Comparison of in vitro antimicrobial susceptibility between mucoid and non-mucoid Pseudomonas aeruginosa and its guiding value for antibiotic therapy
Yun Wu, Aixin Wang, Jinghan Qu, Ruirui Ma, Wei Kang, Yali Liu, Yingchun Xu

TL;DR
This study compares antibiotic susceptibility in mucoid and non-mucoid Pseudomonas aeruginosa to guide better treatment choices.
Contribution
The study provides large-scale evidence on the differing antimicrobial susceptibility and treatment outcomes between mucoid and non-mucoid P. aeruginosa.
Findings
Mucoid P. aeruginosa showed lower resistance to most antibiotics compared to non-mucoid strains.
In vitro susceptibility tests aligned well with treatment outcomes for both mucoid and non-mucoid infections.
Mucoid infections were more common in females and primarily from respiratory tract specimens.
Abstract
The aim of the study was to compare in vitro antimicrobial susceptibility between mucoid and non-mucoid Pseudomonas aeruginosa and its guiding value for antibiotic therapy. A retrospective review was conducted on the sources of isolates, patient information, in vitro antimicrobial susceptibility results, and antimicrobial usage records for mucoid and non-mucoid P. aeruginosa isolates spanning from 2021 to 2023, comparing the differences between the two types. Additionally, infection cases of mucoid and non-mucoid P. aeruginosa were selected for in-depth analysis of their treatment courses, evaluating the guiding value of antimicrobial susceptibility results for antimicrobial therapy. We collected 1,443 non-mucoid P. aeruginosa and 342 mucoid P. aeruginosa. Our findings revealed that mucoid P. aeruginosa was predominantly found in respiratory tract specimens, while non-mucoid P.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
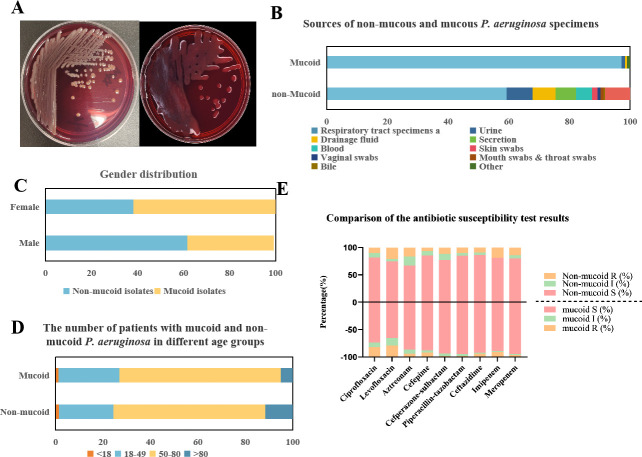 Fig 1
Fig 1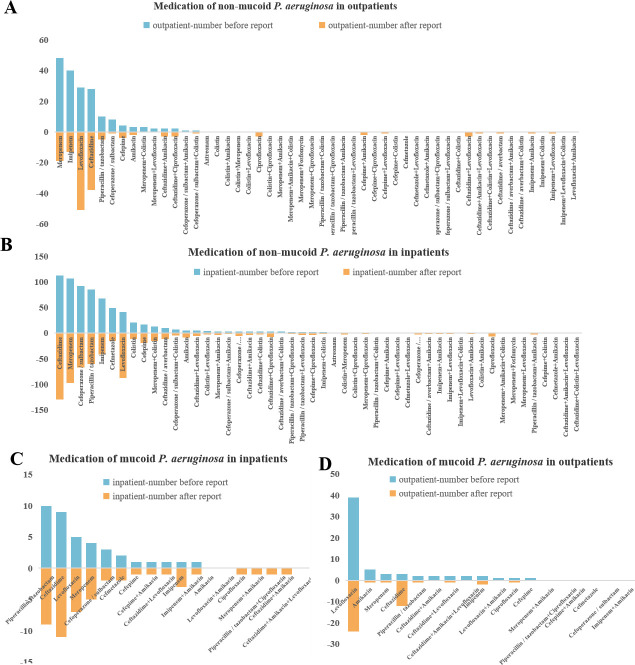 Fig 2
Fig 2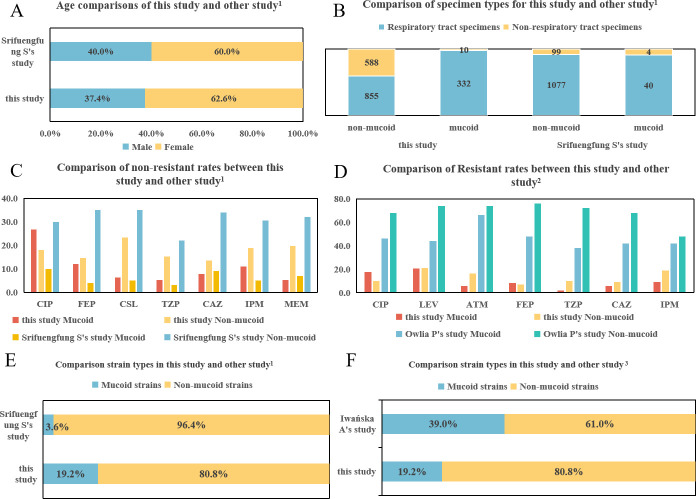 Fig 3
Fig 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBacterial biofilms and quorum sensing · Antibiotic Resistance in Bacteria · Oral microbiology and periodontitis research
INTRODUCTION
Pseudomonas aeruginosa is an opportunistic pathogen, posing serious infection risks to patients undergoing mechanical ventilation, individuals who are immunocompromised, and those with malignancies or HIV infection. Hospital-acquired infections are common, and chronic airway infections with P. aeruginosa are a significant co-morbidity in patients with cystic fibrosis (CF), bronchiectasis, chronic obstructive pulmonary disease (COPD), or ventilator-associated pneumonia (VAP) (1–3).
P. aeruginosa can be classified into mucoid and non-mucoid types based on colony morphology. Mucoid P. aeruginosa displays a slower growth rate, forming smaller colonies when cultured at 35°C for 24 hours, which can lead to their easy oversight (4). Previous studies have confirmed differences in antimicrobial susceptibility (3, 5), as well as in treatment and prognosis (6), between mucoid and non-mucoid P. aeruginosa. Considering the difficulty in performing in vitro antimicrobial susceptibility testing for P. aeruginosa (7), especially for mucoid isolates, it is uncertain whether in vitro susceptibility to antimicrobial agents can accurately guide the selection of antimicrobial agents. Foreign studies indicated that mucoid P. aeruginosa is predominantly isolated from cystic fibrosis patients (8–10); however, cystic fibrosis patients are rare in China. The main diseases caused by mucoid P. aeruginosa in China are still unclear. Additionally, some research has highlighted differences in disease progression and outcomes between mucoid and non-mucoid P. aeruginosa infections (11). Therefore, it’s essential to conduct a comparative study between mucoid and non-mucoid P. aeruginosa, focusing on demographic and clinical characteristics, in vitro antimicrobial susceptibility, as well as the selection of antimicrobial agents. Moreover, it’s vital to evaluate the guiding value of in vitro antimicrobial susceptibility testing for antimicrobial therapy.
This study examined the specimen sources, gender distribution, age groups, clinical diagnosis, and antimicrobial susceptibility of 1,443 non-mucoid P. aeruginosa and 342 mucoid P. aeruginosa isolated from a tertiary hospital in China, Peking Union Medical College Hospital, between 2021 and 2023. We also analyzed the usage of antimicrobial agents among mucoid and non-mucoid P. aeruginosa, comparing differences between outpatients and inpatients, as well as before versus after antimicrobial susceptibility reports. Additionally, we also evaluated the consistency between the results of antimicrobial susceptibility in vitro and the treatment outcome. The primary aim of this analysis was to provide robust insights for the clinical prevention and treatment of P. aeruginosa infections.
MATERIALS AND METHODS
P. aeruginosa isolates and clinical data collection
This study focused on 1,443 non-mucoid P. aeruginosa and 342 mucoid P. aeruginosa, isolated from a diverse range of clinically submitted and qualified specimens at Peking Union Medical College Hospital between 2021 and 2023. Only the first isolate from the same site in the same patient was included. To analyze the differences in the usage of antimicrobial agents between mucoid and non-mucoid P. aeruginosa infection, we retrieved medication usage data from the Hospital Information System for the treatment of P. aeruginosa. Clinical information, including patient’s gender, age, isolated department, and infection site, was also obtained from the Hospital Information System.
Bacterial identification and Antimicrobial Susceptibility Test
All isolates were positive in the oxidase test and identified as P. aeruginosa through matrix-assisted laser desorption/ionization time-of-flight (MALDI-TOF) mass spectrometry (Smart MS, Zhuhai DL Biotech Co., Ltd). Antimicrobial susceptibility test (AST) of mucoid P. aeruginosa was performed using the disk diffusion method. For non-mucoid P. aeruginosa, AST was carried out using VITEK2 N335 (gram-negative bacteria susceptibility test card; BioMérieux) and the disk diffusion method. Interpretation of the AST results was based on the clinical breakpoints of M100-Ed34 of the Clinical and Laboratory Standards Institute (CLSI) 2024 (12). Escherichia coli (ATCC 25922) and P. aeruginosa (ATCC 27853) were used as quality controls.
Correlation of in vitro antimicrobial susceptibility and clinical outcome
Among the 1,143 non-mucoid P. aeruginosa and 342 mucoid P. aeruginosa with antimicrobial susceptibility data, 56 non-mucoid isolates and 57 mucoid isolates, which were isolated from hospitalized patients with a confirmed diagnosis of monomicrobial P. aeruginosa infection, were selected for case information retrieval. Cases with incomplete information or those without antibiotic treatment were excluded. Ultimately, 42 non-mucoid P. aeruginosa cases and 36 mucoid P. aeruginosa cases were involved in our study. Concordance between in vitro antimicrobial susceptibility testing and clinical outcomes was considered if the antimicrobial agents used in the treatment were susceptible in vitro and the treatment outcome was either cured or improved, or if the antimicrobial agents were resistant in vitro and the outcome was either not cured or resulted in death. Any other discrepancies were classified as discordant. Detailed sample data are shown in Fig. S1.
Statistical approach
All statistical analyses were performed using Statistical Package for the Social Sciences version 29.0 software (SPSS Inc., Chicago, IL, USA). Descriptive analysis was conducted, and differences in specimen sources, gender distribution, age groups, clinical distribution, and antibiotic resistance rate between mucoid and non-mucoid isolates were assessed using Pearson’s χ^2^ test or correction for continuity. A P value of < 0.05 was considered statistically significant.
RESULTS
Isolates and patients information
We collected 1,443 non-mucoid and 342 mucoid P. aeruginosa. The sources of the specimens for both mucoid and non-mucoid P. aeruginosa are illustrated in Fig. 1B. Mucoid P. aeruginosa isolates were predominantly isolated from respiratory specimens, accounting for 97% of the total. In contrast, non-mucoid P. aeruginosa isolates isolated from respiratory specimens comprised 45% of the total (P < 0.001), with 8.5% originating from urine and 7.5% from drainage fluid.
Clinical information of the collected isolates. (A) Comparison of mucoid and non-mucoid P. aeruginosa colonies (cultured at 35°C for 24 hours on CBA). Left: the colony morphology of non-mucoid P. aeruginosa. Right: the colony morphology of mucoid P. aeruginosa. (B) Gender distribution of P. aeruginosa mucoid and non-mucoid type. (C) The number of patients with mucoid and non-mucoid P. aeruginosa in different age groups. (D) Sources of non-mucoid and mucoid P. aeruginosa specimens. Respiratory tract specimens include sputum, tracheobronchial aspirate, endotracheal aspirate, and bronchoalveolar lavage fluid. (E) Comparison of the antimicrobial susceptibility test results for non-mucoid and mucoid P. aeruginosa to different antibiotics. Left: Mucoid isolates; Right: Non-mucoid isolates.
Notably, a statistically significant gender disparity was observed (P < 0.001), with mucoid P. aeruginosa isolates being predominantly associated with female patients (62.6%, 214/342), while non-mucoid isolates were predominantly found in male patients (61.7%, 890/1,443). The distribution of patients with mucoid and non-mucoid P. aeruginosa across different age groups is shown in Fig. 1D. A statistically significant difference was observed in the percentage of isolates for individuals above 80 years (P < 0.001).
Comparison of antimicrobial susceptibility results
Figure 1E presented a comparison of antimicrobial susceptibility results for non-mucoid and mucoid P. aeruginosa across nine commonly used antimicrobial agents. Among the nine different antimicrobial agents, it was evident that mucoid P. aeruginosa generally exhibited notably lower resistance levels in comparison to non-mucoid isolates (P < 0.001), except for ciprofloxacin and cefepime. Specifically, mucoid P. aeruginosa exhibited significantly higher resistance to ciprofloxacin compared to non-mucoid isolates (P < 0.001). The lowest resistance rate observed among mucoid isolates was piperacillin-tazobactam (1.7%), while non-mucoid isolates exhibited the lowest resistance rate to cefepime (6.8%). Both mucoid and non-mucoid P. aeruginosa isolates demonstrated the highest resistance rates against levofloxacin, exceeding 20%.
Selection of antimicrobial agents in mucoid and non-mucoid P. aeruginosa
Figure 2 shows the medication use profiles of mucoid and non-mucoid P. aeruginosa in both outpatient and inpatient departments. A notable difference between the two groups was observed in the medication use. There are seven kinds of monotherapy and nine kinds of combined therapy for mucoid P. aeruginosa, while for non-mucoid P. aeruginosa, there are eight kinds of monotherapy and 39 kinds of combined therapy. We observed specific antimicrobial agent preferences in the treatment of mucoid and non-mucoid P. aeruginosa. In mucoid P. aeruginosa, the most frequently prescribed antimicrobial agent was levofloxacin, followed by ceftazidime and piperacillin/tazobactam. Treatment preferences differed between outpatients and inpatients with mucoid P. aeruginosa; piperacillin/tazobactam was most commonly used in hospitalized patients (Fig. 2C), whereas levofloxacin was preferred for outpatients (Fig. 2D). For non-mucoid P. aeruginosa, ceftazidime and meropenem were the most commonly prescribed antimicrobial agents overall. In hospitalized patients, ceftazidime was most frequently used (Fig. 2B), followed by meropenem, whereas levofloxacin was the more popular antimicrobial agent choice for outpatients (Fig. 2A).
Medication of mucoid and non-mucoid P. aeruginosa. A through D.
A definitive antimicrobial susceptibility report significantly influences medication decisions. Among outpatients, 9.78% (9/92) of antimicrobial agents for mucoid P. aeruginosa were adjusted following the microbiological report, compared to 11.50% (32/287) for non-mucoid P. aeruginosa (Fig. 2A, Fig. 2D). For hospitalized patients, 22.91% (11/48) of mucoid P. aeruginosa treatments and 18.10% (148/817) of non-mucoid P. aeruginosa treatments were adjusted post-report (Fig. 2B, Fig. 2C). Compared with the situation that clinicians administer drugs without knowing a definitive antimicrobial susceptibility report, after the report, there was an increase in the use frequency of ceftazidime and levofloxacin, while the use frequency of meropenem and piperacillin/tazobactam decreased in non-mucoid P. aeruginosa. The antimicrobial agents adjustment of mucoid P. aeruginosa was similar to non-mucoid P. aeruginosa, except for mucoid P. aeruginosa in outpatients, where the frequency of levofloxacin decreased. After the report, in both mucoid and non-mucoid P. aeruginosa, the usage of ciprofloxacin became more frequent.
Correlation of in vitro antimicrobial susceptibility and clinical outcome
A total of 42 non-mucoid P. aeruginosa cases and 36 mucoid P. aeruginosa cases were included with complete case information. The analysis results of case information are shown in Table S1. The most commonly used antimicrobial agents for non-mucoid P. aeruginosa were meropenem (15/42, 35.7%), followed by ceftazidime (12/42, 26.1%). For mucoid P. aeruginosa, the most commonly used antimicrobial agent was ceftazidime (12/36, 33.3%). Among non-mucoid P. aeruginosa cases, 78.6% were treated with combined therapy, while only 54.1% of mucoid P. aeruginosa cases were treated with combined therapy. Additionally, we analyzed the consistency between the antimicrobial susceptibility results and the outcomes (improvement or no cure) for the antimicrobial agents used. The results showed that 90.2% of non-mucoid P. aeruginosa infections and 94.4% of mucoid P. aeruginosa infections showed consistency between in vitro antimicrobial susceptibility and outcomes. In the case of mucoid and non-mucoid P. aeruginosa infection, there were two and three cases, respectively, where the in vitro antimicrobial susceptibility was sensitive, yet the clinical treatment outcome was either death or failure to cure. Among infections caused by non-mucoid P. aeruginosa, there were two cases where the in vitro antimicrobial agents were resistant, but the clinical outcome was improved; no such cases were observed in infections caused by mucoid P. aeruginosa.
DISCUSSION
P. aeruginosa can be categorized into mucoid and non-mucoid types based on their colony morphology, and in the infection caused by different morphotypes of P. aeruginosa, the types of diseases and prognosis vary (6). Previous studies have confirmed that there are differences in the specimen sources, affected populations, and in vitro antimicrobial susceptibility between mucoid and non-mucoid P. aeruginosa. In this study, we observed similar results that the rate of mucoid P. aeruginosa isolates among female patients (62.6%) exceeded that among male patients (37.4%). Conversely, non-mucoid P. aeruginosa was primarily isolated from male patients (61.7%). Regarding age distribution, it is notable that middle-aged women with chronic respiratory diseases appear particularly susceptible to mucoid P. aeruginosa infections. We also compared our results with the international research, which is a representative and comparative analysis of the demographic information of mucoid P. aeruginosa (3, 5, 13). The data from these international studies show a strong consistency with the results of this study. Both domestic and international studies indicate a predominance of female isolates in the gender composition (Fig. 3A). In terms of specimen types, the majority are derived from respiratory tract samples (Fig. 3B). Regarding the susceptibility of mucoid and non-mucoid isolates to main antimicrobial agents, while there is variability in resistance levels among isolates from different regions, the differences in resistance levels between mucoid and non-mucoid isolates are consistent, with these differences being more pronounced in Srifuengfung S’ and Owlia P’s studies. For instance, as illustrated in Fig. 3C (3) and Fig. 3D (5), the international data demonstrates that the resistance rates of non-mucoid P. aeruginosa are higher than those of mucoid isolates across all tested antimicrobial agents.
*Comparison of home and foreign data. Reference in this figure. (3, 5, 14). A through F.
Fluoroquinolone, especially ciprofloxacin, plays a crucial role in the treatment of P. aeruginosa infections (15). However, our study demonstrates that fluoroquinolone might not be as effective in treating infections caused by mucoid P. aeruginosa as they are in treating non-mucoid isolates. Both types of P. aeruginosa exhibited the highest resistance rates to levofloxacin among the nine frequently used antimicrobial agents. When analyzing the therapy of P. aeruginosa infections, we found that the use frequency of levofloxacin for both phenotypes of P. aeruginosa was the highest among outpatients, which may contribute to the high rate of levofloxacin resistance. Ciprofloxacin was more susceptible than levofloxacin against mucoid and non-mucoid P. aeruginosa, which may explain the increased use of ciprofloxacin as a single agent or in combination after being reported. Ciprofloxacin was widely used in hospitalized patients with non-mucoid P. aeruginosa infections, either alone or in combination with other antimicrobial agents such as ceftazidime, meropenem, piperacillin/tazobactam, and colistin. However, its use in mucoid P. aeruginosa infections is limited. Piperacillin-tazobactam was the most effective antibiotic with a sensitivity rate of 89.7%, making it one of the cornerstone antimicrobial agents for treating P. aeruginosa infections (14). Several studies have found that macrolide antibiotics have the capability to inhibit the formation of biofilms and adhesion in mucoid P. aeruginosa. While they may not possess direct anti-P. aeruginosa activity, when used in conjunction with antibacterial agents that do have anti-P. aeruginosa activity, they can enhance the overall effectiveness of treatment (16–18).
The in vitro antimicrobial susceptibility testing of mucoid P. aeruginosa is challenging due to its slow growth rate. Therefore, the accuracy of such testing and its clinical guidance value for antimicrobial therapy remain unclear. This study evaluated the use of antimicrobial agents for the treatment of two different phenotypes of P. aeruginosa from two perspectives: first, a comprehensive analysis and comparison of all antimicrobial agents used based on the data from the pharmacy; second, considering that not all isolates may be true pathogens and the possibility of polymicrobial infections, we selected cases from hospitalized patients in which P. aeruginosa was the sole pathogen and reviewed the use of antimicrobial agents, treatment outcomes, and other relevant factors. The results revealed that no matter whether in mucoid or non-mucoid P. aeruginosa, the in vitro antimicrobial susceptibility test results were in good agreement with the therapeutic outcomes. Although mucoid P. aeruginosa is more likely to form biofilms, selecting appropriate antimicrobial agents based on in vitro susceptibility results still yields good therapeutic outcomes. In mucoid P. aeruginosa, the most frequently prescribed antimicrobial agents were levofloxacin and ceftazidime, while for non-mucoid P. aeruginosa, ceftazidime and meropenem were the most commonly prescribed. In vitro antimicrobial susceptibility results of P. aeruginosa are significant for the guidance of clinical antimicrobial agent selection, so it’s vital to consistently supervise the results.
We compared the medication use data from the pharmacy department and retrospectively reviewed cases. The case selection criteria included hospitalized individuals with clear infection indications and P. aeruginosa identified as the sole pathogen. This approach aimed to exclude the potential influence of mixed infections or colonization on the medication use data from the pharmacy department. The case results were generally consistent with the pharmacy department’s data, with minor discrepancies observed. Specifically, the data from the pharmacy department indicated that the most commonly used antimicrobial agents for mucoid P. aeruginosa patients were piperacillin-tazobactam, followed by ceftazidime. However, in the case review, ceftazidime was the most frequently used antimicrobial agent. This discrepancy may be attributed to the limited amount of case information available, leading to potential bias. Through the retrospective analysis of cases, our findings are not consistent with previous studies, which indicated contradictions between laboratory testing and clinical treatment outcomes (19).
This study represents a large-scale, single-center comparative research conducted over two years at a tertiary hospital in China. We found significant differences between mucoid and non-mucoid P. aeruginosa infections in terms of gender, antimicrobial susceptibility test, and the selection of antimicrobial agents. Specifically, mucoid P. aeruginosa infections were predominantly observed in females and were mainly associated with respiratory tract infections. Moreover, the isolates with mucoid phenotype exhibited higher susceptibility to most antimicrobial agents compared to non-mucoid isolates. However, antimicrobial susceptibility testing results effectively guided the selection of appropriate antimicrobial agents, leading to improved disease prognosis. Significantly distinct differences were observed in all these aspects, which have not been previously reported in existing research. We believe these findings will contribute to a comprehensive clinical understanding of the differences between mucoid and non-mucoid P. aeruginosa, guiding rational clinical management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rowe WJ 3rd, Lebman DA, Ohman DE. 2023. Mechanism of resistance to phagocytosis and pulmonary persistence in mucoid Pseudomonas aeruginosa. Front Cell Infect Microbiol 13:1125901. doi:10.3389/fcimb.2023.112590137009499 PMC 10050686 · doi ↗ · pubmed ↗
- 2Sainz-Mejías M, Jurado-Martín I, Mc Clean S. 2020. Understanding Pseudomonas aeruginosa-host interactions: the ongoing quest for an efficacious vaccine. Cells 9:12. doi:10.3390/cells 9122617 PMC 776214133291484 · doi ↗ · pubmed ↗
- 3Srifuengfung S, Tiensasitorn C, Yungyuen T, Dhiraputra C. 2004. Prevalence and antimicrobial susceptibility of Pseudomonas aeruginosa mucoid and non-mucoid type. Southeast Asian J Trop Med Public Health 35:893–896.15916087 · pubmed ↗
- 4Meitert E, Sima F, Savulian C, Chersulick E, Sălăgeanu A. 1989. Comparative study of the biological characteristics of mucoid and non-mucoid Pseudomonas aeruginosa strains isolated from chronic respiratory infections. Arch Roum Pathol Exp Microbiol 48:193–207.2519631 · pubmed ↗
- 5Owlia P, Nosrati R, Alaghehbandan R, Lari AR. 2014. Antimicrobial susceptibility differences among mucoid and non-mucoid Pseudomonas aeruginosa isolates. GMS Hyg Infect Control 9:Doc 13. doi:10.3205/dgkh 00023325152858 PMC 4141634 · doi ↗ · pubmed ↗
- 6Reynolds D, Kollef M. 2021. The epidemiology and pathogenesis and treatment of Pseudomonas aeruginosa infections: an update. Drugs (Abingdon Engl) 81:2117–2131. doi:10.1007/s 40265-021-01635-6PMC 857214534743315 · doi ↗ · pubmed ↗
- 7Kai Lan WZ. 2012. Accuracy evaluation of different antibiotic susceptibility testing for mucoid isolates of Pseudomonas aeruginosa. Lab Med 27:544–548.
- 8Moore JE, Mastoridis P. 2017. Clinical implications of Pseudomonas aeruginosa location in the lungs of patients with cystic fibrosis. J Clin Pharm Ther 42:259–267. doi:10.1111/jcpt.1252128374433 · doi ↗ · pubmed ↗