Identifying and reporting modifications to surgical innovation: a systematic review of IDEAL/IDEAL-D studies
James Olivier, Daisy Elliott, Kerry Avery, Natalie S Blencowe, Rhiannon Macefield

TL;DR
This paper reviews how surgical innovations are modified and reported, aiming to improve transparency and patient safety in surgical research.
Contribution
The study identifies gaps in reporting surgical modifications and proposes a checklist to improve consistency and safety.
Findings
73.1% of included studies reported modifications to procedures, devices, or patient selection.
Most modifications were reported in IDEAL stage 2a, with inconsistent reporting across other stages.
The findings will inform a checklist to standardize modification reporting in surgical innovation.
Abstract
The Idea, Development, Evaluation, Assessment and Long-term follow-up (IDEAL) framework was designed to improve the quality of surgical research and evaluation of surgical innovation. It has become a widely cited tool for evaluating innovative devices and procedures, yet challenges remain concerning the definition and reporting of incremental innovative modifications, hindering evolution and evaluation of innovations and potentially risking patient safety. This systematic review examined IDEAL studies to identify such modifications and establish recent practices around modification reporting to inform the development of future guidance to facilitate safe, transparent and efficient surgical innovation. Systematic review and thematic synthesis of studies reporting surgical innovation. Web of Science and Scopus were searched in July 2023 using citation tools to identify studies following…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
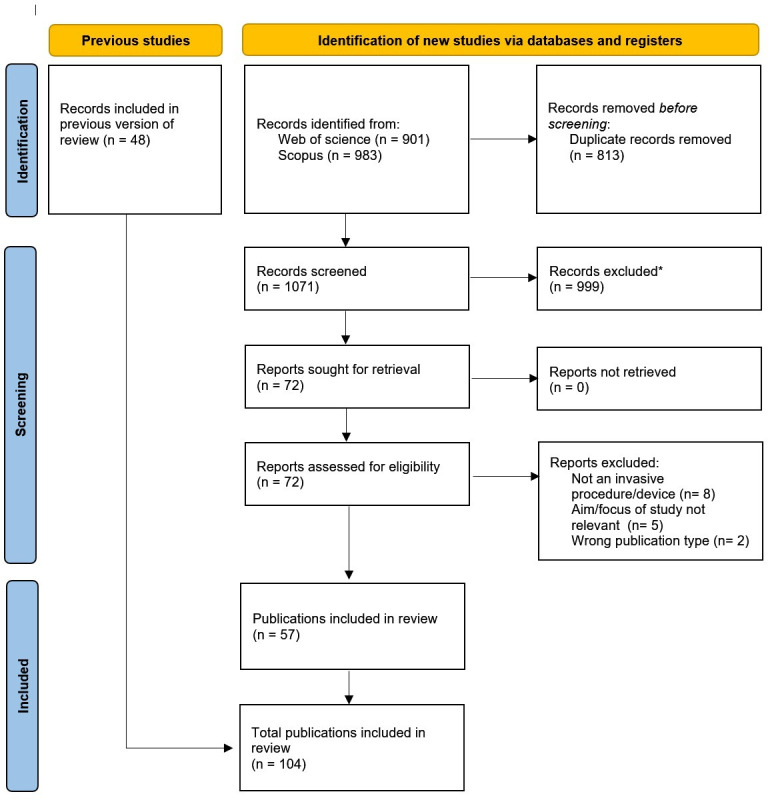 Figure 1
Figure 1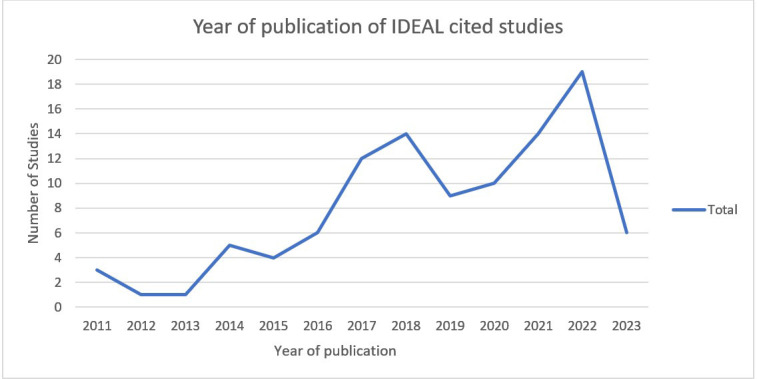 Figure 2
Figure 2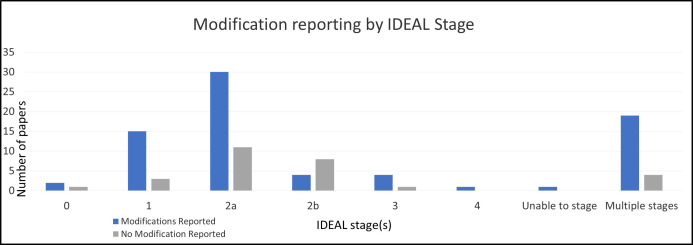 Figure 3
Figure 3| Total number of included studies (%) | Number of studies categorised by IDEAL stage | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| 0 (n=3) | 1(n=18) | 2a (n=41) | 2b (n=12) | 3(n=5) | 4 (n=1) | Multiple or unable to stage (n=24) | |||
| Study design | Case series | 62 (60) | – | 12 | 35 | 2 | 2 | 1 | 10 |
| Case study | 5 (5) | – | 5 | – | – | – | – | – | |
| Cohort study | 22 (21) | – | 1 | 5 | 9 | – | – | 7 | |
| Multiple study designs | 6 (6) | – | – | – | – | – | – | 6 | |
| Preclinical study | 3 (3) | 3 | – | – | – | – | – | – | |
| Randomised trial | 6 (6) | – | – | 1 | 1 | 3 | – | 1 | |
| Surgical specialty | Breast surgery | 5 (5) | – | – | 2 | – | – | – | 3 |
| Cardiothoracic Surgery | 1 (1) | – | – | 1 | – | – | – | – | |
| Colorectal surgery | 12 (12) | – | 1 | 6 | – | – | – | 5 | |
| Head and Neck | 5 (5) | – | 2 | 3 | – | – | – | – | |
| Hepatobiliary | 8 (8) | 1 | 2 | 4 | – | 1 | – | – | |
| Multiple | 2 (2) | – | – | 2 | – | – | – | – | |
| Neurosurgery | 2 (2) | – | 1 | – | – | – | – | 1 | |
| Obstetrics and gynaecology | 11 (11) | – | 4 | 1 | 4 | 1 | – | – | |
| Oesophagogastric | 7 (7) | – | – | 3 | 1 | – | – | 3 | |
| Orthopaedics | 5 (5) | 1 | – | 2 | – | – | – | 2 | |
| Paediatric Surgery | 1 (1) | – | 1 | – | – | – | – | – | |
| Transplant | 8 (8) | – | 2 | 1 | 1 | – | – | 4 | |
| Urology | 38 (36) | 1 | 5 | 17 | 6 | 3 | 1 | 5 | |
| Country | European Economic Area (Non-UK) | 52 (50) | 1 | 10 | 22 | 6 | 3 | 1 | 8 |
| Multiple | 11 (11) | – | 1 | 3 | 1 | 1 | – | 5 | |
| North America | 7 (7) | – | 3 | 2 | – | – | – | 2 | |
| Other | 15 (14) | – | 1 | 6 | 5 | – | – | 3 | |
| UK | 19 (18) | 2 | 3 | 8 | 0 | 1 | – | 5 | |
| Publication year | 2011–2014 | 10 (10) | – | 2 | 3 | – | 8 | – | 5 |
| 2015–2018 | 36 (35) | – | 7 | 14 | 8 | 1 | – | 5 | |
| 2019–2023 | 58 (56) | 3 | 9 | 24 | 4 | 4 | 1 | 13 | |
| Single or multicentre study | Single centre | 76 (73) | 3 | 17 | 32 | 7 | 2 | 1 | 13 |
| Multicentre | 20 (19) | – | – | 4 | 5 | 2 | – | 7 | |
| Not reported | 8 (8) | – | 1 | 4 | – | – | – | 3 | |
| Number of surgeons performing the intervention | 1–2 | 39 (38) | 2 | 8 | 14 | 2 | 2 | – | 10 |
| 3–7 | 16 (15) | 0 | 1 | 8 | 3 | – | – | 4 | |
| >8 | 2 (2) | 1 | – | – | – | – | 1 | – | |
| Not reported/unclear | 47 (45) | – | 9 | 18 | 7 | 3 | – | 9 | |
| Number of participants | 1–10 | 21 (20) | 1 | 12 | 5 | – | – | – | 3 |
| 11–50 | 51 (49) | 2 | 6 | 31 | 3 | – | – | 8 | |
| 51–100 | 13 (13) | – | – | 4 | 2 | 3 | – | 4 | |
| 101–400 | 14 (13) | – | – | 1 | 5 | 1 | – | 7 | |
| >400 | 5 (5) | – | – | – | 2 | 1 | 1 | 1 | |
| Modification category/themes derived from the data | Number of reported modifications (n=425) | |
|---|---|---|
| Procedural | Total=283 (66.6%) | |
| Technical | 225 (79.5%) | |
| Non-technical | 4 (1.4%) | |
| Conversions or abandonments | 54 (19.1%) | |
| Device | Total=94 (22.1%) | |
| Technical | 92 (97.9%) | |
| Non-technical | 0 (0%) | |
| Conversions or abandonments | 2 (2.1%) | |
| Patient selection criteria | Total=48 (11.3%) | |
- —http://dx.doi.org/10.13039/501100000297Royal College of Surgeons of England
- —http://dx.doi.org/10.13039/501100000265Medical Research Council
- —http://dx.doi.org/10.13039/100015250NIHR Bristol Biomedical Research Centre
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealth and Medical Research Impacts
Introduction
Over 10 million surgical procedures are undertaken every year in the UK, with forecasted costs estimated to be close to £9.5 billion.1 2 Surgical innovation is critical to advance treatments and improve patient outcomes, yet it often lacks rigorous evaluation. This can mean potentially harmful procedures, devices and techniques become widespread, before their risks are recognised. High-profile examples with disastrous consequences for patients include silicone breast implants,3 vaginal mesh4 and metal-on-metal hip replacements.5 A 2020 independent safety review led by Baroness Cumberlege identified fundamental failings in existing mechanisms for evaluating surgical innovation and recommended robust evaluation in line with the scrutiny applied to pharmacological interventions.6 This, however, is challenging because surgical innovation occurs very differently from the development and evaluation of new drugs. Surgical innovations, for example, may often undergo incremental and iterative modification (for example, refinements or changes in technique) by surgeons as they perform more cases. Many of these modifications are not documented, reported or shared, as current evaluation systems are not designed to capture such changes.
The Idea, Development, Exploration, Assessment, Long-term follow-up (IDEAL) recommendations, introduced in 2009 to improve the introduction and evaluation of innovative surgical procedures,7 recognise the above challenges. Further updates have since been published to provide practical guidance on applying IDEAL in practice,8 9 yet while use of the framework has increased, there have been challenges in widespread adoption.915 The IDEAL framework suggests that modifications tend to occur in the development stage before an innovative procedure reaches stability, yet it also states that modifications can occur in the exploration stage as the procedure is approaching readiness for definitive evaluation.16 In comparison, the IDEAL guidelines for device evaluation (IDEAL-D) suggest that most modifications occur in a preclinical stage.17 18 The IDEAL framework, therefore, highlights the importance and benefit of reporting modifications, but practical guidance and the conceptualisation of both modifications and stability are lacking.19 If modifications cannot be identified and reported, the point at which an innovation stops evolving and becomes sufficiently stabilised for definitive evaluation may be difficult to recognise.
There is currently no widely accepted definition for modifications in surgical innovation,20 and different terms have been used interchangeably in the literature, such as “variations”, “refinements”, “tinkering” or “alterations”.2123 This contributes to a heterogeneous and inconsistent approach to reporting surgical innovation research and evaluating new surgical procedures and devices, both being recognised problems in the existing literature.24 25 Relevant literature suggests that modifications likely cover a broad spectrum of changes, such as changes to the technical components of a procedure or device, to co-interventions (ie, interventions that occur before, during or after the primary intervention under evaluation)26 and to the characteristics of patients who are offered the intervention.20 27 Decisions to make modifications are often based on individual surgeons’ reflections and experiences of using an innovation in clinical practice. These decisions and practices, however, can be siloed and modifications may not be well-documented or shared with other surgeons.28 This creates a lack of transparency surrounding ‘successful’ and ‘unsuccessful’ modifications, hampers efficient evaluation and creates variation between surgeons and centres. Importantly, this can potentially perpetuate patient harm by inadvertently repeating modifications that can negatively impact patient outcomes. Work to understand modifications in more detail and how best to report them is needed. A review of surgical innovation studies focusing on modification reporting has not yet been undertaken. This systematic review examined the recent practices for reporting modifications in studies following the IDEAL/IDEAL-D framework to inform the development of guidance for identifying and reporting modifications in surgical innovation.
Methods
A study protocol was drafted a priori and prospectively registered on the PROSPERO database (CRD42023427704).29 This study is reported according to Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) recommendations.30
Search strategy
Our strategy to identify studies that followed the IDEAL/IDEAL-D framework involved two steps. First, electronic searches were undertaken to identify studies that cited any of the 13 key IDEAL/IDEAL-D framework publications and guideline papers.79 1618 23 31 Searches were performed in Scopus and Web of Science databases because they have superior functionality for thorough and accurate citation searches (eg, identifying records that have cited any of the 13 key IDEAL/IDEAL-D studies) than other databases.38 39 Date limitations to search for publications from 2019 onwards were applied, as studies published before this date were sourced from an existing review of IDEAL/IDEAL-D studies.40 Searches were performed in July 2023, and results were migrated into V.20 of EndNote.41 Second, records were reduced to only select those that had included the words ‘IDEAL’ or ‘IDEAL-D’ in the title or abstract. This approach for identifying and focusing on IDEAL/IDEAL-D studies as the foundation for this review was based on the rationale that authors of studies aligned to the IDEAL framework are more likely to have considered the importance of reporting modifications, providing a suitable data source for examining recent practices. This strategy to identify IDEAL/IDEAL-D studies was based on an existing review of outcome measurement and reporting in IDEAL-cited studies published in 2020.40 Further details related to the search strategy can be found in online supplemental file 1.
Study selection
Eligible publications for inclusion were primary research studies involving innovative, invasive procedures and devices.40 A pre-existing definition of invasive procedures was used: ‘purposeful or deliberate access to the body gained via an incision, percutaneous puncture, where instrumentation is used in addition to the puncture needle or instrumentation via a natural orifice’.42 Studies in which innovative invasive procedures/devices were co-interventions (eg, radiological imaging for radiologically guided invasive biopsy) were also included due to their potential value in identifying modifications relevant to evaluating surgical innovation. Systematic reviews, book chapters, letters, commentaries, conference proceedings, technical notes, abstracts, editorials and non-English-language publications were excluded.
Records were exported into electronic software (Rayyan)43 to facilitate the screening process. Screening of titles and abstracts for potential eligibility was undertaken by one reviewer (JO), with 10% of records independently screened by a second reviewer (RM) for validation.44 This sample was selected randomly by alphabetising the records by title and selecting every 10th study. Next, full texts of potentially relevant records were obtained via online sources or by contacting authors. Two independent reviewers (JO and RM) screened all full texts to confirm inclusion. Any discrepancies were discussed and resolved with the wider study group. All full-text papers identified from the screening process were supplemented with studies identified in an existing review of IDEAL/IDEAL-D studies that focused on outcome reporting.40 This provided a comprehensive data source of IDEAL/IDEAL-D studies published since the establishment of the IDEAL framework in 2009.
Data extraction and analysis
A standardised data extraction form was developed and piloted by the study team and used for secure electronic data capture and storage in REDCap software.45 One reviewer (JO) extracted data chronologically for each publication, from the newest study to the oldest. The review team held regular meetings to ensure agreement on the approach to data extraction and the data types extracted.
Study characteristics
Details of the innovation, year of publication, number of participating centres and surgeons, number of patients and geographical origins of the study were extracted.
IDEAL stages
The IDEAL stage or stages allocated to studies by authors were extracted. If the authors did not state a specific IDEAL stage, reviewers collectively allocated an IDEAL stage or stages to the study based on a published decision aid to help identify the IDEAL stage of innovation from literature reports.9
Modifications
Any details on modifications, including those relevant to the technical components of the procedure or device, to co-interventions or to patients selected for the procedure, were extracted verbatim. Any contextual information or stated rationale relevant to these modifications was also extracted.46 All verbatim data relating to modifications were then exported from REDCap into NVivo V,12 Pro.47 The Review question, Epistemology, Time/Timescale, Resources, Expertise, Audience and purpose, Type of data criteria48 identified that thematic synthesis would enable the categorisation of findings and subsequent development of themes (patterns in the data).49 This involved line-by-line coding, where text segments were systematically assigned codes (eg, ‘labels’). These were iteratively developed as the analysis progressed until no further themes were identified (eg, saturation of thematic synthesis was achieved). Throughout this process, the primary reviewer (JO) met regularly with the review team to reflect on analysis findings and ensure consistency in approach.
Patient and public involvement
The concept of this research was informed by a public engagement event (FUTURES Festival of Discovery, UKRI funded) held on the SS Great Britain, Bristol. Here, members of the public participated in conversations around innovation in surgery and the role of modification identification and reporting in this process. They also interacted with a life-size ‘Operation Game’ (Altitude Events, Felbridge, UK) and written materials around the work undertaken in the Bristol Biomedical Research Centre. Members of the public highlighted the importance of transparency around modifications to innovative devices and procedures with foreseeable benefits in safety and efficiency of innovation. The review is also part of broader work within the National Institute for Health and Care Research Bristol Biomedical Research Centre Surgical Innovation theme, which regularly undertakes patient and public involvement and engagement activities around surgical innovation to develop ideas, consult on study design and seek advice. Due to its methodological focus, patients or members of the public were not directly involved in this systematic review’s data collection or analysis.
Results
Database searches identified 1071 unique records, with 157 (14.6%) containing the words ‘IDEAL’ and/or ‘IDEAL-D’ in the title and/or abstract. Following abstract screening, 72 records (45.9%) were identified as potentially eligible and proceeded to full-text review. About 57/72 studies (79.2%) met the eligibility criteria for inclusion after full-text review. Reasons for exclusion are listed in the PRISMA diagram30 (figure 1). Combined with 48 studies identified in the existing review of IDEAL/IDEAL-D studies,40 104 publications were included for data extraction and analysis (see online supplemental file 2 for the complete list of citations). Given the exploratory nature of this review, a risk of bias or quality assessment for the included studies was not undertaken, similar to that of other exploratory reviews of surgical innovation studies.40 50
*PRISMA diagram showing identification, screening and inclusion of studies for review. Reasons for exclusion (999 studies): not including IDEAL/IDEAL-D, wrong publication type or not an invasive procedure/device. 1 record was duplicated between the previous review and this current review therefore resulting in 104 total included publications (not 105). IDEAL, Idea, Development, Exploration, Assessment, Long-term follow-up; IDEAL-D, IDEAL guidelines for device evaluation; PRISMA, Preferred Reporting Items for Systematic reviews and Meta-Analyses.
Study characteristics
Table 1 summarises the key characteristics of all 104 included studies, published between 2011–2023. A detailed description of study characteristics is provided in online supplemental file 2. Study reports made up 87 (83.7%) of the publications and 17 (16.3%) were protocols. Case series (n=62, 59.6%) and cohort studies (n=22, 21.2%) were the most frequent study design types, whereas only six (5.8%) were randomised controlled trials. The most common innovation types reported were procedures (n=71, 68.3%) and devices (n=24, 23.1%). These innovations arose from 11 surgical specialities, with urology being the most highly represented (n=38, 36.5%). The number of centres included per study varied from 1 to 40, with a wide range of study sizes (1–2322 participants). In 45 (43.3%) studies, the number of surgeons/operators was not reported, but the range was 1–28 in studies providing this information.
IDEAL stages, use and interpretation
The number of studies with a single allocated IDEAL stage was 73 (70.2%). This was most commonly IDEAL stage 2a (development), in 41 (39.4%) studies (table 1). 22 (21.2%) studies reported innovations that spanned multiple IDEAL stages. The authors of nine studies (8.7%) did not specify an IDEAL stage. For these studies, the authors of this review collectively determined the IDEAL stage, except for one study that contained insufficient information and was labelled ‘unable to stage’.
The number of included studies citing IDEAL increased over time (figure 2). Most studies aligned closely with IDEAL recommendations and expectations for the various stages of innovation regarding the number of patients, centres and surgeons involved in delivering an innovation. However, there were exceptions, with some studies involving more patients, centres or surgeons than usual for the IDEAL stage of innovation, such as one author-reported stage 1 (idea) study involving 37 patients. Another study reported an initial ex-vivo simulation as stage 1, the first three patients as stage 2a and the subsequent 15 patients as stage 2b. The IDEAL recommendations would typically define these instead as stage 0, stage 1 and stage 2a, respectively. Of the 24 studies reporting on innovative devices, only seven (29.1%) cited the device-specific IDEAL-D framework, whereas 17 (70.9%) solely cited the procedure-specific IDEAL framework, although two (8.3%) of these were published before the issuance of IDEAL-D guidance.
Number of studies citing IDEAL over time (up to July 2023). IDEAL, Idea, Development, Exploration, Assessment, Long-term follow-up.
Modification reporting
Incidence/frequency of reporting
Of the 104 studies included, 76 (73.1%) reported modifications. Full details of studies that did and did not report modifications (with citations) are provided in online supplemental file 2. Although modifications were reported in studies across all IDEAL stages (figure 3), they were most commonly reported in stage 2a studies (n=30/104, 28.8%). In all stages, proportionally more studies reported modifications than those that did not, except for stage 2b (figure 3). Modifications were presented graphically (such as in a table, graph or other visual representation) in 24 (23.1%) studies. Some studies reported modifications solely or predominantly in the online supplemental files instead of within the main paper.
Number of studies reporting any modifications by IDEAL stage. IDEAL, Idea, Development, Exploration, Assessment, Long-term follow-up.
Types of modifications reported
Across the 76 studies reporting modifications, the total number of individual modifications identified and extracted from the studies was 425. The number of modifications reported in a single study ranged from 1 to 19. Most modifications related to surgical procedures (n=283, 66.6%), compared with 94 (22.1%) modifications to devices and 48 (11.3%) modifications to patient selection criteria (table 2). Detailed qualitative analysis (ie, coding) of the extracted modification data identified further subcategories of types of modifications. Modifications were categorised within the procedure and device categories as technical, non-technical and cessation (ie, conversions or abandonments). Technical modifications were the most common type of modifications in each category (n=225 for procedures, n=92 for devices). Technical procedural modifications included changes, additions, repetitions or removals of specific procedure steps, changes in a procedural co-intervention or co-treatment (such as anaesthetic agents), changes in the materials or tools used for the procedure and changes in patient position or approach. Technical device modifications included changes to the components of a device, the number of devices used, the size of a device or how a device is used/applied/inserted. Non-technical modifications included alterations in expertise, personnel or non-technical skills. Modifications to patient selection criteria included changes to inclusion and exclusion criteria across both devices and procedures.
Contextual information
Modifications were often described in the context of the timeframe of the innovation, with some occurring before the current study (ie, in a previous study/use of the procedure or device), some during the study and some proposed as future modifications. The intentionality of modifications was described in six (5.8%) studies, either as preplanned or spontaneous/unplanned (eg, in response to an unexpected event during surgery). Modifications were described in terms of magnitude in only two (1.9%) studies, in which authors used the terms major and/or minor. 44 (42.3%) studies included implications of modifications (ie, any benefits and/or drawbacks).
Language around modification reporting
Examples of non-specific or obfuscating language used around modification reporting were identified across the included papers. For example, it was sometimes unclear if a modification had occurred or was theorised as a hypothetical solution to a potential problem. In some studies, the presence of modifications was alluded to but without sufficient detail to allow the reader to learn from it, such as, ‘ The intervention needed to be refined’ or ‘With the refinement of the technique and the rising learning curve, these side events did not occur again’. A wide array of alternative terms for modifications or the process of modifying an innovation were identified across the study reports, although none of the studies included definitions for any of these terms. Examples included adaptations, additions, adjustments, alterations, changes, choices, combinations, developed, expanded, evolve, fine-tune, optimise, improvements, increments, introduced, optimised, refinements, replacing, reverted, solutions and substituted.
Discussion
This review examined primary literature around surgical innovation, focusing on understanding recent reporting practices of modifications to innovative procedures and devices. Within the 104 included studies, wide heterogeneity in the study methods, patient numbers and level of modification reporting was observed. Over a quarter of the included studies did not report or contain any mention of modifications. Where modifications were reported, this occurred across all IDEAL stages but were most frequently in IDEAL stage 2a studies (n=30, 28.8%). There was a preponderance of technical (as opposed to non-technical) modifications; however, the depth and breadth of modification reporting varied noticeably. Some authors reported multiple modifications in detail and included text about the benefits of doing so (such as transparency and shared learning), yet modification reporting itself was inconsistent.
The IDEAL framework recognises the importance of reporting modifications, particularly in stage 2a, but lacks clarity over how this should be done in practice.7 17 This emphasis on modification reporting in early innovation may be reflected in the frequency of modification reporting in stage 2a studies within this review. The observed variation in modification reporting in other IDEAL stages may be partly due to a lack of guidance on identifying and reporting modifications in surgical innovation, particularly in non-stage 2a studies.19 The studies included in this review demonstrated inconsistent approaches to implementing and using IDEAL guidance across all stages, which aligns with findings from previous reviews on the uptake of the IDEAL framework.12 51 This review and qualitative analysis of primary surgical innovation research complements the findings of a scoping review of modification discussions in secondary research (opinion pieces and reviews) across 49 studies up to October 2020.20 Overlap in some conceptual themes was seen, particularly around the contextual details of modifications (including what, when, why and so what).20
Detailed qualitative analysis of the extracted data around modifications and their contextual details identified some studies with particularly rich reporting of modifications.5255 These studies often contained strategies for identifying modifications, such as prospective data capture on a case-by-case basis and using embedded qualitative methods, such as interviewing the users of an innovation after each case or examining their written journals/materials (eg, operation notes). This allows the recording of detailed contextual details around modifications, including what was changed, when modifications occurred (ie, which patients), why they were implemented (ie, the rationale) and their impact (ie, the benefits and drawbacks). Reporting these details may help to facilitate shared learning between innovators and the surgical/research community by providing a more detailed understanding of the modifications and their implications for the evolution and evaluation of the innovation. At times, the presentation of these contextual details was optimised with graphical representations of modifications and the use of the prospective development study format advocated for stage 2a studies by the IDEAL framework.9 35 When reporting multiple IDEAL stages, some authors specified which modifications occurred within each specific stage, either described throughout the study or as a summary with key learning points in the discussion section. Some authors reflected on the iterative nature of innovation and the role of modifications concerning stability and the learning curve. In commenting on the process of reaching stability (ie, when the frequency of modifications is reduced), the context of the modifications and the innovation is set for the reader. Using these strategies when identifying, evaluating and reporting modifications to surgical innovations could significantly contribute to addressing the failures identified in the Cumberlege safety report.6
To our knowledge, this is the first systematic review of primary literature around surgical innovation that has examined the reporting of modifications. The 104 studies covered all stages of innovation, including multiple types of innovations published across 12 years, providing sufficient information to establish reporting practices across the literature via a representative sample. Additionally, this study adopted a broad inclusion strategy for identifying any modifications to devices, procedures or patient selection criteria, which was undertaken based on a lack of an accepted definition for modifications.20 Despite these strengths, potential limitations must be recognised. Only two databases have the functionality required for reliable citation searching38 39; therefore, studies not indexed in these databases could have been missed. Non-English language publications and grey literature were not included for pragmatic reasons due to resource limitations. Therefore, some potentially relevant studies could have been missed. Only studies that cited IDEAL/IDEAL-D and included these words within the title and/or abstract were included. This strategy was employed as it was felt that those authors actively engaging with and using current best practices were most likely to include thorough modification reporting. It is acknowledged that studies following the IDEAL framework but not specifying this in the abstract/title or those not citing IDEAL at all would not have been identified by the current search strategy, which might introduce an element of bias. The original IDEAL framework was published in 20097; therefore, studies published pre-2009 were not included. However, the authors believe that reporting standards are likely to have improved since the publication of the IDEAL framework compared with more historical publications. The final limitation is that this review does not contain any studies after July 2023 (when data searches were conducted).
This review has found that modification reporting is inconsistent and unreliable in surgical innovation research, particularly in non-stage 2a studies. Developing a tool for identifying and reporting modifications has the potential to improve shared learning, enhance the evaluation and implementation of surgical innovation and reduce patient risks. The findings from this review and analysis are currently being used to develop a checklist that will allow surgeons to identify and report modifications across all stages of surgical innovation in a systematic, pragmatic and standardised fashion. This checklist will be able to be used alongside the IDEAL framework and complement conceptual work around modifications.20 The detailed qualitative findings from this review will be presented in future publications when synthesised and combined with findings from subsequent indepth stakeholder interviews. It has previously been shown that surgeons often struggle to distinguish between innovation and variation, which has facilitated work on defining surgical innovation.25 A tool has been developed to define innovation and enable surgeons to identify innovations and distinguish them from variations (or modifications).24 56 The checklist that is being developed from this review will complement this tool by clarifying how to identify and report modifications. It will also enable the operationalisation of the 2023 COHESIVE core outcome set (a consensus agreed set of outcomes to measure and report, as a minimum, in all early-phase studies evaluating novel surgical procedures/devices) in which modifications were one of the eight core domains in the agreed core set.27
Supplementary material
10.1136/bmjopen-2024-097097online supplemental file 1
10.1136/bmjopen-2024-097097online supplemental file 2
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Abbott TEF Fowler AJ Dobbs TD et al Frequency of surgical treatment and related hospital procedures in the UK: a national ecological study using hospital episode statistics Br J Anaesth 20171192495710.1093/bja/aex 13728854546 · doi ↗ · pubmed ↗
- 2FTN Briefing: operating theatres - maximising a valuable resource 20142014 Availablehttps://nhsproviders.org/media/1128/operating-theatres-final.pdf
- 3Greco C The Poly Implant Prothèse breast prostheses scandal: Embodied risk and social suffering Soc Sci Med 2015147150710.1016/j.socscimed.2015.10.06826584233 · doi ↗ · pubmed ↗
- 4Heneghan C Aronson JK Goldacre B et al Transvaginal mesh failure: lessons for regulation of implantable devices BMJ 2017 j 551510.1136/bmj.j 551529217786 · doi ↗ · pubmed ↗
- 5Cohen D How safe are metal-on-metal hip implants?BMJ 2012344 e 141010.1136/bmj.e 141022374741 · doi ↗ · pubmed ↗
- 6Medicines I Medical devices safety review: first do no harm—the report of the immdsreview 202010.1177/0036933021105846734994662 · doi ↗ · pubmed ↗
- 7Mc Culloch P Altman DG Campbell WB et al No surgical innovation without evaluation: the IDEAL recommendations The Lancet 200937411051210.1016/S 0140-6736(09)61116-819782876 · doi ↗ · pubmed ↗
- 8Hirst A Philippou Y Blazeby J et al No Surgical Innovation Without Evaluation Ann Surg 20192692112010.1097/SLA.000000000000279429697448 · doi ↗ · pubmed ↗