Pubic Osteomyelitis Identified on Follow-Up MRI Following Adductor Myositis in a Patient With Escherichia coli Bacteremia
Hisashi Ishikawa, Kazuki Ocho

TL;DR
A patient with Escherichia coli bacteremia developed pubic osteomyelitis after initial imaging missed the infection, highlighting the importance of follow-up imaging in persistent cases.
Contribution
This case emphasizes the dynamic progression of musculoskeletal infections and the value of repeat MRI in diagnosing delayed bone involvement.
Findings
Initial MRI failed to detect pubic osteomyelitis despite persistent symptoms.
Follow-up MRI on day 13 revealed pubic bone marrow edema confirming osteomyelitis.
A 12-week antimicrobial course resolved the infection after diagnosis.
Abstract
A previously healthy 54-year-old man presented with a high-grade fever and bilateral groin pain. Initial non-contrast imaging failed to identify an infectious focus, while blood cultures revealed the presence of Escherichia coli. Pelvic MRI on hospital day 5 demonstrated bilateral adductor brevis myositis without osseous involvement. Despite antimicrobial therapy, symptoms persisted. Follow-up MRI on hospital day 13 revealed new pubic bone marrow edema, confirming a diagnosis of pubic osteomyelitis. The patient was successfully treated with a 12-week course of antimicrobial therapy, resulting in clinical resolution. This case illustrates a key diagnostic challenge in gram-negative bacteremia: musculoskeletal infections can evolve dynamically, and early imaging may underestimate the extent of the disease. The anatomical continuity between muscle and bone enables the contiguous spread of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
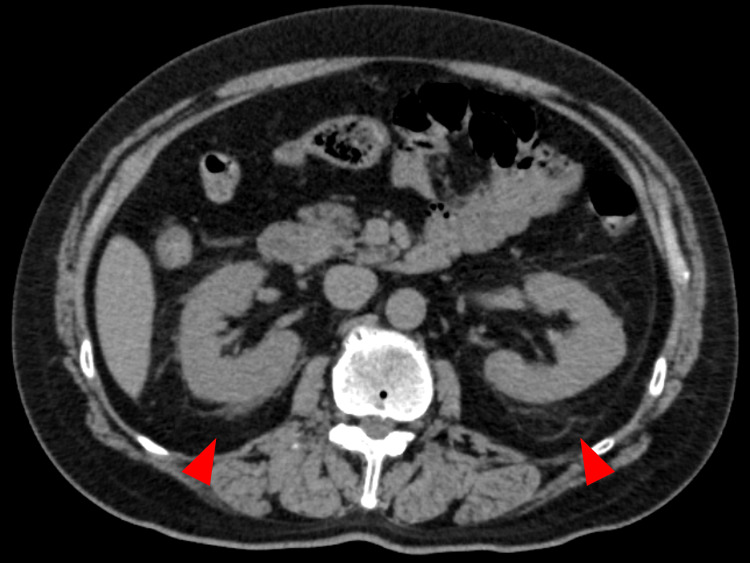 Figure 1
Figure 1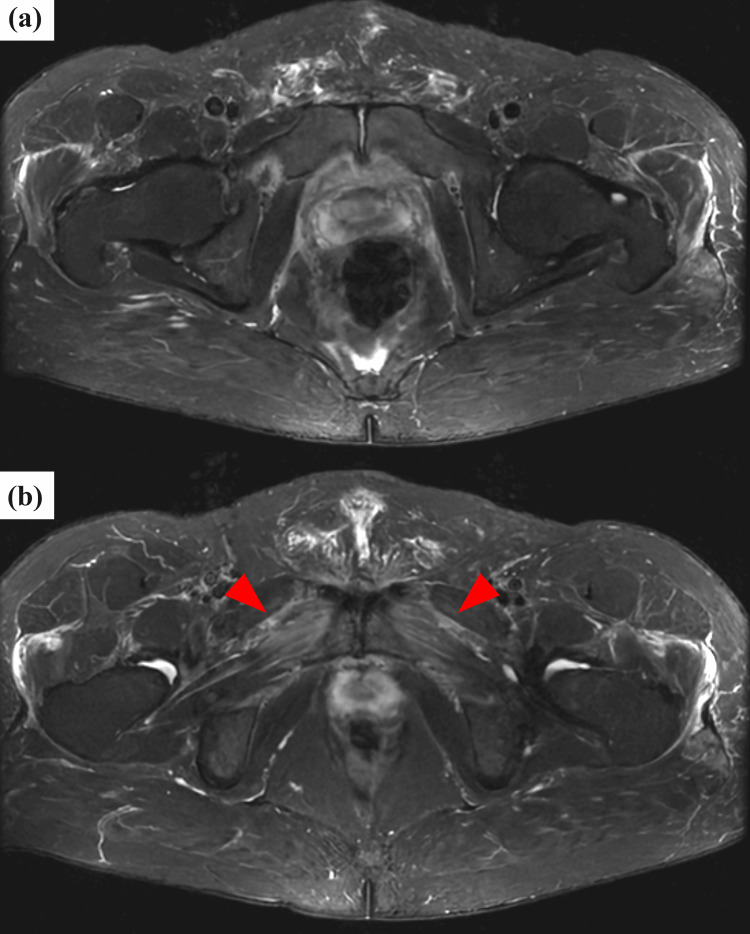 Figure 2
Figure 2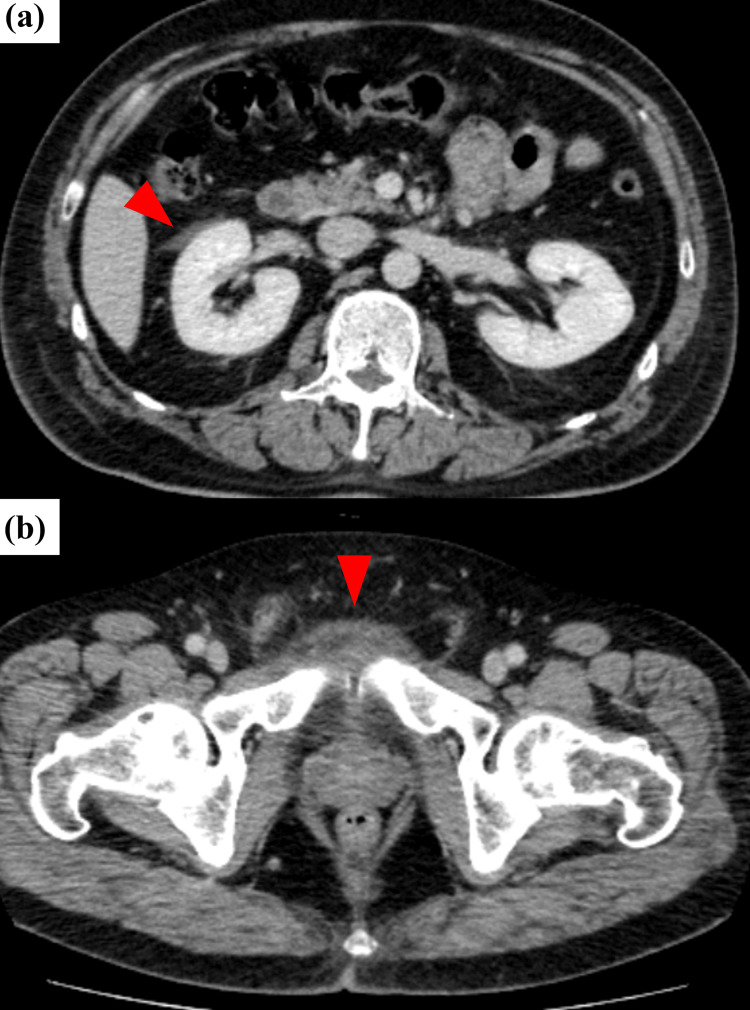 Figure 3
Figure 3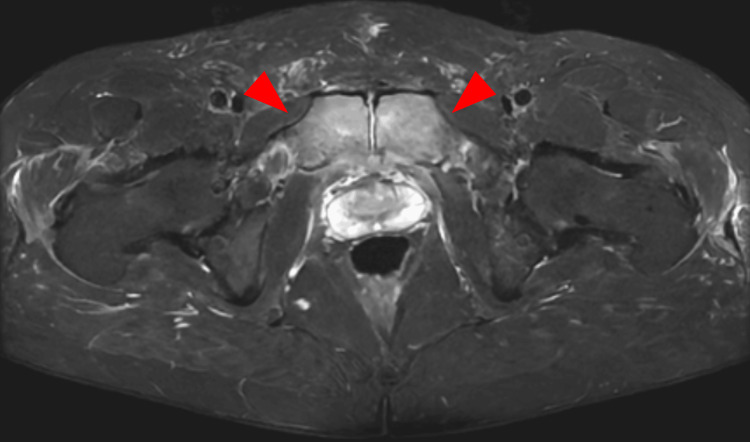 Figure 4
Figure 4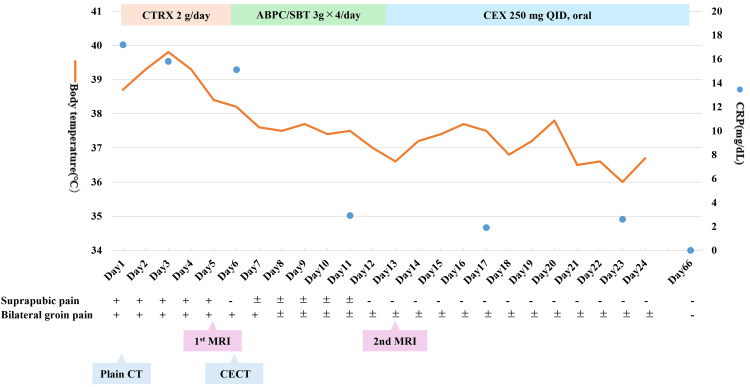 Figure 5
Figure 5| Parameter | Result | Unit | Reference range |
| WBC | 6730 | /μL | 3500-9000 |
| Neut | 94.0 | % | 42-74 |
| Lym | 3.9 | % | 18-50 |
| Mon | 1.8 | % | 2-9 |
| Eos | 0.0 | % | 0-7 |
| Bas | 0.3 | % | 0-2 |
| RBC | 539 | ×106/μL | 438-577 |
| Hb | 15.7 | g/dL | 13.6-18.3 |
| Hct | 47.4 | % | 40.4-51.9 |
| MCV | 87.9 | fL | 76-96 |
| MCH | 29.1 | pg | 27-32 |
| MCHC | 33.1 | g/dL | 31-51 |
| Plt | 9.9 | ×104/μL | 14.0-37.9 |
| PT | 12.9 | S | 8.0-12.0 |
| APTT | 29.8 | S | 26.0-38.0 |
| D-dimer | 56.2 | μg/mL | 0.0-1.0 |
| TP | 6.5 | g/dL | 6.5-8.2 |
| Alb | 4.0 | g/dL | 3.7-5.5 |
| T-Bil | 1.3 | mg/dL | 0.2-1.0 |
| D-Bil | 0.3 | mg/dL | 0.0-0.3 |
| AST | 25 | U/L | 10-40 |
| ALT | 22 | U/L | 5-45 |
| ALP | 49 | U/L | 38-113 |
| γ-GT | 23 | U/L | 0-79 |
| LDH | 184 | U/L | 120-245 |
| CK | 343 | U/L | 50-230 |
| T-CHO | 169 | U/L | 150-219 |
| BUN | 20.2 | mg/dL | 8.0-20.0 |
| Cr | 1.17 | mg/dL | 0.65-1.09 |
| UA | 4.1 | mg/dL | 3.6-7.0 |
| Na | 135.6 | mmol/L | 135-145 |
| K | 3.4 | mmol/L | 3.5-5.0 |
| Cl | 98.3 | mmol/L | 98-108 |
| Ca | 8.9 | mg/dL | 8.2-10.0 |
| Glu | 160 | mg/dL | 80-140 |
| HbA1c | 5.6 | % | 4.6-6.2 |
| CRP | 17.2 | mg/dL | 0.-0.29 |
| TSH | 0.786 | mIU/mL | 0.61-4.23 |
| NT-proBNP | 283 | pg/mL | 0-125 |
| PSA | 0.521 | ng/mL | 0.0-3.9 |
| HBsAg | 0.00 | IU/mL | 0.00-0.02 |
| HCVAb | 0.0 | IU/mL | 0.0-0.9 |
| Urine-pH | 5.5 | 5.0–8.0 | |
| Urine-protein | (3+) | (-)~(±) | |
| Urine-RBC | 10-19 | 0–4 /HPF | |
| Urine-WBC | 1-4 | 0–4 /HPF | |
| Urine-nitrite | (-) | (-) | |
| Urine-bacteria | (1+) | (-) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Diseases and Tuberculosis · Orthopedic Infections and Treatments · Streptococcal Infections and Treatments
Introduction
Musculoskeletal infections secondary to gram-negative bacteremia are diagnostically challenging, particularly when no clear source of infection is identified on initial evaluation [1]. Escherichia coli, although commonly associated with urinary tract infections, can also cause metastatic infections, such as pyomyositis and osteomyelitis [2]. Among imaging modalities, MRI is considered the most sensitive for detecting soft tissue and marrow abnormalities in these conditions [3].
Pubic osteomyelitis is an uncommon but clinically significant form of bone infection, typically associated with trauma, pelvic procedures, or urologic interventions. Its presentation in immunocompetent adults without predisposing factors is particularly rare and may be misdiagnosed or diagnosed late due to its variable symptoms and low clinical suspicion [2]. The anatomical proximity of the pubic bone to the adductor muscle origins provides a plausible route for contiguous infection spread, especially in the setting of hematogenous seeding [4].
This report describes a case in which Escherichia coli bacteremia initially manifested as adductor myositis, later evolving into pubic osteomyelitis. A follow-up MRI, prompted by persistent symptoms, captured the progression. This case highlights the importance of clinical vigilance, symptom-guided reassessment, and the utility of interval imaging in the dynamic management of musculoskeletal infections [1].
Case presentation
A 54-year-old man employed by the municipal water department presented with two days of high-grade fever (maximum 40°C), bilateral groin pain, and suprapubic pain. His occupation involved routine dam inspections with moderate physical exertion, but there had been no recent trauma or unusually intense activity. He had no history of diabetes mellitus, immunosuppression, or other significant comorbidities.
On admission (day 1), physical examination revealed tenderness over the suprapubic area and bilateral groins. Passive extension of the hips elicited pain, and ambulation was limited. Hip range of motion was moderately restricted due to pain, but there were no neurological deficits or joint effusions.
Initial laboratory investigations revealed a white blood cell count of 6730/μL, C-reactive protein (CRP) 17.2 mg/dL, and D-dimer 56.2 μg/mL. Urinalysis showed bacteriuria, although both initial and post-prostatic massage urine cultures were negative. The prostate was non-tender and non-enlarged on digital rectal examination. A summary of the patient’s laboratory findings on admission is provided in Table 1.
Non-contrast abdominal CT performed on admission (day 1) demonstrated mild bilateral perinephric fat stranding (Figure 1). Empiric intravenous ceftriaxone (2 g/day) was initiated for suspected bacteremia of urinary or musculoskeletal origin. Blood cultures drawn on admission grew Escherichia coli, which was susceptible to β-lactam antibiotics and resistant only to azithromycin. Repeat blood cultures on day 17 were negative, confirming microbiological clearance.
Non-contrast axial abdominal CT on admissionMild bilateral perinephric fat stranding is noted (arrowheads), raising suspicion for a urinary tract infection as the potential source of bacteremia.CT: computed tomography
On hospital day 5, pelvic MRI (STIR sequence) revealed bilateral adductor brevis myositis without osseous involvement (Figure 2). Symptoms persisted, and contrast-enhanced CT on day 6 showed perinephric fluid and fat stranding around the pubic symphysis (Figure 3). In response, antibiotics were escalated to sulbactam/ampicillin (3 g every six hours) from day 7 to day 13. Follow-up pelvic MRI on day 13 revealed new bone marrow edema in the pubic bone, consistent with osteomyelitis (Figure 4).
Pelvic MRI (STIR sequence) on hospital day 5(a) No abnormal signal is observed in the pubic bone. (b) Symmetric high signal intensity is present in the bilateral adductor brevis muscles (arrowheads), localized to their proximal origin, consistent with early myositis and without osseous involvement at this stage.MRI: magnetic resonance imaging, STIR: short tau inversion recovery
Contrast-enhanced abdominal and pelvic CT on hospital day 6(a) A loculated fluid collection measuring approximately 2–3 cm is observed in the right perinephric space (arrow), without signs of abscess or gas formation, suggestive of transient inflammation. (b) Fat stranding anterior to the pubic symphysis, new compared to prior imaging, suggests evolving pelvic inflammation.CT: computed tomography
Pelvic MRI (STIR sequence) on hospital day 13Diffuse high signal intensity involving the bilateral pubic bone marrow (arrowheads) is observed, consistent with osteomyelitis. This represents progression from earlier MRI findings of isolated myositis without osseous involvement.MRI: magnetic resonance imaging, STIR: short tau inversion recovery
The patient’s fever gradually resolved, and CRP levels declined during treatment. He was transitioned to oral cephalexin (250 mg QID) on day 14. He was discharged on day 23 in stable condition and completed a total of 12 weeks of antimicrobial therapy as an outpatient. At follow-up, he remained clinically well, without recurrence of symptoms. A timeline summarizing body temperature, CRP trends, antimicrobial regimen, imaging study dates, and the evolution of suprapubic and groin pain is presented in Figure 5.
Clinical timeline integrating symptoms, body temperature, CRP, imaging, and antimicrobial therapyThis figure summarizes the patient's clinical course, including body temperature (orange line) and CRP values (blue dots), over the course of hospitalization and follow-up. Antimicrobial regimens are shown as colored bars. Key imaging studies, including non-contrast CT, contrast-enhanced CT, and pelvic MRI, are annotated. The presence and improvement of suprapubic and bilateral groin pain are represented using symbols: “+” (present), “±” (improved), and “−” (resolved).CRP: C-reactive protein, CT: computed tomography, MRI: magnetic resonance imaging, CTRX: ceftriaxone, ABPC/SBT: ampicillin/sulbactam, CEX: cephalexin, QID: quater in die, CECT: contrast-enhanced computed tomography
Discussion
This case illustrates the dynamic evolution of musculoskeletal infection in the context of Escherichia coli bacteremia, progressing from adductor myositis to pubic osteomyelitis. While Escherichia coli is a common cause of urinary tract infections, its ability to produce metastatic musculoskeletal involvement is less frequently appreciated, particularly in immunocompetent hosts [5]. The anatomical proximity of the adductor brevis origin to the pubic bone allows for direct contiguous spread of infection, as demonstrated radiologically and clinically in this case [2,4].
Initial MRI on hospital day 5 revealed bilateral adductor brevis myositis without osseous involvement, while follow-up MRI on day 13 confirmed new bone marrow edema consistent with osteomyelitis [6]. This progression underscores the importance of symptom-guided interval imaging, particularly when early studies are inconclusive or symptoms persist [6,7]. Although the utility of repeat imaging is well recognized in vertebral osteomyelitis, its role in non-vertebral cases is less frequently emphasized. Considering the anatomical variability and lower clinical suspicion in non-spinal sites, routine reassessment may be underutilized [7].
Empiric ceftriaxone therapy was selected for the initial management of suspected gram-negative bacteremia. This choice is supported by current clinical guidance and widely accepted as an appropriate first-line agent for community-acquired Escherichia coli infections, including those with potential musculoskeletal involvement [8]. Due to persistent symptoms and evolving imaging findings, therapy was escalated to sulbactam/ampicillin. Following clinical improvement and microbiological confirmation of β-lactam susceptibility, the patient was transitioned to oral cephalexin. This stepwise approach, combining initial intravenous therapy with a switch to oral agents based on clinical response and pathogen susceptibility, reflects principles supported by both observational studies and randomized trials evaluating antibiotic strategies for bone and joint infections [9]. Notably, the resistance profile of the isolate, susceptibility to β-lactams, and resistance to azithromycin were consistent with patterns commonly observed in community-acquired strains of Escherichia coli [10]. While molecular typing was not performed, the clinical pattern supports hematogenous seeding and contiguous spread.
This case also highlights the diagnostic challenge posed by pubic osteomyelitis, a rare and often underrecognized entity. Its presentation may mimic other causes of lower abdominal or pelvic pain, including athletic pubalgia, prostatitis, or pelvic insufficiency fractures, often leading to diagnostic delay. Awareness of the anatomical relationship between the pubic symphysis and surrounding musculature, and careful integration of imaging findings with evolving symptoms, is crucial for timely diagnosis.
Although the patient responded well to a 12-week course of antibiotics, the optimal duration of therapy for pubic osteomyelitis remains uncertain and should be individualized. Several guidelines and case series support durations ranging from six to 12 weeks, with decisions guided by clinical response, inflammatory markers, and radiologic improvement. In this case, the resolution of fever, normalization of CRP, and improvement on follow-up imaging collectively supported the completion of treatment.
Conclusions
This case highlights a key diagnostic principle: musculoskeletal infections can evolve over time, and initial imaging may underestimate the extent of the disease. The progression from adductor myositis to pubic osteomyelitis illustrates the anatomical continuity that can facilitate the spread of infection, even in immunocompetent individuals.
Symptom-guided repeat MRI was crucial for identifying delayed osseous involvement. This emphasizes the importance of clinical judgment and interval imaging in patients with gram-negative bacteremia and musculoskeletal symptoms. A structured timeline helped visualize the interplay between symptoms, diagnostics, and therapy, offering a useful model for managing similar cases.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Magnetic resonance imaging of musculoskeletal infections Pol J Radiol Weaver JS Omar IM Mar WA 14116287202210.5114/pjr.2022.113825 PMC 904786635505859 · doi ↗ · pubmed ↗
- 2Osteomyelitis of the pelvic bones: a multidisciplinary approach to treatment J Bone Jt Infect Dudareva M Ferguson J Riley N Stubbs D Atkins B Mc Nally M 184193220172911907710.7150/jbji.21692 PMC 5671931 · doi ↗ · pubmed ↗
- 3The role of MRI in musculoskeletal practice: a clinical perspective J Man Manip Ther Dean Deyle G 1521611920112285187810.1179/2042618611 Y.0000000009 PMC 3143009 · doi ↗ · pubmed ↗
- 4Osteomyelitis 5 2025 2017 https://radsource.us/osteomyelitis/
- 5Septic arthritis and osteomyelitis of the pubic symphysis - a retrospective study of 26 patients J Bone Jt Infect Hansen RL Bue M Borgognoni AB Petersen KK 354272022 https://jbji.copernicus.org/articles/7/35/2022/3525190310.5194/jbji-7-35-2022 PMC 8892565 · doi ↗ · pubmed ↗
- 6Magnetic resonance imaging of musculoskeletal infections Pol J Radiol Weaver JS Omar IM Mar WA 141162872022 https://www.termedia.pl/Journal/-126/pdf-46472-1010.5114/pjr.2022.113825 PMC 904786635505859 · doi ↗ · pubmed ↗
- 7Musculoskeletal infection: role of CT in the emergency department Radiographics Fayad LM Carrino JA Fishman EK 172317362720071802551410.1148/rg.276075033 · doi ↗ · pubmed ↗
- 82015 Infectious Diseases Society of America (IDSA) clinical practice guidelines for the diagnosis and treatment of Native vertebral osteomyelitis in adults Clin Infect Dis Berbari EF Kanj SS Kowalski TJ 264661201510.1093/cid/civ 48226229122 · doi ↗ · pubmed ↗