Optimal duration of antimicrobial prophylaxis in patients undergoing distal pancreatectomy: A multicenter cohort study
Kenjiro Okada, Kenichiro Uemura, Sohei Satoi, Tsutomu Fujii, Manabu Kawai, So Yamaki, Toru Watanabe, Hideki Motobayashi, Shinya Takahashi

TL;DR
This study found that giving antibiotics for more than 24 hours after distal pancreatectomy does not reduce infections better than shorter durations.
Contribution
The study provides evidence on the optimal duration of antimicrobial prophylaxis for distal pancreatectomy.
Findings
Shorter antibiotic duration (intraoperative or up to 24 hours) had lower surgical site infection rates.
Prolonged antibiotic use was an independent risk factor for surgical site infections.
No significant difference in severe infection rates between the two groups.
Abstract
Antimicrobial prophylaxis is routinely administered in patients undergoing distal pancreatectomy, with cephalosporins being the most frequently used agents. However, there is limited evidence regarding optimal duration of antimicrobial prophylaxis. This study aimed to evaluate the optimal duration of antimicrobial prophylaxis in distal pancreatectomy. A multicenter cohort study was performed using a common database of patients who underwent distal pancreatectomy between April 2017 and March 2022 at four high‐volume centers in Japan. Eligible patients were divided into two groups according to the duration of antimicrobial prophylaxis: intraoperative or up to 24 h after surgery and more than 24 h after surgery. Primary endpoint was the incidence of surgical site infections. A total of 496 patients were enrolled in this study, including 254 and 242 patients categorized into the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
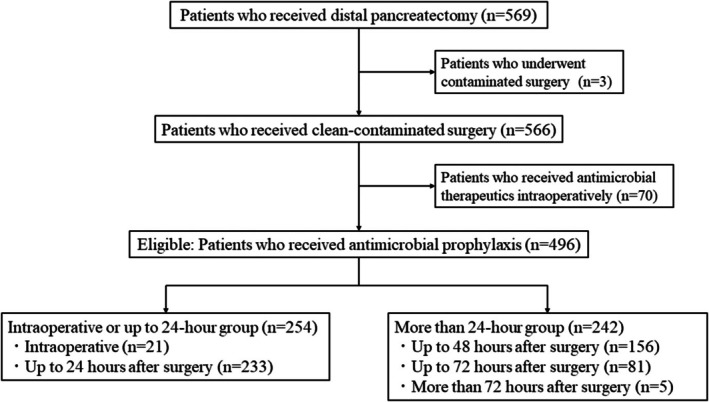 FIGURE 1
FIGURE 1| Factors | Antimicrobial prophylaxis |
| |
|---|---|---|---|
| Intraoperative or up to 24‐h, | More than 24‐h, | ||
| Patient demographics | |||
| Age, ≥80 years | 42 (17) | 33 (14) | 0.367 |
| Sex, female | 140 (55) | 118 (49) | 0.157 |
| BMI, ≥22 kg/m2 | 120 (47) | 118 (49) | 0.736 |
| ASA‐PS, ≥3 | 20 (8) | 35 (14) | 0.019 |
| Cardiovascular disease | 25 (10) | 39 (16) | 0.037 |
| Pulmonary disease | 14 (6) | 42 (17) | <0.001 |
| Diabetes | 74 (29) | 86 (36) | 0.127 |
| Laparotomy | 70 (28) | 85 (35) | 0.069 |
| Smoking | 70 (28) | 89 (37) | 0.028 |
| Steroids | 5 (2) | 3 (1) | 0.517 |
| PNI, <45 | 59 (23) | 64 (26) | 0.407 |
| Pancreatic disease, malignant | 161 (63) | 120 (50) | 0.002 |
| Neoadjuvant therapy | 80 (32) | 81 (33) | 0.639 |
| Procedures, minimally invasive | 108 (43) | 102 (42) | 0.933 |
| Texture of pancreas, soft | 202 (80) | 221 (91) | <0.001 |
| Thickness of pancreas transection, ≥15 mm | 79 (31) | 79 (33) | 0.713 |
| Method of pancreas transection, stapler | 221 (87) | 226 (93) | 0.016 |
| Vascular resection | 22 (9) | 25 (10) | 0.526 |
| Organ resection | 26 (10) | 22 (9) | 0.666 |
| Operation time, ≥300 min | 87 (34) | 118 (49) | 0.001 |
| Estimated blood loss, ≥400 mL | 65 (26) | 73 (30) | 0.256 |
| Transfusion | 14 (6) | 17 (7) | 0.486 |
| Postoperative outcomes | |||
| Surgical site infections | 49 (19) | 80 (33) | <0.001 |
| Superficial | 5 (2) | 10 (4) | 0.156 |
| Deep | 2 (1) | 2 (1) | 0.961 |
| Organ/space | 43 (17) | 70 (29) | 0.001 |
| Infectious CR‐POPF | 20 (8) | 41 (17) | 0.002 |
| CD ≥IIIa | 24 (9) | 20 (8) | 0.643 |
| Remote infections | 7 (3) | 3 (1) | 0.223 |
| Non‐infectious postoperative complications | 44 (17) | 47 (19) | 0.546 |
| Non‐infectious CR‐POPF | 6 (2) | 13 (5) | 0.078 |
| Postoperative hospital stays | 13 (IQR, 9–18) | 17 (IQR, 12–26) | <0.001 |
| Readmission | 17 (7) | 8 (3) | 0.081 |
| 90‐day mortality | 0 | 1 (0.4) | 0.231 |
| Factors | Antimicrobial prophylaxis |
| |
|---|---|---|---|
| Intraoperative or up to 24‐h, | More than 24‐h, | ||
| Patient demographics | |||
| Age, ≥80 years | 27 (15) | 25 (14) | 0.764 |
| Sex, female | 100 (55) | 96 (53) | 0.673 |
| BMI, ≥22 kg/m2 | 82 (45) | 88 (49) | 0.527 |
| ASA‐PS, ≥3 | 15 (8) | 18 (10) | 0.584 |
| Cardiovascular disease | 20 (11) | 17 (9) | 0.603 |
| Pulmonary disease | 14 (8) | 7 (4) | 0.112 |
| Diabetes | 55 (30) | 64 (35) | 0.314 |
| Laparotomy | 51 (28) | 62 (34) | 0.212 |
| Smoking | 58 (32) | 56 (31) | 0.821 |
| Steroids | 4 (2) | 1 (1) | 0.162 |
| PNI, <45 | 43 (24) | 41 (23) | 0.803 |
| Pancreatic disease, malignant | 102 (56) | 91 (50) | 0.246 |
| Neoadjuvant therapy | 50 (28) | 63 (35) | 0.140 |
| Procedures, minimally invasive | 85 (47) | 83 (46) | 0.833 |
| Texture of pancreas, soft | 166 (92) | 162 (90) | 0.471 |
| Thickness of pancreas transection, ≥15 mm | 53 (29) | 52 (29) | 0.908 |
| Method of pancreas transection, stapler | 169 (93) | 168 (93) | 0.836 |
| Vascular resection | 14 (8) | 22 (12) | 0.158 |
| Organ resection | 16 (9) | 13 (7) | 0.561 |
| Operation time, ≥300 min | 72 (40) | 77 (43) | 0.593 |
| Estimated blood loss, ≥400 mL | 41 (23) | 48 (27) | 0.393 |
| Transfusion | 9 (5) | 10 (6) | 0.814 |
| Postoperative outcomes | |||
| Surgical site infections | 34 (19) | 59 (33) | 0.003 |
| Superficial | 2 (1) | 9 (5) | 0.026 |
| Deep | 1 (1) | 1 (1) | 1.000 |
| Organ/space | 31 (17) | 53 (29) | 0.006 |
| Infectious CR‐POPF | 14 (8) | 31 (17) | 0.006 |
| CD ≥IIIa | 16 (9) | 16 (9) | 1.000 |
| Remote infections | 5 (3) | 2 (1) | 0.245 |
| Non‐infectious postoperative complications | 28 (15) | 34 (19) | 0.402 |
| Non‐infectious CR‐POPF | 5 (3) | 11 (6) | 0.121 |
| Postoperative hospital stays | 13 (IQR, 9–17) | 16 (IQR, 12–26) | <0.001 |
| Readmission | 12 (7) | 7 (4) | 0.236 |
| 90‐day mortality | 0 | 1 (0.6) | 0.239 |
| Factors | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| Surgical site infection |
| OR | 95% CI |
| ||
| Yes, | No, | |||||
| Age, years | ||||||
| <80 | 107 (83) | 314 (86) | 0.481 | |||
| ≥80 | 22 (17) | 53 (14) | ||||
| Sex | ||||||
| Male | 65 (50) | 173 (47) | 0.525 | |||
| Female | 64 (50) | 194 (53) | ||||
| BMI, kg/m2 | ||||||
| <22 | 58 (45) | 200 (55) | 0.062 | |||
| ≥22 | 71 (55) | 167 (45) | ||||
| ASA‐PS | ||||||
| ≤2 | 114 (88) | 327 (89) | 0.821 | |||
| ≥3 | 15 (12) | 40 (11) | ||||
| Cardiovascular disease | ||||||
| Yes | 20 (16) | 44 (12) | 0.314 | |||
| No | 109 (84) | 323 (88) | ||||
| Pulmonary disease | ||||||
| Yes | 16 (12) | 40 (11) | 0.645 | |||
| No | 113 (88) | 327 (89) | ||||
| Diabetes | ||||||
| Yes | 43 (33) | 117 (32) | 0.762 | |||
| No | 86 (67) | 250 (68) | ||||
| Laparotomy | ||||||
| Yes | 42 (33) | 113 (31) | 0.710 | |||
| No | 87 (67) | 254 (69) | ||||
| Smoking | ||||||
| Yes | 49 (38) | 110 (30) | 0.097 | |||
| No | 80 (62) | 257 (70) | ||||
| Steroids | ||||||
| Yes | 2 (2) | 6 (2) | 0.948 | |||
| No | 127 (98) | 361 (98) | ||||
| PNI | ||||||
| <45 | 33 (26) | 90 (25) | 0.811 | |||
| ≥45 | 96 (74) | 277 (75) | ||||
| Pancreatic disease | ||||||
| Borderline/benign | 58 (45) | 157 (43) | 0.667 | |||
| Malignant | 71 (55) | 210 (57) | ||||
| Neoadjuvant therapy | ||||||
| Yes | 37 (29) | 124 (34) | 0.283 | |||
| No | 92 (71) | 243 (66) | ||||
| Procedures | ||||||
| Minimally invasive | 55 (43) | 155 (42) | 0.937 | |||
| Open | 74 (57) | 212 (58) | ||||
| Antimicrobial prophylaxis | ||||||
| Intraoperative or up to 24 h | 49 (38) | 205 (56) | <0.001 | 1.0 | 0.001 | |
| More than 24 h | 80 (62) | 162 (44) | 2.04 | 1.32–3.14 | ||
| Texture of pancreas | ||||||
| Soft | 105 (81) | 318 (87) | 0.156 | |||
| Firm | 24 (19) | 49 (13) | ||||
| Thickness of pancreas transection, mm | ||||||
| <15 | 75 (58) | 263 (72) | 0.005 | 1.0 | 0.023 | |
| ≥15 | 54 (42) | 104 (28) | 1.65 | 1.07–2.54 | ||
| Method of pancreas transection | ||||||
| Stapler | 109 (85) | 338 (92) | 0.017 | 1.0 | 0.022 | |
| Non‐stapler | 20 (15) | 29 (8) | 2.13 | 1.11–4.06 | ||
| Vascular resection | ||||||
| Yes | 18 (14) | 29 (8) | 0.052 | |||
| No | 111 (86) | 338 (92) | ||||
| Organ resection | ||||||
| Yes | 13 (10) | 35 (10) | 0.859 | |||
| No | 116 (90) | 332 (90) | ||||
| Operation time, min | ||||||
| <300 | 56 (43) | 235 (64) | <0.001 | 1.0 | 0.003 | |
| ≥300 | 73 (57) | 132 (36) | 1.92 | 1.26–2.93 | ||
| Estimated blood loss, mL | ||||||
| <400 | 85 (66) | 273 (74) | 0.068 | |||
| ≥400 | 44 (34) | 94 (26) | ||||
| Transfusion | ||||||
| Yes | 10 (8) | 21 (6) | 0.423 | |||
| No | 119 (92) | 346 (94) | ||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatic and Hepatic Oncology Research · Surgical site infection prevention · Gallbladder and Bile Duct Disorders
INTRODUCTION
1
Antimicrobial prophylaxis is essential for the management of postoperative infections in gastrointestinal surgery, which is associated with a higher incidence of surgical site infections than other surgeries. The appropriate use of antimicrobial prophylaxis is important, as prolonged administration of antimicrobial prophylaxis can result in antimicrobial resistance or microbial substitution. The World Health Organization guidelines1 or American clinical practice guidelines2 for preventing surgical site infections recommend that antimicrobial prophylaxis be administered intraoperatively or up to 24 h after surgery, with cephalosporins being the most frequently used agents for gastrointestinal procedures. Several randomized clinical trials of antimicrobial prophylaxis for gastrectomy3, 4, 5 and colectomy6 have been performed. With regards to elective gastrectomy for gastric cancer, intraoperative administration of antimicrobial prophylaxis did not increase the incidence of surgical site infections compared to postoperative administration and is therefore recommended for intraoperative use only. However, with respect to elective colectomy for colorectal cancer, it is unclear whether there is a difference in the usefulness of intraoperative administration alone and postoperative administration. Furthermore, there is little evidence regarding the optimal duration of antimicrobial prophylaxis in gastrointestinal surgical procedures other than gastrectomy and colorectal resection (i.e., esophageal surgery, hepatobiliary, and pancreatic surgery).7
Pancreatic surgery has a high risk of surgical site infection, and antimicrobial prophylaxis is widely used for varying durations postoperatively. Pancreatoduodenectomy includes pancreatic anastomosis and gastrointestinal reconstruction. The incidence of postoperative infectious complications, including postoperative pancreatic fistula (POPF), is relatively higher than that for other gastrointestinal surgeries.8, 9 A randomized clinical trial10 reported that single‐day prophylactic use was appropriate for pancreatoduodenectomy following biliary drainage without cholangitis, which can increase the risk of postoperative infectious complications.11 In distal pancreatectomy, the incidence of postoperative complications, including POPF, remains high at 10–30%.12, 13 However, distal pancreatectomy does not involve gastrointestinal anastomosis, and the incidence of postoperative infections could be relatively lower than that after pancreatoduodenectomy. From the viewpoint of upper abdominal surgery, gastrectomy may be comparable to distal pancreatectomy, and evidence from randomized controlled trials3, 4, 5 suggests that intraoperative or up to 24‐h antimicrobial prophylaxis may be appropriate for distal pancreatectomy. Nevertheless, the types of postoperative complications differ significantly between gastrectomy and distal pancreatectomy. As a result, the optimal duration of antimicrobial prophylaxis for distal pancreatectomy remains unclear. Therefore, this large‐scale multicenter cohort study was conducted to evaluate the optimal duration of antimicrobial prophylaxis in distal pancreatectomy.
METHODS
2
Study design
2.1
This multicenter cohort study included patients who underwent distal pancreatectomy for pancreatic disease between April 2017 and March 2022 at four high‐volume surgical institutions in Japan: Kansai Medical University Hospital, Toyama University Hospital, Wakayama Medical University Hospital, and Hiroshima University Hospital. First generation cephalosporins were generally administrated as perioperative antimicrobial prophylactic agents in this study, and second generation cephalosporins were also administrated when first generation cephalosporins could not be used during the study period. Patients who underwent contaminated surgery were excluded from this study. Patients who received antimicrobial therapeutics such as third/fourth generation cephalosporins or carbapenem intraoperatively were also excluded. Those without preoperative infections were eligible for inclusion in this study. Patients were categorized into two groups based on the duration of antimicrobial prophylaxis: intraoperative or up to 24 h after surgery and more than 24 h after surgery. When postoperative infection occurred clinically and the patient was switched from antimicrobial prophylaxis to antimicrobial therapeutics, the duration of antimicrobial therapy was not included. The primary endpoint of this study was the incidence of surgical site infection within 30 days of surgery. The secondary endpoints were the incidence of remote infection, clinically relevant postoperative pancreatic fistula (CR‐POPF), postoperative complications other than infectious complications, length of postoperative hospital stay, readmission, and 90‐day mortality. This study was approved by the Institutional Review Board of Hiroshima University and was conducted in accordance with the principles of the Declaration of Helsinki (approval number: E‐2022‐0227).
Postoperative infection
2.2
Postoperative infections included surgical site and remote infections. Surgical site infections were categorized as superficial, deep incisional, or organ/space infections. Remote infections were classified as respiratory tract infection, antibiotic‐associated diarrhea, urinary tract infection, catheter‐related bloodstream infection, drain infection, or bacteremia of unknown origin, in accordance with the National Healthcare Safety Network infection criteria.14 The presence of POPF was determined according to the International Study Group of Pancreatic Fistula criteria.15 A single closed drain was routinely placed near the pancreatic stump remnant. Grade B and C POPF were defined as CR‐POPF and classified into infectious and non‐infectious CR‐POPF. The incidence of postoperative infection was monitored for 30 days postoperatively, and the severity was graded according to the Clavien–Dindo classification system.16 Grades III, IV, and V were defined as severe. Readmission was defined as admission within 30 days of discharge from the initial surgery. Mortality was defined as surgery‐related death occurring within 90 days of surgery.
Data collection
2.3
Patient characteristics, including age, sex, body mass index (BMI), American Society of Anesthesiologists physical status classification (ASA‐PS), combined cardiovascular and pulmonary disease, diabetes, laparotomy, smoking, steroid use, prognostic nutritional index (PNI), pancreatic disease, and whether or not neoadjuvant therapy was administered, were collected. Surgical data included antimicrobial prophylaxis duration, surgical procedure, texture of pancreas, thickness and method of pancreas transection, combined vascular and organ resection, operation time, estimated blood loss, and transfusion. The postoperative outcome data included surgical site and remote infections, CR‐POPF, non‐infectious postoperative complications, postoperative hospital stay, readmission, and 90‐day mortality.
Statistical analysis
2.4
Continuous variables are presented as median and interquartile range (IQR). Categorical variables were compared using the chi‐squared test or Fisher's exact test, while continuous variables were compared using the Mann–Whitney U test. Propensity score matching (PSM) was performed to adjust for selection bias. A propensity score for each patient was estimated using a logistic regression model, with duration of antimicrobial prophylaxis as the dependent variable. Covariates included clinicopathological factors potentially associated with postoperative infections. After calculating the propensity scores, 1:1 nearest neighbor matching was applied with a caliper of 0.2. Risk factors were evaluated using univariate and multivariate logistic regression models, and odds ratios (OR) and 95% confidence intervals were reported. All tests were two‐sided, and p < 0.05 was considered significant. Statistical analyses were performed using the JMP software (version 17.0; SAS Institute, Cary, NC, USA).
RESULTS
3
Participants
3.1
This study enrolled 569 consecutive patients who underwent distal pancreatectomy at four high‐volume Japanese centers between April 2017 and March 2022. Of these patients, three who underwent contaminated surgery and 70 who received antimicrobial therapeutics such as third/fourth generation cephalosporins or carbapenem intraoperatively were excluded. The remaining 496 patients were eligible for this study. The enrolled patients were divided into the intraoperative or up to 24‐h administration of antimicrobial prophylaxis (n = 254) and more than 24‐h groups (n = 242), respectively. The intraoperative or up to 24‐h group included those who received antimicrobial prophylaxis intraoperatively (n = 21) and up to 24 h after surgery (n = 233). The more than 24‐h group included those who received antimicrobial prophylaxis for up to 48 h after surgery (n = 156), up to 72 h after surgery (n = 81), and more than 72 h after surgery (n = 5). The patient flow diagram is summarized in Figure 1.
Patient flow diagram of this study.
Surgical site infections occurred in 129 patients (26%), including 15 superficial incisional surgical site infections (3%), four deep incisional surgical site infections (1%), and 113 organ/space surgical site infections (23%). CR‐POPF occurred in 80 patients (16%), including 61 infectious POPF (12%) and 19 non‐infectious POPF (4%). Severe surgical site infections were observed in 44 patients (9%). Remote infections occurred in 10 patients (2%), including five cases of respiratory tract infections, two urinary tract infections, one antibiotic‐associated diarrhea, and others. Severe remote infections were observed in three patients (1%). Antimicrobial therapy was administered to 127 patients (26%) with postoperative infections. Non‐infectious postoperative complications occurred in 91 patients (18%). The median postoperative hospital stay was 14 days (IQR, 10–22 years). Readmission was required for 25 patients (5%), and 90‐day mortality occurred in one patient (0.2%).
Comparisons between the intraoperative or up to 24‐h and more than 24‐h groups
3.2
Comparisons of patient demographics and postoperative outcomes between the two groups are summarized in Table 1. In terms of baseline characteristics, the intraoperative or up to 24‐h group had a significantly lower incidence of ASA‐PS ≥3, cardiovascular diseases, pulmonary diseases, and smoking, whereas they had a significantly higher rate of malignant tumors. Other characteristics, including age, sex, BMI, diabetes, laparotomy, steroid use, PNI and neoadjuvant therapy, were not significantly different between the two groups. With regards to surgical factors, the intraoperative or up to 24‐h group had a significantly lower incidence of soft pancreas, stapler transection, and longer operation time. Other surgical factors, including procedures, thickness of pancreas transection, combined vascular and organ resection, estimated blood loss and transfusion, were not significantly different between the two groups.
With respect to postoperative outcomes, the intraoperative or up to 24‐h group had a significantly lower incidence of surgical site infections (not superficial incisional and deep incisional but organ/space infections, 17% vs. 29%, p = 0.001), infectious CR‐POPF (8% vs. 17%, p = 0.002), and prolonged postoperative hospital stay (13 vs. 17 days, p < 0.001). Severe surgical site infections were not significantly different between the two groups (p = 0.643). Other surgical outcomes, including remote infection, non‐infectious postoperative complications, non‐infectious CR‐POPF, readmission, and 90‐day mortality, were not significantly different between the two groups.
After PSM using the following nine variables — ASA‐PS, cardiovascular disease, pulmonary disease, smoking status, pancreatic disease, type of procedure, texture of the pancreas, method of pancreatic transection, and operation time — 181 patients were assigned to each group (Table 2). Patient characteristics were almost similar between the two groups. In terms of postoperative outcomes, the intraoperative or up to 24‐h group had a significantly lower incidence of surgical site infections (including superficial incisional and organ/space infections) at 19% compared with 33% in the more than 24‐h group (p = 0.003), as well as a lower rate of infectious CR‐POPF (8% vs. 17%, p = 0.006) and prolonged postoperative hospital stay (13 vs. 16 days, p < 0.001).
Risk factors of postoperative surgical site infection
3.3
Univariate and multivariate analyses of the risk factors for postoperative surgical site infections are summarized in Table 3. Univariate analysis showed that antimicrobial prophylaxis, thickness and method of pancreas transection, and operation time were significantly associated with surgical site infection. Multivariate logistic regression revealed that more than 24‐h administration of antimicrobial prophylaxis (OR = 2.04; p = 0.001), thicker pancreas transection (OR = 1.65; p = 0.023), non‐stapler transection of pancreas (OR = 2.13; p = 0.022), and longer operation time (OR = 1.92; p = 0.003) were independent risk factors for postoperative surgical site infections.
DISCUSSION
4
Antimicrobial prophylaxis is useful for the prevention of postoperative infections following gastrointestinal surgery. Its short‐term use is generally recommended,1, 2 as it minimizes the development of bacterial resistance, reduces the risk of antibiotic‐related complications, and is cheaper than prolonged regimens. However, specific evidence regarding the optimal duration of antimicrobial prophylaxis for each gastrointestinal surgical procedure remains controversial,3, 4, 5, 6 especially in pancreatic surgery.
Pancreatic surgery is a highly specific and difficult procedure, and postoperative complications including infectious diseases can occur even in high‐volume centers.17, 18, 19 Postoperative infections after pancreatic surgery primarily include surgical site infections (POPF, abdominal abscess, and anastomotic leakage) and remote infections (respiratory tract infections, antibiotic‐associated diarrhea, and urinary tract infections). Pancreatoduodenectomy includes pancreatojejunostomy/gastrostomy, hepaticojejunostomy, and gastro/duodenojejunostomy, and can cause POPF, bile leakage, anastomotic leakage, and various other infectious complications associated with gastrointestinal reconstruction. In addition, periampullary diseases with bile stenosis or obstructive jaundice require preoperative biliary drainage, and bile contamination is a risk factor for postoperative infection after pancreatoduodenectomy.11 Furthermore, the use of perioperative antibiotics covering bile contamination is valid for preventing postoperative infection. Antimicrobial prophylaxis and therapeutics may not be appropriate in most preoperative biliary drainage cases. In contrast, distal surgery does not require preoperative biliary drainage or intraoperative gastrointestinal anastomosis, and antimicrobial prophylaxis is relatively easy. In the current study, cephalosporins were used as antimicrobial prophylaxis for the eligible patients. Postoperative infection occurred in 28% of the eligible patients, including surgical site infection (26%) and remote infection (2%). Most surgical site infections were organ/space infections and almost half were infectious CR‐POPF. Nationwide surveys reported that postoperative infections after pancreatic surgery occurred in 15–31%20, 21, 22, 23 of patients, and our study results from four high‐volume centers were considered valid and reliable for the analysis of relationships between antimicrobial prophylaxis and postoperative infection after distal pancreatectomy. To the best of our knowledge, this is the first multicenter cohort study to report on the association between the duration of antimicrobial prophylaxis and postoperative infections after distal pancreatectomy. Moreover, the present study comprised a multi‐institutional cohort of patients who underwent surgery during the most recent 5‐year period, minimizing the bias of changes in usual practices, such as surgical procedures or treatment indications for postoperative infection.
Patients in this study were classified into two groups based on the duration of antimicrobial prophylaxis: intraoperative or up to 24‐h and more than 24‐h administration groups. Between the two groups, the more than 24‐h group had significantly worse performance status, cardiovascular and pulmonary disease, smoking, borderline tumors, soft pancreas, non‐stapler transection, and longer operation time. Some of them were previously reported as risk factors of postoperative infections.24, 25 These may represent an important bias in patient demographics in this retrospective study. With respect to postoperative outcomes, organ/space surgical site infections, mostly infectious CR‐POPF, occurred more frequently in the more than 24‐h group, whereas the frequencies of severe infections, remote infections, non‐infectious postoperative complications, readmission, and mortality were similar. These results were consistent in the PSM analysis and indicate that longer antimicrobial prophylaxis is highly associated with non‐severe infections. Clinically, whether longer antimicrobial prophylaxis causes infectious CR‐POPF or whether longer antimicrobial prophylaxis should be administered to high‐risk CR‐POPF patients remains controversial. However, multivariate logistic regression models revealed that more than 24‐h administration of antimicrobial prophylaxis was an independent risk factor for surgical site infections, as well as thicker pancreas transection, non‐stapler transection, and longer operation duration.
POPF is the most common postoperative complication following distal pancreatectomy. The definition and grading of POPF were developed and updated by an international study group.8 The risk factors for CR‐POPF include the following: small duct, soft pancreas, high‐risk pathology, and excessive blood loss.26 Longer antimicrobial prophylaxis was not included in the factors influencing fistula risk score. If prolonged antimicrobial prophylaxis causes infectious CR‐POPF, the underlying pathophysiological mechanism may involve antimicrobial resistance or microbial substitution. This longer administration could activate trypsin, elastase, and other pancreatic exocrine enzymes, leading to the development of infectious CR‐POPF, despite patients typically receiving supportive therapies, such as perioperative pancreatic enzymes, protectants, or early diets, to prevent these problems. In addition, prolonged antimicrobial prophylaxis may lead to occult bacterial translocation,27 a mild bacteremia not detected by conventional culture methods that can cause postoperative infections. In other surgical fields, prolonged prophylaxis with antimicrobials has also been associated with an increased risk of acquired antimicrobial resistance.28 Moreover, Krezalek et al.29 demonstrated that immune cells, such as those in Trojan horses, carrying gut‐derived antimicrobial‐resistant bacteria might be a plausible mechanism behind surgical site infections in the absence of direct contamination. Based on this theory, prolonged antimicrobial prophylaxis may be associated with postoperative infections.
This study has several limitations. First, patient selection, antimicrobial prophylaxis durations and protocols, surgical techniques, and approaches to postoperative infections may have varied among the centers, although PSM was conducted to minimize bias. However, four high‐volume centers in Japan were included in the study, all of which followed standard perioperative assessments in compliance with established guidelines. Second, it remains clinically unclear whether longer antimicrobial prophylaxis causes surgical site infections, or whether longer antimicrobial prophylaxis is administered to high‐risk surgical site infection patients. To overcome these limitations, further prospective randomized controlled trials with a larger number of institutions are warranted. In conclusion, prolonged administration of antimicrobial prophylaxis may not be effective in preventing surgical site infections after distal pancreatectomy compared to intraoperative or up to 24‐h administration.
AUTHOR CONTRIBUTIONS
Kenjiro Okada: Conceptualization; data curation; formal analysis; investigation; methodology; project administration; writing – original draft; writing – review and editing. Kenichiro Uemura: Conceptualization; formal analysis; investigation; methodology; project administration; supervision; writing – review and editing. Sohei Satoi: Conceptualization; writing – review and editing. Tsutomu Fujii: Conceptualization; writing – review and editing. Manabu Kawai: Conceptualization; writing – review and editing. So Yamaki: Data curation; writing – review and editing. Toru Watanabe: Data curation; writing – review and editing. Hideki Motobayashi: Data curation; writing – review and editing. Shinya Takahashi: Conceptualization; formal analysis; investigation; methodology; project administration; supervision; writing – review and editing.
FUNDING INFORMATION
The authors received no financial support for the research, authorship, and/or publication of this article.
CONFLICT OF INTEREST STATEMENT
Author Tsutomu Fujii is an editorial board member of Annals of Gastroenterological Surgery.
ETHICS STATEMENT
Approval of the research protocol by an Institutional Reviewer Board: The protocol for this research project has been approved by the Institutional Review Board of Hiroshima University, and it conforms to the provisions of the Declaration of Helsinki.
Informed Consent: N/A.
Registry and the Registration No. of the study/trial: Institutional Review Board of Hiroshima University, Approval No. E‐2022‐0227.
Animal Studies: N/A.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Leaper DJ , Edmiston CE . World Health Organization: global guidelines for the prevention of surgical site infection. J Hosp Infect. 2017;95:135–136.28139389 10.1016/j.jhin.2016.12.016 · doi ↗ · pubmed ↗
- 2Bratzler DW , Dellinger EP , Olsen KM , Perl TM , Auwaerter PG , Bolon MK , et al. Clinical practice guidelines for antimicrobial prophylaxis in surgery. Am J Health Syst Pharm. 2013;70:195–283.23327981 10.2146/ajhp 120568 · doi ↗ · pubmed ↗
- 3Mohri Y , Tonouchi H , Kobayashi M , Nakai K , Kusunoki M , Mie Surgical Infection Research G . Randomized clinical trial of single‐ versus multiple‐dose antimicrobial prophylaxis in gastric cancer surgery. Br J Surg. 2007;94:683–688.17514671 10.1002/bjs.5837 · doi ↗ · pubmed ↗
- 4Imamura H , Kurokawa Y , Tsujinaka T , Inoue K , Kimura Y , Iijima S , et al. Intraoperative versus extended antimicrobial prophylaxis after gastric cancer surgery: a phase 3, open‐label, randomised controlled, non‐inferiority trial. Lancet Infect Dis. 2012;12:381–387.22297080 10.1016/S 1473-3099(11)70370-X · doi ↗ · pubmed ↗
- 5Takagane A , Mohri Y , Konishi T , Fukushima R , Noie T , Sueyoshi S , et al. Randomized clinical trial of 24 versus 72 h antimicrobial prophylaxis in patients undergoing open total gastrectomy for gastric cancer. Br J Surg. 2017;104:e 158–e 164.28121044 10.1002/bjs.10439 · doi ↗ · pubmed ↗
- 6Suzuki T , Sadahiro S , Maeda Y , Tanaka A , Okada K , Kamijo A . Optimal duration of prophylactic antibiotic administration for elective colon cancer surgery: a randomized, clinical trial. Surgery. 2011;149:171–178.20655559 10.1016/j.surg.2010.06.007 · doi ↗ · pubmed ↗
- 7Ohge H , Mayumi T , Haji S , Kitagawa Y , Kobayashi M , Kobayashi M , et al. The Japan Society for Surgical Infection: guidelines for the prevention, detection, and management of gastroenterological surgical site infection, 2018. Surg Today. 2021;51:1–31.33320283 10.1007/s 00595-020-02181-6PMC 7788056 · doi ↗ · pubmed ↗
- 8Bassi C , Marchegiani G , Dervenis C , Sarr M , Abu Hilal M , Adham M , et al. The 2016 update of the international study group (ISGPS) definition and grading of postoperative pancreatic fistula: 11 years after. Surgery. 2017;161:584–591.28040257 10.1016/j.surg.2016.11.014 · doi ↗ · pubmed ↗