Hidden in Plain Sight: Delayed Diagnosis of Poorly Cohesive Gastric Carcinoma in a Young Male Patient
Tyler R Ellett, Andrew Pippas, Humberto Rios, William F Willett, Maria B Diaz

TL;DR
A young man with persistent heartburn was later diagnosed with aggressive gastric cancer, highlighting the need for earlier screening in young adults.
Contribution
This case emphasizes the rising incidence of early-onset gastric cancer and the importance of timely diagnosis in young patients.
Findings
The patient had non-hereditary, poorly cohesive gastric adenocarcinoma despite H. pylori treatment and acid suppression.
Persistent pyrosis in young adults may be an early sign of gastric cancer and warrants closer monitoring.
Early-onset gastric cancer is increasing and differs from late-onset cases in etiology and presentation.
Abstract
Poorly cohesive gastric adenocarcinoma is classified as a diffuse type of gastrointestinal tract tumor composed of undifferentiated cells with an inherent propensity for aggressive behavior. Recent trends in surveillance indicate that gastric cancer (GC) is affecting younger adults and is distinct from GC that occurs later in life. Early-onset gastric cancer (EOGC) is associated with various environmental and genetic factors. Younger patients with recurrent pyrosis may warrant earlier surveillance in light of this worrisome trend. Herein, we discuss a young male patient who developed non-hereditary, poorly cohesive gastric adenocarcinoma with an extended history of pyrosis despite long-term acid suppression and triple therapy for Helicobacter pylori (H. pylori).
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
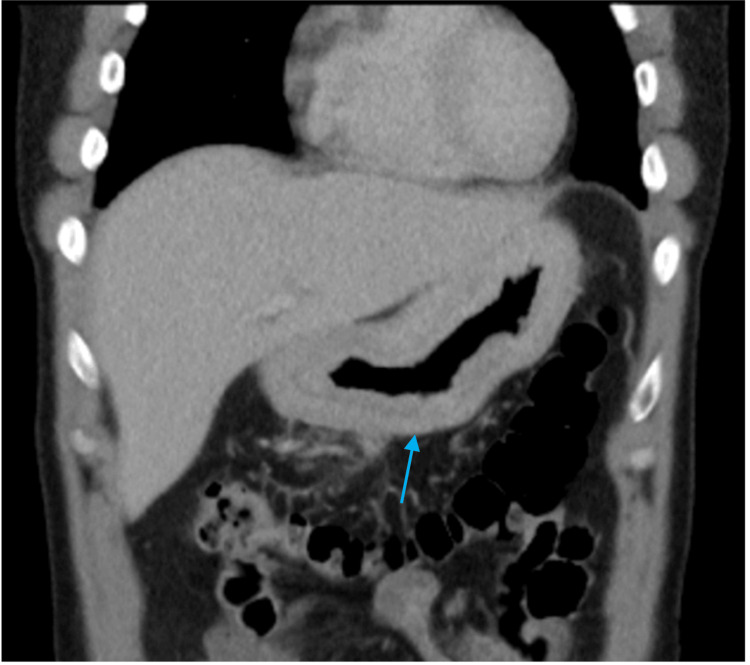 Figure 1
Figure 1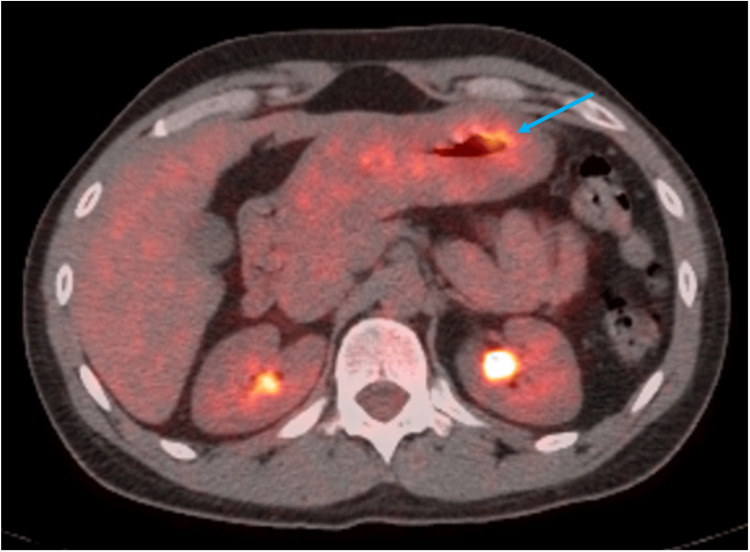 Figure 2
Figure 2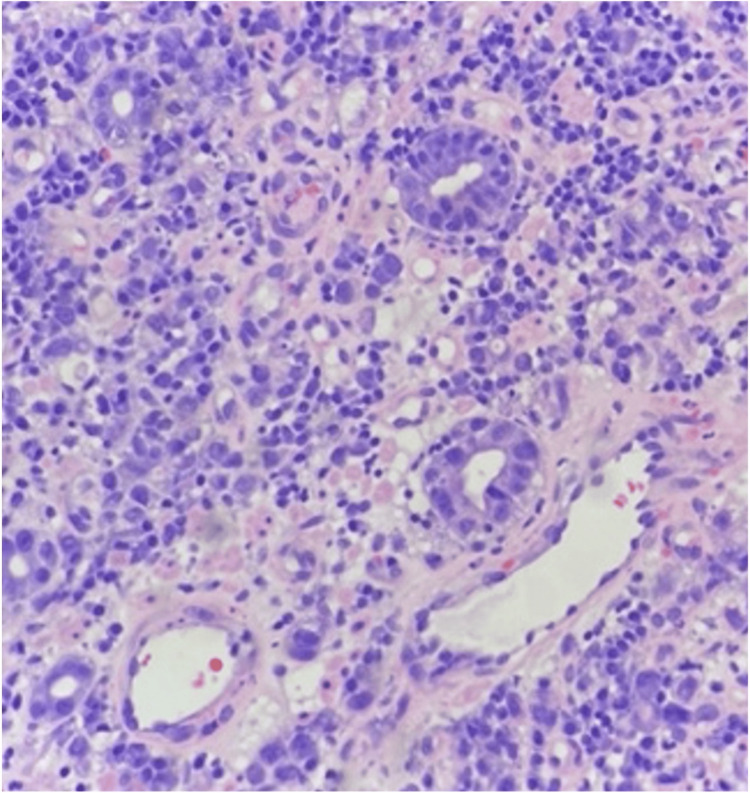 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal disorders and treatments · Ovarian cancer diagnosis and treatment
Introduction
Despite significant advancements, gastric cancer (GC) remains the fifth most common cancer and the fifth leading cause of cancer-related death [1]. In the United States, 30% of new GC cases occur in young adults, with a strong association to diffuse-type histology, higher grade, and metastatic disease [2]. The mechanisms for this are still poorly understood. Known environmental risk factors appear less prominent when compared to later-onset GC, and reduced lifetime exposure suggests a hereditary component. Heritable GC accounts for a subset of early-onset cases, with approximately 77% of GC cases being sporadic [3]. Early-onset GC (EOGC), defined as occurring before age 50, is linked to distinct mutations in the BANP, MUC5B, and RHOA genes, epigenetic alterations, and dysbiosis caused by Helicobacter pylori (H. pylori) eradication therapy [4]. Common presenting symptoms include nausea, vomiting, and bloating. Due to a lack of routine or standardized screening, it is often overlooked, leading to a delayed diagnosis.
Case presentation
A previously healthy 41-year-old Nigerian male patient presented to the emergency department with a chief complaint of discomfort in the stomach with associated bloating and diarrhea. The initial onset of abdominal pain began in 1999, with subsequent visits for similar discomfort in 2009, 2015, and 2019. He received treatment with cimetidine, omeprazole, and triple therapy for *H. pylori *infection based on clinical suspicion. No testing for confirmation or eradication was performed. He had no prior medical history, surgeries, or medications. His social history was insignificant, and his family history was negative for gastrointestinal disease. Complete blood count and comprehensive metabolic panel were normal. Computed tomography (CT) of the chest, abdomen, and pelvis revealed diffuse gastric wall thickening with heterogeneously enhancing necrotic lymph nodes in the mesentery (Figure 1). Esophagogastroduodenoscopy (EGD) revealed decreased distensibility in the stomach with an ulcerated lesion in the antrum. The pylorus had a linitis plastica-like appearance, and multiple ulcerations with a broad base were noted above the tumoral lesion.
Computed tomography of the abdomen with findings of diffuse gastric wall thickening (blue arrow).
A colonoscopy was conducted and was negative for polyps, masses, or changes consistent with inflammatory bowel disease. Positron emission tomography (PET) demonstrated abnormal fluorodeoxyglucose (FDG) uptake in the mid- to distal gastric body with a maximal diameter of 55 mm (Figure 2). A gastric body biopsy revealed ulcerated, poorly differentiated adenocarcinoma with focal signet ring cell features favoring poorly cohesive type (Figure 3).
Positron emission tomography with abnormal uptake of fluorodeoxyglucose in the mid- to distal gastric body (blue arrow).
Diffuse-type gastric adenocarcinoma (haematoxylin and eosin staining, 100x magnification), demonstrating discohesive tumor cells.
Giemsa stain was positive for H. pylori organisms. Genetic testing completed by NeoGenomics (NeoGenomics Laboratories, Fort Myers, FL) was negative for human epidermal growth factor receptor 2 (HER2)/neu expression. Programmed death ligand-1 (PD-L1) expression was positive with 15% staining and 2+ intensity. Mismatch repair genes were intact. The patient was initiated on a neoadjuvant chemotherapy regimen consisting of docetaxel, cisplatin, and 5-fluorouracil (DCF) prior to planned total gastrectomy.
Discussion
EOGC rates are rising, particularly in low-incidence countries in Europe, Oceania, and the Americas. Key risk factors of GC include family history, smoking, obesity, gastroesophageal reflux disease (GERD), high salt intake, alcohol consumption, Epstein-Barr virus, and H. pylori infection [5]. While H. pylori is linked to severe gastric disease and about 3% of infections lead to non-cardia GC, its prevalence has declined globally, indicating other factors in tumor development [6]. In a nationwide population study, alcohol consumption and smoking increased the risk of EOGC in men, but not in women [7]. Proton pump inhibitors (PPIs), commonly used for GERD, are debated concerning their role in gastric carcinogenesis. Early observational studies suggest they may increase the risk of GC, atrophy, and *H. pylori *resistance [8,9]. Recent studies have revealed a significant role of gut microbiome dysbiosis and distinct genomic alterations in the development of EOGC.
Through microbiota sequencing, evidence has demonstrated elevated levels of oral microbiome bacteria in cardia and non-cardia GC cases [10]. In various meta-analyses investigating the association between gastric disease and the microbiome, Streptococcus anginosus (S. anginosus) has emerged as a consistently enriched bacterium following H. pylori eradication, a finding supported by level 1 evidence [11,12]. Generally found in the oral cavity, this bacterium cannot survive at a pH lower than five, and randomized control trials have demonstrated translocation into the gut with PPI use [13]. In a recent article published by Cell Host and Microbe, Fu et al. showed that S. anginosus can activate pro-oncogenic pathways, impair epithelial membrane integrity, and induce inflammation through the ANAX2 host receptor [14]. Their findings highlight a second bacterium or “second hit” in the ‘H. pylori initiation-non-H. pylori acceleration’ cascade. The role of probiotics remains unclear following antibiotic treatment, but supplementation with *Bifidobacterium *and Lactobacillus may partially assist in restoring post-eradication microbial dysbiosis [15].
The Lauren classification, first described in 1965, identifies two types of gastric adenocarcinoma: intestinal and diffuse. As in this case, diffuse gastric adenocarcinoma is marked by poorly differentiated cells with or without signet ring cells that can infiltrate the gastric wall, causing linitis plastica. Unlike the intestinal type, the diffuse type is often genomically stable, and other genetic factors are thought to contribute to EOGC due to limited environmental carcinogen exposure [16]. Tumor biology research has reformed the standard of care for a broad and expanding range of cancers. A number of surface proteins, including the PD-L1 protein and HER2, as well as intracellular deficient mismatch repair (dMMR) proteins, have potential prognostic and predictive implications, although very nuanced and cancer-specific. Conventional treatment for HER2-negative advanced GC is anti-PD-L1-based therapy. The expression of PD-L1 alone has shown limited reliability for predicting immunotherapy effectiveness in GC, particularly in low mutational burden tumors [17]. This is supported by Pietrantonio et al.’s meta-analysis of randomized clinical trials, including KEYNOTE-062, CheckMate-649, JAVELIN Gastric 100, and KEYSTONE-061, demonstrating worse survival outcomes in patients with low microsatellite instability treated with anti-PD-L1-based treatment compared to patients with high microsatellite instability [18]. Aside from targetable proteins and genomic integrity, epigenomic studies provide further insight into EOGC tumor regulation and behavior.
Genome-wide analysis has identified single-nucleotide polymorphisms (SNPs) in XRCC genes and alterations in BANP, MUC5B, RHOA, ARID1A, and TGFBR1 [19,20]. Ge et al. recruited 12 GC patients to show a significant difference in genome-wide methylation expression between patients with EOGC and late-onset GC. The study speculated that hypermethylation of Cg11037477, a promoter region of the eukaryotic translation initiation factor 4E (EIF4E), may lead to deregulation of the well-established oncologic PI3K-AKT pathway. A significant association was found between age at diagnosis and expression of EIF4E with hypermethylation of the promoter region (p<0.05). In addition, the down-expression of EIF4E was associated with poor survival [4]. The patient we describe has an SNP (Gln77Gln) in the XRCC2 gene, which is involved in DNA double-strand repair. As with CDH1, the relevance of XRCC2 with EOGC is not readily established or identified as a hereditary factor. These studies suggest that early-onset GCs show distinct genomic and epigenomic features compared to those that arise later in life.
Conclusions
The prevalence of GC in individuals under 50 years old is increasing, and healthcare practitioners should closely monitor symptoms in this population. Testing for H. pylori, initiating eradication therapy with confirmation of eradication, and practicing judicious use of PPIs may offer clinical benefit, particularly in individuals under 50 with dyspeptic symptoms. Research on the gut microbiome has demonstrated the causality of S. anginosus in gastric tumorigenesis and established a mechanism for oncogenesis. Currently, no guidelines support interval screening with EGD for detecting EOGC; however, genomic testing may help identify individuals at higher risk and justify earlier screening. The risk factors for GC are well established, but more studies are needed to differentiate between early-onset and later-onset GC. Overall, further research into developing primary and secondary prevention strategies is crucial for reducing the burden of GC. This case highlights the importance of considering various risk factors to improve risk stratification and enhance surveillance efforts.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The International Agency for Research on Cancer (IARC): Global Cancer Observatory 6 2025 2022 https://gco.iarc.fr/en
- 2Early-onset gastric cancer is a distinct disease with worrisome trends and oncogenic features Surgery Bergquist JR Leiting JL Habermann EB 54755516620193133168510.1016/j.surg.2019.04.036 · doi ↗ · pubmed ↗
- 3Hereditary gastrointestinal cancers: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up Ann Oncol Stjepanovic N Moreira L Carneiro F Balaguer F Cervantes A Balmaña J Martinelli E 155815713020193137880710.1093/annonc/mdz 233 · doi ↗ · pubmed ↗
- 4Hypermethylation of EIF 4E promoter is associated with early onset of gastric cancer Carcinogenesis Ge Y Wu Q Ma G 66713920182934227310.1093/carcin/bgx 110 · doi ↗ · pubmed ↗
- 5Global, regional, and national burden of early-onset gastric cancer Cancer Biol Med Tan N Wu H Cao M 6676782120243910968410.20892/j.issn.2095-3941.2024.0159 PMC 11359495 · doi ↗ · pubmed ↗
- 6Helicobacter pylori and gastric cancer: factors that modulate disease risk Clin Microbiol Rev Wroblewski LE Peek RM Jr Wilson KT 7137392320102093007110.1128/CMR.00011-10PMC 2952980 · doi ↗ · pubmed ↗
- 7Impact of smoking and alcohol consumption on early-onset gastric cancer development in young Koreans: a population-based study J Gastric Cancer Kang SJ Shin CM Han K 1451582420243857550810.5230/jgc.2024.24.e 2PMC 10995832 · doi ↗ · pubmed ↗
- 8Long-term use of proton-pump inhibitors and risk of gastric cancer: a review of the current evidence Therap Adv Gastroenterol Cheung KS Leung WK 175628481983451112201910.1177/1756284819834511 PMC 641548230886648 · doi ↗ · pubmed ↗