore, as a retrospective study, the analysis was limited regarding the materials, as well as the surgery time and complexity.
CONCLUSIONS
Although the mean cost of the outpatient procedure was higher than the inpatient procedure, the advantages of outpatient surgery provide a favorable cost-benefit ratio for patients, and outpatient ETA is safe. However, further studies with larger samples conducted at different centers throughout Brazil are needed, in addition to analyses of why outpatient costs are higher than hospital costs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chung JH Heo S Varicose veins and the diagnosis of chronic venous disease in the lower extremities J Chest Surg.202457210911910.5090/jcs.23.11037994090 PMC 10927428 · doi ↗ · pubmed ↗
- 2Gawas M Bains A Janghu S Kamat P Chawla P A comprehensive review on varicose veins: preventive measures and different treatments J Am Nutr Assoc.202241549951010.1080/07315724.2021.190951034242131 · doi ↗ · pubmed ↗
- 3Raetz J Wilson M Collins K Varicose veins: diagnosis and treatment Am Fam Physician 2019991168268831150188 · pubmed ↗
- 4Sociedade Brasileira de Angiologia e de Cirurgia Vascular Estimativas Internet 2024 citado 2024 abr 25 https://sbacv.org.br/imprensa/estimativas/
- 5De Maeseneer MG Kakkos SK Aherne T et al European Society for Vascular Surgery (ESVS) 2022 clinical practice guidelines on the management of chronic venous disease of the lower limbs Eur J Vasc Endovasc Surg 202263218426710.1016/j.ejvs.2021.12.02435027279 · doi ↗ · pubmed ↗
- 6Varetto G Gibello L Frola E et al Day surgery versus outpatient setting for endovenous laser ablation treatment: a prospective cohort study Int J Surg 20185118018310.1016/j.ijsu.2018.01.03929412185 · doi ↗ · pubmed ↗
- 7Darwood RJ Theivacumar N Dellagrammaticas D Mavor AI Gough MJ Randomized clinical trial comparing endovenous laser ablation with surgery for the treatment of primary great saphenous varicose veins Br J Surg 200895329430110.1002/bjs.610118278775 · doi ↗ · pubmed ↗
- 8Deindl C Neumann A The future of outpatient surgery Urologie.202261882983810.1007/s 00120-022-01878-535925293 PMC 9257115 · doi ↗ · pubmed ↗