Genomic medicine for heart failure prediction in patients with atrial fibrillation
Leonoor F J M Wijdeveld, Sean J Jurgens

Abstract
Graphical Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
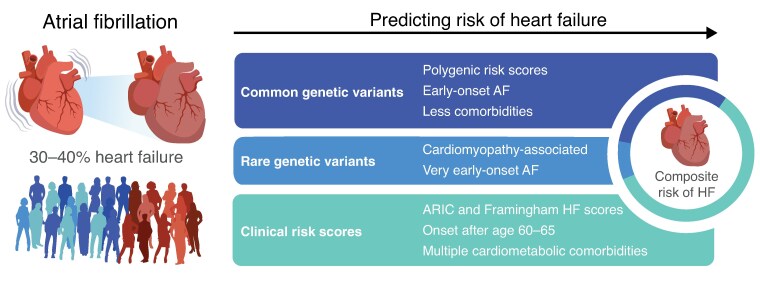 Figure 1
Figure 1- —Amsterdam UMC YTF
- —Dutch Heart Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBiotechnology and Related Fields
This editorial refers to ‘Polygenic risk-based prediction of heart failure in young patients with atrial fibrillation: an analysis from the UK Biobank’, by Hyo-Jeong Ahn et al., https://doi.org/10.1093/europace/euaf104.
Atrial fibrillation (AF) is a highly prevalent disorder of the cardiac rhythm. While there is a strong clinical emphasis on stroke risk and stroke prevention, AF also represents a major risk factor for heart failure (HF). In fact, 30–40% of AF patients will develop HF during their lifetime, while only 10–20% will experience an ischaemic stroke.^1^ In turn, HF is associated with substantially increased mortality among AF patients.^2^ Nevertheless, while international guidelines stress the importance of individualized clinical management,^3,4^ prevention and prediction of HF remain exceedingly challenging in AF patients.
AF is known to have a strong heritable component. Notably, large genetic association studies (GWAS) have identified hundreds of genetic variants associated with arrhythmia.^5,6^ At the same time, AF is common in heritable cardiomyopathies and may be an early indicator of such genetic cardiomyopathy,^7^ especially in a young AF patient with few comorbidities.^8^ These findings suggest that genetic factors contribute to the susceptibility of AF patients to develop HF, leaving an opportunity for genome-informed personalized medicine. Indeed, we recently showed that certain rare genetic variants increase the risk of HF in people with AF.^9^ Although these rare genetic variants are more common in AF patients than in the general population, they are still quite rare. In contrast, common genetic variants could be relevant to a larger segment of the AF population. While it is plausible that common genetic variants contribute to HF risk in AF patients, the role of such variants in HF risk stratification remains underexplored.
Hereto, Anh et al.^10^ studied the potential role of a polygenic risk score (PRS), built from common genetic variants, for the prediction of HF among AF patients. They developed the PRS from a prominent HF GWAS,^11^ and employed a statistical approach to ensure data from UK Biobank individuals did not contribute to the PRS development. Next, they applied this new PRS score to a cohort of 21 167 individuals with AF—without any prior HF diagnosis—from the UK Biobank, a well-known large prospective cohort from the United Kingdom. In this cohort, they examined if participants in the upper two tertiles of the PRS score, labelled moderate-high, had a relatively higher risk of incident HF compared with the lowest tertile, labelled low. Subsequently, they stratified the analysis by age of AF onset with a cut-off of 60 years for early-onset AF. Finally, they investigated if the PRS would improve their own clinical risk model for HF.
In their work, Anh et al. found that AF patients with a moderate-high PRS score had an approximately 20% higher risk of HF over a median follow-up of 3.8 years, as compared with patients with low polygenic risk. This increase in HF risk was even more pronounced when stratifying the cohort by age of diagnosis. In individuals with early-onset AF (N = 2231), a moderate-high PRS was associated with an over two-fold higher risk of future HF. Next, Anh et al. constructed a clinical risk model for HF which had a modest area under the curve (AUC) of 0.64. Once they added the PRS to their clinical risk model, correct prediction of HF showed a modest improvement in all AF patients (8.8%), but the predictive ability of the model increased remarkably in early-onset AF patients by 29.7%, AUC 0.71.
Among these early-onset AF patients, the authors then showed that PRS was most valuable for individuals without prevalent diabetes, hypertension, or a history of MI. This finding suggests an important role for PRS in prognosis, as these individuals would be classified as low-risk when assessed solely by conventional cardiometabolic risk factors. On the other hand, the PRS by Anh et al. did not contribute to the risk of HF in people with AF and a history of MI, indicating that the influence of this HF PRS is negligible when AF is associated with overt structural insult to the heart. As such, the extensive subgroup analyses form a significant strength of the paper, showing which patients would potentially benefit from PRS-based stratification. We do note, however, that subgroups were individually small and additional replication in other cohorts will be needed before definitive statements can be made about specific subgroups within the early-onset patients. Moreover, it should be noted that the study population was restricted to individuals of European ancestry, thus the utility of PRS for HF risk prediction in the AF still needs to be validated in diverse cohorts.
That being said, the results in the early-onset AF group are striking given the recent attention to genetics in young AF patients in recent AF guidelines. The new ACC/AHA guidelines provided an initial 2B recommendation to consider genetic testing in patients with very early-onset AF (<45 years).^12^ Similarly, the 2024 ESC/EACTS guidelines also emphasize personalized management of risk factors and comorbidities in AF.^4^ Consistent with the findings by Ahn et al., previous work on rare genetic variation also indicated that the influence of genetics is increasingly important with younger ages of AF onset.^9,13^ Thus, it is conceivable that an HF PRS might be a meaningful addition to genetic testing for individuals with very early-onset AF, and in particular for the estimated 85–95% of patients without causative rare genetic variants.^9,14^ While we note that clinical genetic testing currently focuses on rare genetic variants and does not assess PRS, these results indicate that both genetic approaches could add to the prognosis of early-onset AF patients, in the future. Nevertheless, we stress again that additional studies of young AF patients—assessing both common and rare genetic variation^9^—are needed.
The meaningful contribution of PRS to HF prediction—especially among young AF patients with few comorbidities—also provides a compelling rationale for future research integrating both genetic and dynamic molecular approaches, like proteomics and metabolomics, to elucidate the distinct pathways driving HF development in this patient population.^15^ This is especially important for therapeutic strategies in these young patients, as current interventions, like lifestyle modifications, cardiovascular risk management, and increased clinical surveillance, would likely not reach their full potential in patients with few comorbidities. In addition to improving mechanistic and therapeutic understanding of AF and HF, future studies could also assess whether circulating proteins or metabolites, potentially paired with imaging data, might further improve HF prediction models on top of clinical and genetic risk.^16^
Overall, a more holistic approach to HF prediction in the AF population is needed. The study by Anh et al. identifies a significant genetic component to HF risk in AF patients, which calls for increased efforts to unravel how rare and common variants leave the fibrillating heart more vulnerable to HF. More information on how rare and common genetic variants contribute to the development of HF could open the door to personalized screening tools and targeted therapies to prevent, detect, or delay the onset of HF in (early-onset) AF patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Vinter N, Cordsen P, Johnsen SP, Staerk L, Benjamin EJ, Frost L et al Temporal trends in lifetime risks of atrial fibrillation and its complications between 2000 and 2022: Danish, nationwide, population based cohort study. BMJ 2024;385:e 077209.38631726 10.1136/bmj-2023-077209 PMC 11019491 · doi ↗ · pubmed ↗
- 2Zuin M, Bertini M, Vitali F, Turakhia M, Boriani G. Heart failure-related death in subjects with atrial fibrillation in the United States, 1999 to 2020. J Am Heart Assoc 2024;13:e 033897.38686875 10.1161/JAHA.123.033897 PMC 11179935 · doi ↗ · pubmed ↗
- 3Joglar JA, Chung MK, Armbruster AL, Benjamin EJ, Chyou JY, Cronin EM et al 2023 ACC/AHA/ACCP/HRS Guideline for the diagnosis and management of atrial fibrillation: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2024;149:e 1–156.38033089 10.1161/CIR.0000000000001193 PMC 11095842 · doi ↗ · pubmed ↗
- 4Rienstra M, Tzeis S, Bunting KV, Caso V, Crijns HJGM, De Potter TJR et al Spotlight on the 2024 ESC/EACTS management of atrial fibrillation guidelines: 10 novel key aspects. Europace 2024;26:euae 298.39716733 10.1093/europace/euae 298PMC 11666470 · doi ↗ · pubmed ↗
- 5Roselli C, Surakka I, Olesen MS, Sveinbjornsson G, Marston NA, Choi SH et al Meta-analysis of genome-wide associations and polygenic risk prediction for atrial fibrillation in more than 180,000 cases. Nat Genet 2025;57:539–47.40050429 10.1038/s 41588-024-02072-3PMC 12094172 · doi ↗ · pubmed ↗
- 6Choi SH, Jurgens SJ, Xiao L, Hill MC, Haggerty CM, Sveinbjörnsson G et al Sequencing in over 50,000 cases identifies coding and structural variation underlying atrial fibrillation risk. Nat Genet 2025;57:548–62.40050430 10.1038/s 41588-025-02074-9 · doi ↗ · pubmed ↗
- 7Yeung C, Enriquez A, Suarez-Fuster L, Baranchuk A. Atrial fibrillation in patients with inherited cardiomyopathies. Europace 2019;21:22–32.29684120 10.1093/europace/euy 064 · doi ↗ · pubmed ↗
- 8Kany S, Jurgens SJ, Rämö JT, Christophersen IE, Rienstra M, Chung MK et al Genetic testing in early-onset atrial fibrillation. Eur Heart J 2024;45:3111–23.39028637 10.1093/eurheartj/ehae 298PMC 11379493 · doi ↗ · pubmed ↗