The effect of tadalafil 5 mg on erection and persistent storage lower urinary tract symptoms after transurethral resection of prostate: a randomized controlled study
Diaa-Eldin Taha, Hossam Nabeeh, Khaled Magdy Zeinelabden, Elsayed Abdelhalim, Salah Elmekawy, Ibrahem Ismail Samaha, Ahmed behiry, Ahmed abd Elmoaty, Tarek Abdelbaky, Ali Ibrahim

TL;DR
This study found that tadalafil 5 mg daily after prostate surgery improves erectile function and slightly reduces urinary symptoms.
Contribution
The study is the first to evaluate tadalafil's effect on persistent urinary symptoms and erectile function after TURP.
Findings
Tadalafil significantly improved erectile function scores compared to placebo at 1, 3, and 6 months post-TURP.
Tadalafil modestly reduced storage lower urinary tract symptoms compared to placebo.
Improvements in erectile function were statistically significant across all time points.
Abstract
We conducted a double-blind, randomized controlled trial to evaluate the effect of early administration of tadalafil (5 mg once daily) on persistent storage lower urinary tract symptoms (LUTS) and erectile function following transurethral resection of the prostate (TURP). All enrolled patients underwent TURP and were randomly assigned to one of two groups: Group A received tadalafil (5 mg once daily) postoperatively, while Group B received a placebo. Erectile function was assessed using the International Index of Erectile Function-5 (IIEF-5) questionnaire, and LUTS were evaluated using the International Prostate Symptom Score (IPSS). The study was conducted at a tertiary care hospital between May 2021 and October 2022. A total of 195 patients were enrolled and randomized into two groups: Group A (n = 103), which received tadalafil 5 mg once daily, and Group B (n = 92), which received a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
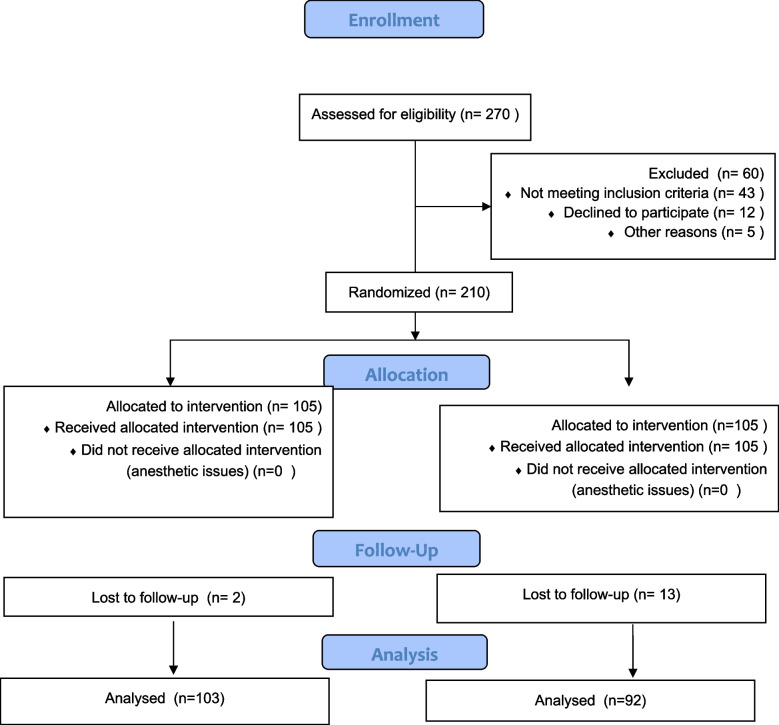 Figure 1
Figure 1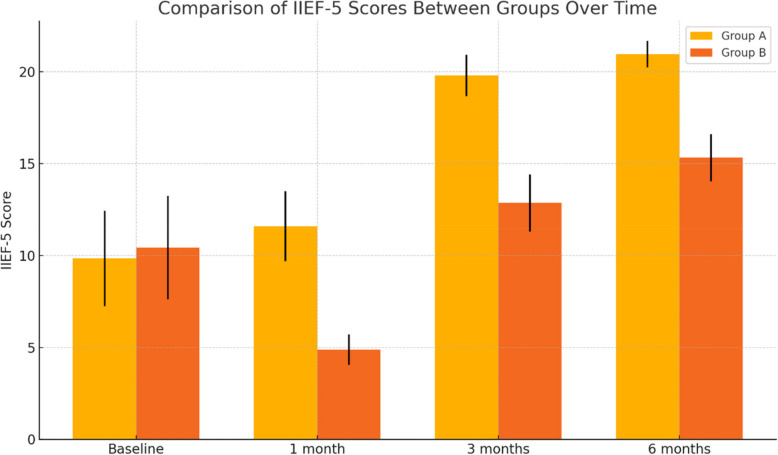 Figure 2
Figure 2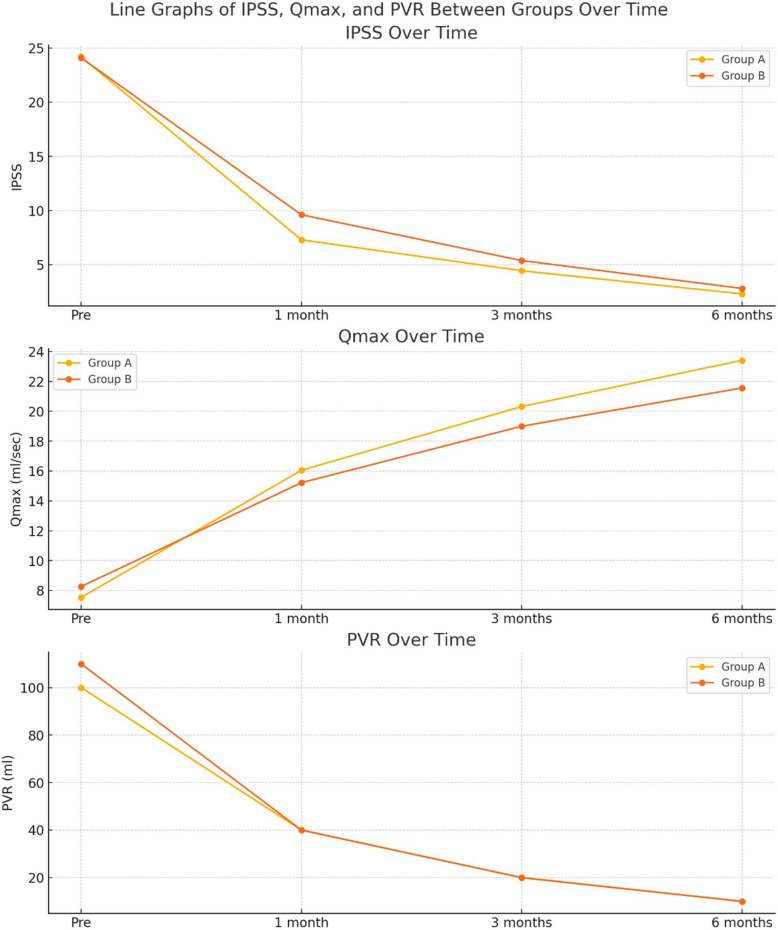 Figure 3
Figure 3- —Kafr El Shiekh University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrinary Bladder and Prostate Research · Sexual function and dysfunction studies · Pelvic floor disorders treatments
Introduction
Men with lower urinary tract symptoms (LUTS) due to benign prostatic hyperplasia (BPH) have a higher incidence of erectile dysfunction (ED) [1]. Moreover, LUTS themselves serve as an independent risk factor for ED, significantly compromising quality of life (QoL). The underlying pathophysiological mechanisms linking LUTS secondary to BPH and ED remain incompletely understood, although both conditions share several common determinants [9, 16].
Transurethral resection of the prostate (TURP) remains the gold standard for managing benign prostatic hyperplasia (BPH), despite the introduction of newer minimally invasive surgical techniques [5, 22]. However, the impact of TURP on sexual function remains uncertain. While some studies report a negative effect, others suggest an improvement in sexual function among patients with ED [19, 26].
TURP may contribute to ED through various mechanisms, primarily due to thermal injury affecting the cavernous nerves during surgery. Additional factors include the psychological impact of the procedure and the temporary cessation of sexual activity in the postoperative period [24].
Previous studies have reported that some patients experience persistent irritative symptoms following TURP, requiring postoperative medication to manage ongoing urinary symptoms. These symptoms significantly impact patients'quality of life after surgery. When selecting candidates for TURP, predicting the persistence of irritative bladder symptoms is crucial; however, studies investigating prognostic factors for bladder irritation remain limited. According to recent research, severe preoperative irritative bladder symptoms or frequent nocturia may increase the likelihood of persistent postoperative symptoms [11].
Phosphodiesterase type 5 inhibitors (PDE5-Is) were initially approved for the treatment of ED; however, they have also been shown to be highly effective in alleviating LUTS in men, regardless of the presence of ED [3, 17, 20, 23]. PDE5-Is promote relaxation of the bladder neck and prostate by increasing nitric oxide levels in smooth muscle, thereby directly influencing micturition phases in addition to their role in penile erection [6, 7]. Another study indicates that a once-daily dose of 5 mg tadalafil is a potentially effective, well-tolerated, and safe treatment option for patients with LUTS [4].
Tadalafil 5 mg once daily is currently approved for the treatment of LUTS, regardless of the presence of coexisting ED [16]. Another study reported that Tadalafil 5 mg once daily improved LUTS in men without ED by a magnitude like that observed in men with ED [2].
Once-daily tadalafil 5 mg has been shown to be most effective in enhancing drug-assisted erectile function in men with ED following radical prostatectomy. It also facilitates early recovery of erectile function post-prostatectomy and may help protect against penile structural changes. However, unassisted erectile function does not improve after discontinuation of active therapy for nine months [18].
Tadalafil monotherapy significantly improves both storage and voiding lower urinary tract symptoms (LUTS) and enhances the International Prostate Symptom Score (IPSS) [12].
To determine the potential benefits of initiating tadalafil early after TURP, we conducted this study to evaluate the efficacy of daily tadalafil 5 mg in managing persistent storage symptoms and improving erectile function post-TURP.
Materials and Methods
Following approval by the institutional ethics committee, this study was conducted at a tertiary care hospital between May 2021 and October 2022. Patients diagnosed with benign prostatic hyperplasia (BPH) who underwent transurethral resection of the prostate (TURP), either monopolar or bipolar, were eligible for inclusion. Informed consent was obtained from all participants prior to enrollment. Patients were then randomized into two groups: Group A received tadalafil 5 mg once daily, while Group B received a placebo.
All patients included in the study were sexually active prior to undergoing TURP. Patients who were sexually inactive were excluded from analyses related to sexual function, due to the recognized limitations of the International Index of Erectile Function (IIEF-5) in evaluating erectile function among sexually inactive men.
A comprehensive medical history was obtained for each participant. Evaluations included the IIEF-5 questionnaire for erectile function, the International Prostate Symptom Score (IPSS), and the IPSS storage symptom subscore-15 for assessing storage symptoms.
Additional assessments included uroflowmetry, pelvi-abdominal ultrasonography with post-void residual (PVR) urine measurement, and laboratory investigations (urinalysis, urine culture, renal function tests, complete blood count, coagulation profile, and prostate-specific antigen [PSA] level). All evaluations were conducted at baseline (pre-TURP) and at 1, 3, and 6 months postoperatively.
Randomization
Patients were randomly assigned in a 1:1 ratio into two groups using simple randomization. Group A received early administration of tadalafil 5 mg once daily starting one week after TURP, while Group B (control group) received a placebo. The randomization process was double-blinded, with both patients and surgeons blinded to group allocation. The study was conducted and will be reported in accordance with the Consolidated Standards of Reporting Trials (CONSORT) guidelines. (Fig. 1).Fig. 1. Flowchart illustrating the enrollment, randomization, allocation, follow-up, and analysis of patients in the study. Patients were assessed for eligibility, randomized into two groups (tadalafil 5 mg once daily vs. placebo) after TURP, and followed for six months. The flowchart details participant distribution, loss to follow-up, and final analysis
Sample size
The sample size was calculated a priori using power analysis (G*Power, version 3.1.9.2). The analysis was conservatively based on three primary outcomes: resolution of storage symptoms post-TURP, improvement in erectile function, and alleviation of lower urinary tract symptoms (LUTS). A Type I error rate (α) of less than 5% and a Type II error rate (β) of less than 20% were assumed. Based on these parameters, a minimum sample size of 105 patients per group was estimated to achieve 80% statistical power, accounting for an anticipated dropout rate of 20%.
Assessment
The primary outcome of the study was to evaluate the effect of early administration of tadalafil 5 mg once daily on persistent storage lower urinary tract symptoms (LUTS) and erectile function following transurethral resection of the prostate (TURP). The secondary outcome was to assess patient compliance and any adverse effects associated with tadalafil use.
Statistical analysis
Data analysis was conducted using the Statistical Package for the Social Sciences (SPSS), version 26. Categorical variables were summarized using absolute frequencies and compared using the chi-square test or Fisher’s exact test, as appropriate. Quantitative variables were expressed as means and standard deviations for normally distributed data, or as medians and interquartile ranges for non-normally distributed data. Between-group comparisons of quantitative variables were performed using the independent samples t-test for normally distributed data and the Mann–Whitney U test for non-normally distributed data. Within-group comparisons over two time points were analyzed using the paired samples t-test for normally distributed data and the Wilcoxon signed-rank test for non-normally distributed data. A p-value of < 0.05 was considered statistically significant, while a p-value of ≤ 0.001 was considered highly significant.
Results
Of the 270 patients assessed for eligibility, 195 were enrolled in the study. These patients were randomized into two groups: 103 patients (53%) were assigned to Group A, receiving tadalafil 5 mg once daily, and 92 patients (47%) to Group B, receiving a placebo. The allocation process is illustrated in the CONSORT flow diagram Fig. 1**. **
There is a statistically non-significant difference between the studied groups regarding age, BMI, medical comorbidities and prostate size Table 1. Table 1. Comparison between the studied groups regarding baseline dataGroup AGroup BtpMean ± SD^a^Mean ± SD****Age (year)63.21 ± 4.7864.08 ± 3.14−1.5130.132BMI^b^** (kg/m**^2^)24.01 ± 1.4724.38 ± 2.24−1.3240.188N = 102 (%)N = 93 (%)χ2pDiabetes mellitus14 (13.7%)22 (23.7%)3.1870.074Hypertension37 (36.3%)31 (33.3%)0.1850.667Liver disease6 (5.9%)4 (4.3%)Fisher0.854Previous surgical history68 (66.7%)63 (67.7%)0.0260.873ASA^c^1.114¥ 181 (79.4%)65 (69.9%) 215 (14.7%)22 (23.7%)0.291 35 (4.9%)6 (6.5%) 41 (1%)0 (0%)Median (IQR)Median (IQR)ZPProstate size90(66–120)90(65–119.5)−0.1840.854This analysis shows that the clinical disparities between the two groups (age, BMI, comorbidities, surgical history and ASA). X^2^ Chi square test t independent sample t test Z Mann Whitney test **p ≤ 0.001 is statistically highly significant *p < 0.05 is statistically significant ¥Chi square for trend test^a^SD Standard deviation^b^BMI Body mass index^c^ASA American society of anesthesiologists
With regard to erectile function, there was no statistically significant difference in baseline IIEF-5 scores between the two groups (p = 0.131). In Group A, a significant improvement in IIEF-5 scores was observed following TURP. The mean ± SD IIEF-5 score in Group A was 9.84 ± 2.6 at baseline, which increased to 11.59 ± 1.9, 19.8 ± 1.12, and 20.97 ± 0.72 at 1, 3, and 6 months postoperatively, respectively (P < 0.001), as shown in Fig. 2. In contrast, Group B showed a significant decline in erectile function at 1 month post-TURP, with the IIEF-5 score decreasing from a baseline of 10.43 ± 2.81 to 4.88 ± 0.82. A gradual improvement was noted at 3 and 6 months, with scores of 12.86 ± 1.56 and 15.32 ± 1.28, respectively (P < 0.001) Table 2.Fig. 2. Comparison of International Index of Erectile Function between the study groups before TURP and throughout the 6-month follow-up periodTable 2Comparison between the studied groups regarding IIEF-5 before TURP and during 6 month follow-up periodGroup AGroup BtpMean ± SDMean ± SDIIEF baseline9.84 ± 2.610.43 ± 2.81−1.5170.131IIEF 1 month11.59 ± 1.94.88 ± 0.8232.488 < 0.001IIEF 3 months**19.8 ± 1.1212.86 ± 1.5635.362 < 0.001IIEF 6 months20.97 ± 0.7215.32 ± 1.2837.483 < 0.001T independent sample t test *p < 0.05 is statistically significant **p ≤ 0.001 is statistically highly significant IIEF: International index of erectile dysfunction
Regarding overall lower urinary tract symptoms (LUTS), there was no statistically significant difference between the groups in terms of baseline International Prostate Symptom Score (IPSS), with a p-value of 0.779. Both groups demonstrated a comparable improvement in IPSS, maximum urinary flow rate (Qmax), and post-void residual urine (PVR). However, there was a statistically significant difference between the two groups regarding the storage IPSS score (p value: 0.036). as shown in Table 3. Table 3. Comparison between the studied groups regarding IPSS, Storage IPSS, Voiding IPSS, Qmax, and PVR before TURP and during 6 month follow up periodGroup AGroup BtpMean ± SDMean ± SDIPSS^a^** pre24.18 ± 2.4124.08 ± 2.630.280.779 IPSS 1 month7.31 ± 1.669.62 ± 3.34−6.027 < 0.001**** IPSS 3 months4.46 ± 0.975.4 ± 1.98−4.135 < 0.001**** IPSS 6 months2.33 ± 0.692.83 ± 1.27−3.34 < 0.001****STORAGE IPSS pre8.63 ± 1.828.03 ± 0.222.1130.036*** STORAGE IPSS 1 month3.05 ± 0.783.22 ± 0.72−1.545 < 0.001**** STORAGE IPSS 3 months1.63 ± 0.492.48 ± 0.5−12.077 < 0.001**** IPSS 6 months0.92 ± 0.671.69 ± 0.47−9.19 < 0.001****Voiding IPSS pre15.55 ± 3.07916.04 ± 3.445−1.0570.292** Voiding IPSS 1 month4.26 ± 1.9346.41 ± 3.301−5.466.000 Voiding IPSS 3 months2.83 ± 1.0352.95 ± 2.082-.472.637 Voiding IPSS 6 months1.41 ± 1.0181.18 ± 1.2591.401.163Qmax**^b^** pre7.54 ± 2.458.27 ± 2.28−3.47 < 0.001**** Qmax 1 month16.05 ± 2.0515.22 ± 2.00.638 < 0.001**** Qmax 3 months20.32 ± 3.1519.00 ± 2.10.897 < 0.001**** Qmax 6 months23.41 ± 3.3821.56 ± 3.595.892 < 0.001****Median (IQR)Median (IQR)ZPPVR^c^ pre100(90–120)110(70–160)−1.0410.298 PVR 1 month40(30–50)40(20–50)−1.0960.273 PVR 3 months20(20–30)20(15–30)−0.9560.239 PVR 6 months**10(10–20)10(10–20)−0.7720.262T independent sample t test Z Mann Whitney test *p < 0.05 is statistically significant **p ≤ 0.001 is statistically highly significant^a^IPSS International prostate system score^b^Qmax Maximum urine flow rate^c^PVR Post voiding residual
The mean (± SD) IPSS in Group A before transurethral resection of the prostate (TURP) was 24.18 ± 2.41, which improved to 7.31 ± 1.66, 4.46 ± 0.97, and 2.33 ± 0.69 at 1, 3, and 6 months post-TURP, respectively (P < 0.001). In Group B, the mean (± SD) IPSS before TURP was 24.08 ± 2.63, which improved to 9.62 ± 3.34, 5.4 ± 1.98, and 2.83 ± 1.27 at 1, 3, and 6 months post-TURP, respectively (P < 0.001) Fig. 3. Fig. 3. Comparison of International Prostate Symptom Score (IPSS), storage IPSS, maximum urinary flow rate (Qmax), and postvoid residual volume (PVR) between the study groups before TURP and throughout the 6-month follow-up period
The mean (± SD) maximum urinary flow rate (Qmax) in Group A preoperatively was 7.54 ± 2.45, which improved to 16.05 ± 2.05, 20.32 ± 3.15, and 23.41 ± 3.38 at 1, 3, and 6 months postoperatively, respectively (P < 0.001). In Group B, the mean (± SD) Qmax preoperatively was 8.27 ± 2.28, and postoperatively it was 15.22 ± 2.0, 19.00 ± 2.1, and 21.56 ± 3.59 at 1, 3, and 6 months, respectively (P < 0.001) Fig. 3.
Both groups demonstrated a significant improvement in post-void residual urine (PVR), with a reduction observed at 1, 3, and 6 months following TURP. However, the difference between the two groups was not statistically significant (P = 0.2) Fig. 3.
The improvement in the Voiding IPSS score was comparable between the two groups, with no significant difference observed.
A slight improvement in persistent storage symptoms was noted in Group A compared to Group B. The mean (± SD) preoperative storage symptom sub-score in Group A was 8.63 ± 1.82, which improved to 3.05 ± 0.78, 1.63 ± 0.49, and 0.92 ± 0.67 at 1, 3, and 6 months post-TURP, respectively (P < 0.001). In Group B, the mean (± SD) preoperative storage symptom sub-score was 8.03 ± 0.22, which improved to 3.22 ± 0.72, 2.48 ± 0.5, and 1.69 ± 0.47 at 1, 3, and 6 months post-TURP, respectively (P < 0.001) (Table 3).
Nearly all patients were compliant with daily tadalafil usage. Regarding adverse effects, only 13 patients reported mild headaches and runny noses for a short duration. These symptoms did not result in discontinuation of tadalafil treatment.
Discussion
PDE5-I treatment was more effective than placebo in patients with ED following nerve-sparing radical prostatectomy, promoting the recovery of erectile function and potentially protecting against penile structural changes [10].
Tadalafil is safe and effective, and can be used as the first-line medication for the clinical treatment on male ED after transurethral resection of prostate [25].
Administration of 5 mg tadalafil once daily resulted in significant improvements in total International Prostate Symptom Score (IPSS), including both voiding and storage subscores, as well as enhancements in IPSS-related quality of life (QoL) and the BPH Impact Index (BII) [4].
Similarly, in our study, and to the best of our knowledge, this is the first trial to compare the effects of early post-TURP administration of tadalafil 5 mg on persistent storage symptoms and erectile function.
In elderly men, ED and LUTS associated with benign prostatic enlargement (BPE) are highly prevalent comorbid conditions that negatively impact quality of life (QoL) and impose a significant economic burden. Preclinical and clinical studies have established that, in addition to aging, various metabolic factors contribute to the onset and progression of both ED and LUTS, leading to penile and nerve alterations, as well as prostate enlargement and inflammation [8].
TURP is widely recognized as the most effective traditional surgical method for treating BPH. Once the bladder is relieved of obstruction, the thickened bladder wall undergoes atrophy, restoring its elasticity and alleviating irritative symptoms. Notably, the degree of symptom improvement is reported to be particularly high in patients with severe preoperative irritative symptoms [14].
However, a recent study indicated that TURP does not alleviate irritative symptoms in all patients, with 20% to 30% requiring postoperative medication due to persistent symptoms, ultimately leading to a decline in quality of life. Several clinical studies have demonstrated significant improvements in LUTS with the use of PDE5 inhibitors. Although the precise mechanism underlying LUTS improvement with PDE5 inhibitors remains unclear, proposed mechanisms include the relaxation of smooth muscle cells in the urogenital tract via the NO/cGMP/PDE5 pathway [13].
In our study, we observed a significant improvement in erectile function in Group A. The mean (± SD) IIEF score in Group A was 9.84 ± 2.6 before TURP, increasing to 11.59 ± 1.9, 19.8 ± 1.12, and 20.97 ± 0.72 at 1, 3, and 6 months post-TURP, respectively (P < 0.001).
Regarding overall LUTS, both groups demonstrated comparable improvements in IPSS, Qmax, and PVR. However, in Group A, there was a slight greater improvement in persistent irritative symptoms than Group B. The mean (± SD) preoperative storage symptom sub-score was 8.63 ± 1.82, which decreased to 3.05 ± 0.78, 1.63 ± 0.49, and 0.92 ± 0.67 at 1, 3, and 6 months post-TURP, respectively (P < 0.001). Similarly, in the first systematic review on the use of PDE5 inhibitors for LUTS, Laydner et al. reported that PDE5 inhibitors improve the IPSS score and IIEF-5 but do not significantly affect Qmax [15].
Several randomized controlled trials (RCTs) have demonstrated that PDE5 inhibitors significantly reduce IPSS scores, improving both storage and voiding LUTS, and enhancing patients'quality of life. Similarly, a meta-analysis reported significant improvements in IPSS and IIEF scores with PDE5 inhibitor use, though no significant change was observed in Qmax. Additionally, another study found that tadalafil was both effective and well tolerated in the treatment of erectile dysfunction (ED) and LUTS in sexually active men with both conditions, with significant improvements observed irrespective of baseline severity [21].
Limitation of study
This study represents the first prospective trial of penile rehabilitation using tadalafil 5 mg once daily post-TURP. However, several limitations were identified in this study. First, the sample size was relatively small, and therefore, a larger-scale study involving a more extensive population is recommended for more robust conclusions.
Additionally, the study did not compare the outcomes of patients who received tadalafil on demand with those who received tadalafil on a daily basis early postoperatively. Also, Further clinical studies with longer follow-up periods are necessary to comprehensively assess the long-term effects of tadalafil on erectile function and irritative symptoms following transurethral resection of the prostate (TURP).
Conclusion
In comparison to placebo, early Tadalafil 5 mg daily monotherapy after TURP can improve erectile dysfunction. We found that tadalafil 5 mg has a slight improvement in persistent storage symptoms post-TURP.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cui J, Cao D, Bai Y, Wang J, Yin S, Wei W, Xiao Y, Wang J, Wei Q. Efficacy and Safety of 12-week Monotherapy With Once Daily 5 mg Tadalafil for Lower Urinary Tract Symptoms of Benign Prostatic Hyperplasia: Evidence-based Analysis. Front Med (Lausanne). 2021;8. 10.3389/fmed.2021.74401210.3389/fmed.2021.744012 PMC 854599834712682 · doi ↗ · pubmed ↗
- 2Hirahara N, Harikai S, Fujihara A, Yamada Y, Ushijima S, Ukimura O. Efficacy of tadalafil on symptom‐specific bother in men with lower urinary tract symptoms. LUTS: Lower Urinary Tract Symptoms. 2022;14:393–400. 10.1111/luts.1245710.1111/luts.1245735830962 · doi ↗ · pubmed ↗
- 3Yu H, Wu H, Rao D. Analysis of the therapeutic effect of Tadalafil on male ED after transurethral resection of prostate. Int J Impot Res. 2012;24:147–149. 10.1038/ijir.2012.610.1038/ijir.2012.622513502 · doi ↗ · pubmed ↗