COVID-19 safe dental practices among a group of Egyptian students: a cross-sectional study
Dena Ali Abozaid, Dina Hamed, Karim Mostafa Hindy, Mayar Moustafa Budair, Ziad Baher Hussein, Ziyad Islam Hegazy, Dina Nabih Kamel Boulos

TL;DR
This study examines how Egyptian dental students follow safe practices during the pandemic, finding that most have good attitudes and hygiene habits but need improvement in temperature checks and HEPA filter knowledge.
Contribution
The study provides insights into KAP of Egyptian dental students regarding safe dental practices during the pandemic, identifying areas needing curricular improvement.
Findings
88.5% of students had satisfactory safe dental measures practice scores.
Hand hygiene was the most common safe practice (82.7%), while temperature checks were the least common (28.8%).
A moderate correlation was found between safe dental practice scores and attitude scores (r = 0.470).
Abstract
The COVID-19 pandemic has had a tremendous effect on dental practice. Dental practice during the pandemic has been associated with an increased risk of COVID-19 transmission. Adopting proper infection control measures in dentistry helps alleviate the risk of infection. The pandemic has created an even more challenging environment for dentists to perform their job safely, thus necessitating the adoption of very strict infection control measures for safe dental practice. This study aimed to assess the knowledge, attitude, and practice (KAP) regarding COVID-19 safe dental measures among dentistry students currently in clinical training. A cross-sectional study was conducted. The study included a total of 104 dental students, who took clinical practical sessions in a nongovernmental dentistry school, in Egypt. Data collection was performed via an online questionnaire. This study found…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
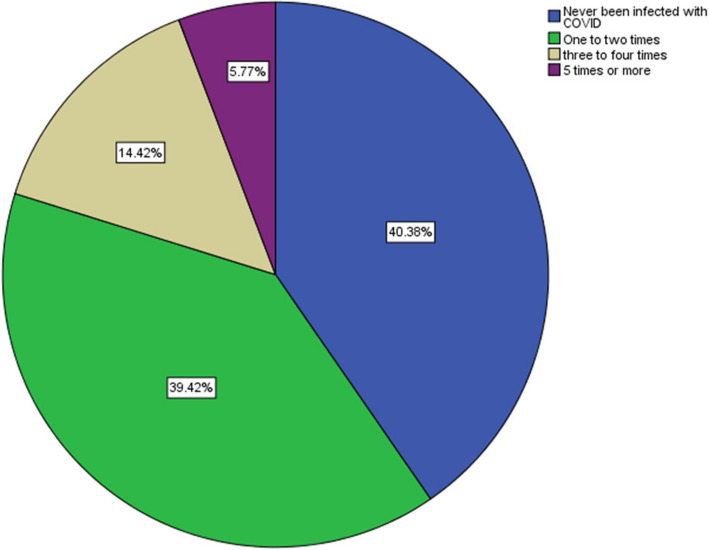 Figure 1
Figure 1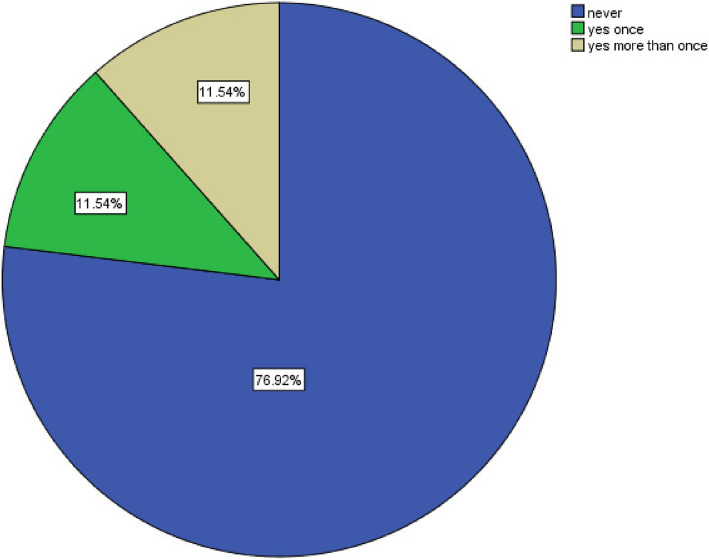 Figure 2
Figure 2- —Ain Shams University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental Research and COVID-19 · COVID-19 diagnosis using AI · Scientific and Engineering Research Topics
Background
Coronavirus disease 2019 (COVID-19) is a newly discovered viral infection that started in Wuhan, China, in December of 2019. Globally, since the start of the COVID-19 pandemic and until August 2nd, 2021, there have been more than 198 million confirmed cases of COVID-19, as well as more than 4 million deaths worldwide [1]. COVID-19 causes severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), a type of lower respiratory tract infection that can be severe and possibly fatal. Preventive measures to control the spread of COVID-19 include careful infection control, patient isolation, and social distancing [2].
The COVID-19 pandemic has been associated with significant occupational risk for healthcare professionals. Owing to their direct contact with patients, inhalation of aerosols released during dental treatments, and contact with contaminated surfaces, dentists are the front-line healthcare workers most at risk of contracting COVID-19 [3]. In Poland, not only was there a sudden drop in the number of dental procedures performed, but also dental care professionals reported experiencing confusion, fear, and anxiety [4]. There is a high risk of infection during dental practice, so it is imperative to adopt strict infection control measures [5]. Airborne contamination can be minimized by adopting proper infection control during all dental procedures [6], which highlights its importance during the COVID-19 pandemic. Previous studies conducted to evaluate infection control measures among dentists during COVID-19 pandemic in USA, Poland and Germany reported a generally strict infection control measure [7–9]. A multicentric study conducted among dental practitioners in low to middle income countries (India, Malaysia, Saudi Arabia, Thailand, Cambodia), as well as Italy reported that nearly half of the dentists felt that it was acceptable to work during the COVID-19 pandemic, as they perceived it as a low-risk situation. Additionally, most of the participants were adhered to infection control measures [10]. On the other hand, a study conducted among Jordanian dentists revealed that, although participants were aware of COVID-19 symptoms and modes of transmission, they had a limited understanding of the extra precautionary methods that would protect them and their patients from the virus, and that only 18% of them considered COVID-19 to be very dangerous [11]. In Egypt, there is scarce information and research that addresses this issue.
Previous studies on infection control practices among dental professionals and students highlight key differences from the current research. A quasi-experimental study conducted before the pandemic at a primary health care (PHC) dental clinic revealed inconsistent adherence to protective measures, with only 20% of participants consistently wearing face masks and 60% using them occasionally. However, the study was limited by its small sample size—20 dentists and 5 nurses—and its confinement to a single district PHC, which may restrict the generalizability of its findings. Additionally, the two-month intervention period raises concerns about its ability to assess long-term adherence to infection control measures [12]. Similarly, a study at Tanta University examined infection control practices among dental students, finding that adherence improved as students advanced in their academic years. More than half demonstrated satisfactory infection control practices, yet the study did not specify whether new dental safety curricula were introduced during the pandemic. Moreover, while acknowledging the university’s hybrid teaching model, it lacked detailed information on the structure of clinical training sessions, including whether students engaged in hands-on practice [13]. These limitations underscore the need for further investigation into the impact of education and training methodologies on infection prevention in dental settings. The current study aimed to assess, students’ knowledge of COVID-19 safe dental measures, attitude towards infection control measures and their perception of the effectiveness of these measures, as well as to measure the frequency of practicing"COVID-19 safe dental measures"among dentistry students. The students in the current study were actively engaged in clinical training, regularly attending dental sessions at the NGU School of Dentistry. Under the supervision of faculty and instructors, they practiced and managed patients, gaining hands-on experience in a controlled academic environment. This study highlights key strengths and gaps in dental education, reinforcing the importance of safety protocols in enhancing professional standards and safeguarding public health. Its findings can contribute to refining the existing curriculum, helping to mitigate risks in dental settings while promoting the long-term well-being of both patients and practitioners.
Subjects and methods
Study design and study settings
A cross-sectional study was conducted at the school of dentistry at Newgiza University (NGU), NGU is a newly established multidisciplinary nongovernmental private university in Egypt, with a partnership with University College London (UCL). NGU education is marked by a strong focus on academic excellence and practical knowledge and ability to deliver a high-quality and contemporary undergraduate dental program, making the NGU dental school a unique experience of learning and an appropriate place to assess infection control and safe dental practices during the COVID-19 pandemic, as the university is very well equipped. The data collection started in 2021 and was completed by the end of 2022.
Study population
This study was conducted among NGU dentistry school students. Students in their clinical training and take dental clinical sessions in the NGU school of dentistry regularly, where they practice and manage patients under the supervision of school staff and instructors, were included in the study. First and second-year students were excluded from the study as they did not have clinical sessions. As part of their regular dentistry curricula, dentistry students at NGU are introduced to infection control measures via group work sessions (2 sessions along the 5-years-dentistry studying, 2 h each). Students learn infection control measures by doing in clinical dentistry classes, where they practice dentistry under supervision of faculty staff and instructors. After COVID-19 pandemic, the university held seminars to increase awareness on COVID-19 modes of infection and respiratory etiquette for all students. Per the teaching curricula, there was an addition of a learning material on oral manifestation of COVID-19 patients, yet no curricula were added regarding the infection control measures for dentists specifically, or regarding safer dental practice in the pandemic.
Sampling methods and sample size
Sample size calculation was performed via Epi Info, and it was assumed that 50% of the dental students adopted satisfactory infection control measures during their clinical dental classes [13]; with confidence level 95% and margin of error 10%, a sample size of 97 participants was found to be enough to achieve study objectives. A total of 104 students were recruited by a non-random convenience sample.
Study tool
An anonymous online self-administered questionnaire was used. The questionnaire was constructed in English language. The questionnaire was constructed based on "safe dental practices during COVID-19" and after reviewing previous literature [14–16]. The questionnaire included the following sections: sociodemographic aspects**,** knowledge about safe dental practice during the COVID-19 pandemic**,** adapted infection control measures in dental practice during the COVID-19 pandemic, and the dentists’ concerns regarding COVID-19 transmission during practice. A practice score was calculated as the sum of 8 questions concerning safe dental practice. The items were in 3-dimensions (all the time = 2, sometimes = 1, and never = 0); a higher score indicates better safe dental practice. Students who scored 8 or more were considered to have safe dental practices during the COVID-19 pandemic. An attitude score was calculated as the sum of 11 questions assessing students’ beliefs about the effectiveness of safe dental practices (items shown. The questions are three dimensions, ranging from 0 to 2, where higher scores reflect a more positive attitude toward safe dental measures. Students who scored 11 or more points were considered to have positive attitude toward safe dental practices. A pilot study to test questionnaire accuracy and comprehensibility was conducted on 15 dental students. Minor changes were adopted on the questionnaire after the pilot study, as rephrasing the questions and enlisting more answer options. The pilot study participants were not included in the study results.
Statistical analysis
The collected data was analysed using the Statistical Package for Social Science (SPSS version 24) program. A suitable analysis was done according to the type of data obtained for each parameter. The Qualitative data was presented in the form of numbers and percentages (proportions). The quantitative data was presented in the form of means and standard deviations.
Ethics approval
Participation in the study was entirely voluntary. The online questionnaire was anonymous, ensuring that no personal or identifiable information was collected. Informed consent was obtained from all participants through a consent statement provided at the beginning of the questionnaire, as well as a disclaimer that the collected data are for research purposes and will be published, and explanation of the research. Confidentiality of all collected data was strictly maintained throughout the study. Approval from the Ethical Committee at NGU was obtained (N.10.2023).
Results
The study included a total of 104 dental students who attended clinical sessions. The participated dentistry students were in the mainly from year years 4 and 3 at the time of the study (52 (50%) and 32 (30.8%), respectively) (Table 1). The most common source of information was the school of dentistry itself (88.5%), followed by World Health Organization fact sheets (68.3%) (Table 2). Table 1. Sociodemographic characteristics of the studied population (n= 104)MeanSDMin.Max.Age21.111.0141923Number%SexMale4240.4%Female6259.6%Academic Year3rd year3230.8%4th year5250.0%5th year2019.2%Table 2. Knowledge regarding safe dental practices during COVID-19 pandemicSource of information for “safe dental practices” during the COVID-19^a^Yes (n%)School of dentistry92 (88.5%)World Health Organization fact sheets71 (68.3%)The Egyptian Ministry of Health69 (66.3%)Published research 48 (46.2%)The Egyptian Dentistry Syndicate37 (35.6%)Center for Disease Control and Prevention35 (33.7%)^a^Items are not mutually exclusive
Per the adopted safe dental measures among the students on their clinical classes, the study shows that additional hand hygiene was the most practiced dental infection control precautionary measures to ensure safe dental practices during the COVID-19 pandemic, with 82.7% of the respondents reporting practicing it all the time. The least adopted measure was checking patient temperature, with only 28.8% of the respondents doing so all the time (Table 3). Table 3. Practice of safe dental measures during COVID-19Items of Safe dental practice score All the timeSometimesNeverN (%)N (%)N (%)Additional hand hygiene86 (82.7%)17 (16.3%)1 (1.00%)Patient masks in waiting area82 (78.8%)16 (15.4%)6 (5.8%)Wearing Face shield49 (47.1%)50 (48.1%)5 (4.8%)Avoidance of aerosol-generating treatments43 (41.3%)40 (38.5%)21 (20.2%)Wearing double gloves42 (40.4%)44 (42.3%)18 (17.3%)Room rotation^^41 (39.4%)29 (27.9%)34 (32.7%)Wearing higher masks as KN95, N95, FFP237 (35.6%)51 (49.0%)16 (15.4%)Checking patient temperature30 (28.8%)34 (32.7%)40 (38.5%)^^Rotating practice between two rooms to limit exposure
Most students believed that the most effective measures for infection control during dental practice is wearing face shields, the patient wearing masks in the waiting area, and additional hand hygiene (Tables 4). Nearly two-thirds of the students believed that their knowledge of safe dental measured were good (Table 5). A total of 88.5% of the dental students had a satisfactory safe dental practice, and 93.2% of the students had a positive attitude towards safe dental measures. There was no statistically significant difference between male and female attitudes toward safe dental measures nor safe dental practice score (Table 6). There was a statistically significant association between age, and satisfactory safe dental practice score (Tables 7). There was a non-statistically significant in the source of knowledge of COVID-19 safe dental measures among male and female students (Table 8). There was a statistically significant association between both practicing hand hygiene and checking patient temperature, and gender (p = 0.023, p = 0.046) respectively (Table 9). There was no statistically significant association between students’ attitude toward safe dental and gender (Table 10). Female students perceived dental practice during COVID-19 as a high risk compared to male students, the difference was statistically significant (p = 0.003). Female students were more concerned compared to male students to get infected with COOVID-19 due to their dental practice (× 2 = 3.914, p = 0.048) (Table 11). Nearly 40% of the students stated that they have never been infected with COVID-19 before (Fig. 1). Nearly 77% of the students have never missing clinical classes due to fear of COVID-19 infection (Fig. 2). Table 4. Students’ attitude towards safe dental measures during COVID-19Items of Safe dental attitude scoreVery effectiveNeutralNot EffectiveN (%)N (%)N (%)Patient masks in waiting area75 (72.1%)27 (26.0%)2 (1.9%)Wearing Face shield70 (67.3%)30 (28.8%)4 (3.8%)Additional hand hygiene69 (66.3%)33 (31.7%)2 (1.9%)Avoidance of aerosol-generating treatments62 (59.6%)36 (34.6%)6 (5.8%)Checking patient temperature57 (54.8%)38 (36.5%)9 (8.7%)Wearing higher masks as KN95, N95, FFP256 (53.8%)42 (40.4%)6 (5.8%)Additional sterilization using UV light lamps53 (51.0%)39 (37.5%)12 (11.5%)Room rotation during practice51 (49.0%)40 (38.5%)13 (12.5%)Wearing double gloves49 (47.1%)38 (36.5%)17 (16.3%)HEPA filters45 (43.3%)42 (40.4%)17 (16.3%)Atomizer in practicing clinic43 (41.3%)44 (42.3%)17 (16.3%)^^Rotating practice between two rooms to limit exposureTable 5Students’ beliefs and perceptions regarding dental measures and patient care during COVID-19 pandemicN%How do you assess risk of COVID19 infection associated with dental practiceLow87.7%Average3028.8%High6663.5%Regular dental care can be maintained during COVID-19 with the proper infection control measureAgree8480.8%Neutral00.0%Disagree2019.2%Dental care should be only for emergency critical situationsAgree4644.2%Neutral1918.3%Disagree3937.5%How do you assess your fear of Being Infected with COVID-19 due to dental practiceConcerned4644.2%Neutral3432.7%Not Concerned2423.1%How do you assess your fear of infecting others with COVID-19 due to dental practiceConcerned5149.0%Neutral3836.5%Not Concerned1514.4%Self-evaluation of knowledge of “safe dental Measures”Good7067.3%Average3028.8%Poor43.8%Self-evaluation of practiced measures against COVID-19Good6461.5%Average3634.6%Poor43.8%Table 6. Practice and attitude scores towards safe dental measures among male and female studentsGenderP valueMale (n= 42)Female (n= 62)N %N %Safe Dental Measures Practice ScoreSatisfactory (n= 92)3788.10%5588.70%0.579Unsatisfactory (n= 12)511.90%711.30%Safe Dental Measures Attitude ScorePositive (n = 97)3992.90%5893.50%0.593Negative (n= 7)37.10%46.50%Table 7. Association between students’ practice and attitude towards safe dental measures and ageAge In YearsP valueMeanSDSafe Dental Measures Practice scoreSatisfactory (n= 92)20.990.8830.013Unsatisfactory (n = 12)21.750.866Safe Dental Measures Attitude ScorePositive (n= 97)21.070.9040.870Negative (n = 7)21.141.069Table 8Sources of information for safe dental measures during COVID-19 among male and female studentsGenderP valueMale (n= 42)Female (n= 62)N%N%NGU school of dentistryYes3685.70%5690.30%0.539The Egyptian ministry of healthYes2661.90%4369.40%0.43The Egyptian dentistry syndicateYes1638.10%2133.90%0.659WHO fact sheetsYes2661.90%4572.60%0.251CDCYes1433.30%2133.90%0.955Published researchYes2047.60%2845.20%0.805Table 9Practicing safe dental measures during COVID-19 among male and female studentsGenderP valueMale (n= 42)Female (n= 62)NColumn %NColumn %Wearing Face shieldAll the time1842.90%3150.00%0.087Sometimes2150.00%2946.80%Never37.10%23.20%Checking patient temperatureAll the time1228.60%1829.00%0.046Sometimes1945.20%1524.20%Never1126.20%2946.80%Wearing double glovesAll the time1535.70%2743.50%0.083Sometimes1945.20%2540.30%Never819.00%1016.10%Wearing higher masks as KN95, N95, FFP2All the time1433.30%2337.10%0.089Sometimes2047.60%3150.00%Never819.00%812.90%Additional hand hygieneAll the time3071.40%5690.30%0.023Sometimes1228.60%58.10%Never00.00%11.60%Patient masks in waiting areaAll the time3378.60%4979.00%0.135Sometimes614.30%1016.10%Never37.10%34.80%Avoidance of aerosol-generating treatmentsAll the time1638.10%2743.50%0.075Sometimes2252.40%1829.00%Never49.50%1727.40%Room RotationAll the time1638.10%2540.30%0.09Sometimes1433.30%1524.20%Never1228.60%2235.50%Table 10. Attitude towards effectiveness of the following measures for a safe dental practice during COVID among male and female studentsGenderMale (n= 42)Female (n= 62)N%N%P valueWearing Face shieldVery Effective2661.9%4471.0%0.342Neutral1433.3%1625.8%Not Effective24.8%23.2%Wearing double glovesVery Effective1842.9%3150.0%0.288Neutral1535.7%2337.1%Not Effective921.4%812.9%Wearing higher masks as KN95, N95, FFP2Very Effective2354.8%3353.2%0.950Neutral1638.1%2641.9%Not Effective37.1%34.8%Additional hand hygieneVery Effective2661.9%4369.4%0.240Neutral1433.3%1930.6%Not Effective24.8%00.0%Additional sterilization using UV light lampsVery Effective1842.9%3556.5%0.186Neutral1842.9%2133.9%Not Effective614.3%69.7%Atomizer in practicing clinicVery Effective1740.5%2641.9%0.332Neutral1535.7%2946.8%Not Effective1023.8%711.3%HEPA filtersVery Effective1740.5%2845.2%0.236Neutral1535.7%2743.5%Not Effective1023.8%711.3%Checking patient temperatureVery Effective2354.8%3454.8%0.423Neutral1842.9%2032.3%Not Effective12.4%812.9%Patient masks in waiting areaVery Effective3173.8%4471.0%0.544Neutral1126.2%1625.8%Not Effective00.0%23.2%Avoidance of aerosol-generating treatmentsVery Effective2457.1%3861.3%0.839Neutral1638.1%2032.3%Not Effective24.8%46.5%Room rotation during practiceVery Effective2457.1%2743.5%0.182Neutral1433.3%2641.9%Not Effective49.5%914.5%Table 11. Beliefs and perceptions regarding dental measures and patient care during COVID-19 pandemic among male and female students GenderP valueMale (n= 42)Female (n= 62)N%N%Risk of COVID19 infection associated with dental practiceLow716.7%11.6%Average1433.3%1625.8%0.003High2150.0%4572.6%Regular dental care can be maintained during COVID-19 with the proper infection control measureAgree1535.7%3150.0%0.641Neutral1331.0%2133.9%Disagree1433.3%1016.1%Dental care should be only for emergency critical situationsAgree1842.9%3353.2%Neutral1535.7%2337.1%0.484Disagree921.4%69.7%How do you assess your fear of Being Infected with COVID-19 due to dental practiceConcerned2764.3%4369.4%Neutral1535.7%1524.2%0.048Not Concerned00.0%46.5%How do you assess your fear of infecting others with COVID-19 due to dental practiceConcerned2969.0%3556.5%0.125Neutral1228.6%2438.7%Not Concerned12.4%34.8%Self-evaluation of knowledge of “safe dental Measures”Good1945.2%2743.5%Average1023.8%914.5%0.901Poor1331.0%2641.9%Self-evaluation of the quality of practiced measures against COVID-19Good3378.6%5182.3%Average00.0%00.0%0.186Poor921.4%1117.7%Fig. 1. Frequency of COVID-19 infection during the past 12 monthsFig. 2Frequency of skipping dental classes for fear of COVID-19 infection
Discussion
This research provides insight not only into safe dental practices during the COVID-19 pandemic but also, into the standard infection control measures needed for safe dental practice. Dentists are at risk of becoming infected or infecting patients during their practice [6]. On a daily basis, dentists are in contact with multiple sources of infection, such as the patient's saliva, contaminated materials, and dental surfaces [17]. Dental practice during the pandemic subsequently increased the risk of COVID-19 transmission. These findings demonstrate the importance of possessing sufficient knowledge and training not only to protect against COVID-19 but also as a guideline for safe dental practice in general. The current study revealed that more than half of the dental students self-evaluated their safe dental measures during clinical dental classes as “good” (61.5%).
With respect to the students’ sources of information, the main sources of information on safe dental practices during the COVID-19 pandemic were the school of dentistry itself and the World Health Organization website, which are credible medical sources and trusted governmental institutions, confirming that the students had reliable high-quality information regarding safe dental practices. A study conducted in six sub-Saharan countries reported that more than half of participants relied on social media as a source of COVID-19-related information and that those who relied on social media as a source of information agreed more readily with the effectiveness of masks than did those who did not rely on social media (AOR 1.33, 95% CI: 1.01–1.77) [18]. Moreover, a study conducted among a group of Ethiopian healthcare workers reported that nearly half of the participants relied on social media as a source for COVID-19 information [19], which proposed social media as a good source of safe dental practice information. Yet, a study conducted in Jordan reported that most medical students (83.4%) relied on social media to gain information about COVID-19; however, only 9.7% of the students used face masks routinely, and only 19.3% believed that face masks were effective [20]. These findings suggest that the source of information has an impact on the safety of dental knowledge, attitude, and practice of students. Social media, as a source of health information, has both advantages and advantages. It can be a communication tool and a portal for international and governmental health organizations to offer valid and reliable health information. However, social media lacks an accuracy checker to validate the information. Moreover, social media algorithms suggest content based on user’s activity. This may lead to the dissemination of false knowledge and rumors. While social media offers a tool to disseminate information, its use in health should be used with caution and not as a replacement for medical school and professional organization information. In the current study the students primarily relied on the knowledge disseminated through the school itself regarding COVID-19. As part of their regular dentistry curricula, dentistry students at NGU are introduced to infection control measures via group work sessions (2 sessions along the 5-years-dentistry studying, 2 h each). Students were taught the infection control measures in clinical dentistry classes, where they practiced dentistry under supervision of faculty staff and instructors. After COVID-19 pandemic, the university held seminars to increase awareness on COVID-19 modes of infection and respiratory etiquette for all students, which seemed satisfactory for the students as (67.3%) and (61.5%) self-evaluated their knowledge and practice of safe dental measures as good. Moreover, the current study showed that most of the dental students had a positive attitude score as well as a satisfactory practice score of safe dental measures. Moreover, nearly 40% of the students stated that they have never been infected with COVID-19. However, some area needed improvement, and more effort is needed to raise students’ awareness of the importance of measuring patient temperature, using advanced sterilization techniques, especially that the students reported that they were only and added teaching session during the pandemic on oral manifestation of COVID-19 patients, yet no curricula were added regarding the additional infection control measures dentists specifically should apply to have a safe practice during the pandemic.
Since the emergence of the COVID-19 pandemic, attention has been given to dental practices, and precautionary measures have been implemented. This study highlighted concerns related to the increased risk of infection associated with dental practices. Many studies have shown a growing tendency to limit dental practice to emergency cases only during the pandemic. In a study conducted in Brazil, 64.6% of dentists attended only emergency treatments during the pandemic [21]. Similarly, a study in China revealed that patients themselves were reducing their visits to the dentist, with a 70% reduction in patients seeking nonurgent dental services during the pandemic [22]. Moreover, a study conducted in Egypt among dental students at a governmental university reported that 68.2% of the students wished that they could stop their dental practice during the pandemic [13]. These results reflect the shared concern that dental procedures pose a high risk of transmission worldwide. The participants in the current study also reported concerns about becoming infected or infecting others during their practice. This finding is consistent with another study in which dentists feared contracting COVID-19 due to their profession and feared infecting their family members [23]. Results of the present study showed that gender influenced the students’ tendency to abide by infection control and safety measures. With respect to safe dental practices during the COVID-19 pandemic, most female students practiced hand hygiene (90.3%), whereas (71.4%) of male students did. Similarly, a study conducted in Saudi Arabia, showed that female dental students had higher compliance with safe dental practices [24]. The results of the present study also revealed that only (26.2%) of the male students “never” checked patient temperature, whereas (46.8%) of the female students did. These results contradict those of Younis et al. [13] who reported a statistically nonsignificant association between sex and safe dental practice scores.
The results of the present study revealed that age was associated with having a satisfactory safe dental measures practice score. Similarly, previous study revealed that more senior students than junior students had safe dental practice scores [13]. A study in Turkey reported that clinical students had higher health anxiety inventory scores than non-clinical students did; however, the study did not report any difference in anxiety scores across different age groups [25]. This may be associated with senior students feeling less concerned, more experienced, or more confident, which could be linked to a more relaxed approach and less strict adherence to infection control and safe dental practice measures. However, the present study did not find any statistically significant difference in the level of students’ concern and fear of COVID-19 according to academic year or age.
On the NGU campus, COVID-19 vaccination campaigns were launched during the 2021–2022 academic year, as COVID-19 vaccination was mandatory for school enrollment, and all students were vaccinated with the COVID-19 vaccine. The results of the present study revealed that most of the students reported being infected with COVID-19, as 41% of the respondents experienced one to two COVID-19 infections. These rates are expected since the field of dentistry requires close contact with patients, thereby increasing the risk of infection transmission. The COVID-19 infection rates reported in this study are similar to rates reported among medical students in a study conducted in Jordan, where 34.6% of the students reported COVID-19 infection [26]. This highlights that routine infection control measures as hand wash are just not enough alone for prevention of COVID-19 infections, as 38.5% of the students never checked for patient temperature, and 32.7% never adopted room rotation to avoid risk of COVID-19 as advised in the guidelines [27].
More than half of the students (68.3%) believed that their safe dental practice knowledge was “good or very good”. This could be explained by the infection control protocols mandated by the university itself. The School of Dentistry protocol prohibits students from working in labs without proper use of personal protective equipment PPE. The results also revealed that fewer than one-third of the students had skipped clinical classes due to fear of infection; moreover, 76.9% of the students never skipped practical sessions in fear of becoming infected. This could be due to their trust in PPE; yet this may also be due to the university’s strict attendance policies.
The current study revealed that the most common practiced safety measure used hand hygiene (82.7%). This reflects individuals’ dedication to limiting the spread of COVID-19, especially as hand hygiene is the most feasible and efficient method to prevent transmission [28]. The current study revealed that the students were aware of the high risk of infection associated with dental practice, as 63.5% of the students believed that the risk of infection during dental practice was high, which reflects a high awareness of hazards associated with dental practice among the students. Unexpectedly, checking patients’ temperature was the least safe dental practice measure adopted among the students, and only 28.8% of the students reported practicing it. Checking a patient’s temperature is a safety measure that can be performed quickly and regularly, which is why it is expected to be done as frequently as the hand hygiene. Not measuring the temperature of the patients, nor taking history of fever or use of antipyretics can strongly increase the risk of infection [29].
The current study revealed that 16.3% of the students believed that HEPA filters and using atomizer were not effective measures for safe dental practice. This is an unexpected result since the use of HEPA filters is an exceptional method for preventing air borne infections. The filters remove bioaerosols from the air, eliminating contaminants [30]. Moreover, 16.3% of the current study participants believed that wearing double gloves was not effective in reducing infections among dentists. Similarly, a study conducted in India among interns, dental postgraduate students, and dental faculty members reported that 5.2%, 12.1%, and 12.7% of the participants, respectively, believed that wearing double gloves was not effective in reducing infections [31]. Dentists are exposed to pathogens during their practice and wearing double gloves reduces the risk of microorganism transmission for safer practice [32, 33]. This highlights that students’ attitude toward necessity and effectiveness of wearing gloves during dental practice still need further improvement. The current study showed that female dental students were more concerned about the risk of COVID-19 infection and subsequently more adherent to most of the precautionary infection control measures compared to their male colleagues. This finding is consistent with a previous study conducted in Egypt which reported that female dentists were more adherent to COVID-19 infection control measures [34].
More than one third (35.6%) of the students used (KN95, N95, FFP2) masks “all the time”, and 50% used them “sometimes” during their practice. This finding aligns with that of Ameena et al. [35], who surveyed dental practitioners, dental house surgeons, postgraduate students, and teaching faculty, and reported that nearly half of them (54.7%) used N95 masks while performing aerosol-generating procedures and that 10.3% of the study participants used both regular masks and N95 masks [35]. Only 53.8% of the studied students believed that wearing the before mentioned types of masks was an effective precautionary measure for safe dental practice. This is true, as using these masks was the most efficient solution to prevent infection as revealed in a study that analyzed coughing and COVID-19 transmission [36]. Similarly, a study conducted among specialized dentists revealed that more than three fourths of the specialists (78.7%) believed that the N-95 mask was effective in protecting against COVID-19, and 67.3% believed hand washing to be effective [37]. Additionally, a study of Jordanian dentists showed that, most of them (92.2%) were compliant with safe dental practice measures as goggles, masks, and gloves [11]. Compared with the students in our study, the increase in age and dental years of experience improved dentists’ knowledge and perceptions of the adopted precautionary measures.
Conclusions and Recommendations
The current study highlights key strengths and gaps in dental education, reinforcing the importance of safety protocols in enhancing professional standards and safeguarding public health. The current study showed that most dental students were aware of preventive measures, demonstrated a positive attitude and reported incorporating them into clinical dental sessions during the COVID-19 pandemic. The infection control practices adopted during this period may serve as a foundation for enhancing routine dental infection control protocols. Nevertheless, there is still room for improvement, a more structured and detailed curriculum on infection control measures may be beneficial—particularly in areas such as consistent patient temperature monitoring and improving students’ understanding and attitude toward the use of HEPA filters. Incorporating a mandatory patient temperature screening is warrented. Future research, especially multicenter studies involving governmental dental schools and practicing dentists, could provide broader insights and help shape interventions to strengthen safe dental practices.
Limitations
This study has several limitations. It was conducted at a single private dental school with a relatively small sample size, which may limit generalizability—particularly to public dental faculties with different resources and conditions. The use of convenience sampling may have introduced selection bias, as participants who were more available or willing to respond may not represent the broader student population. Data were collected through self-reported questionnaires, which are subject to recall and social desirability biases, and students’ actual clinical behaviour was not confirmed by observation. These may be associated with overreporting of positive behaviors or attitude.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization. data.who.int, WHO Coronavirus (COVID-19) dashboard > Deaths [Dashboard]. 2023. https://data.who.int/dashboards/covid 19/deaths. Website last Accessed June 2024.
- 2Tysiąc-Miśta M and Dziedzic A. The Attitudes and Professional Approaches of Dental Practitioners during the COVID-19 Outbreak in Poland: A Cross-Sectional Survey. Int J Environ Res Public Health. 2020;17 (13):4703. 10.3390/ijerph 17134703. Published 30 Jun 2020.10.3390/ijerph 17134703 PMC 737019632629915 · doi ↗ · pubmed ↗
- 3Upendran A, Gupta R and Geiger Z. Dental Infection Control. In: Stat Pearls. Treasure Island (FL): Stat Pearls Publishing. 2024. Available from: https://www.ncbi.nlm.nih.gov/books/NBK 470356/.29261939 · pubmed ↗
- 4Harrel SK and Molinari J. Aerosols and splatter in dentistry: a brief review of the literature and infection control implications. J Am Dent Assoc. 2004;135(4):429–7. 10.14219/jada.archive.2004.0207.10.14219/jada.archive.2004.0207 PMC 709385115127864 · doi ↗ · pubmed ↗
- 5Lucaciu O, Boca A, Mesaros AS, Petrescu N, Aghiorghiesei O, Mirica IC, Hosu I, Armencea G, Bran S and Dinu CM. Assessing SARS-Co V-2 Infection Rate among Romanian Dental Practitioners. Int J Environ Res Public Health. 2021;4(18)9:4897. 10.3390/ijerph 18094897. PMID: 34064469; PMCID: PMC 8124498.10.3390/ijerph 18094897 PMC 812449834064469 · doi ↗ · pubmed ↗
- 6Farahat MT, Hegazy N and Mohammed MA. The Egyptian Journal of Hospital Medicine. The Assessment of Infection Control Measures in Dental Clinics Primary Health Care, Bilqas,Dakahlia. 2020; 81(3):1621–7. https://journals.ekb.eg/article_116806_405794 c 384d 9a 91401 d 3ec 226cb 4eea 9.pdf.
- 7Centers for Disease Control and Prevention. (n.d.). Standard Precautions for All Dental Health Care Personnel. https://www.cdc.gov/dental-infection-control/hcp/summary/standard-precautions.html. Website last Accessed June 2024
- 8Shi Adrian H, Guo W, Chng CK and Chan BH. “Precautions When Providing Dental Care During Coronavirus Disease 2019 (COVID-19) Pandemic.” Ann Acad Med Singapore. 2020;49:312–19. 10.47102/annals-acadmedsg.2020111.32582908 · pubmed ↗