Hepatobiliary Complications Associated With Ketamine Use: Clinical Insights and Future Directions
Hafiza Wajeeha Waheed, Muhammad R Ashraf, Talha Sajjad, Hanzala Jehangir, Iqra Baig, Ahmad Zulaid, Abdul Rehman Nasir, Allah Dad

TL;DR
This paper reviews how ketamine use can affect liver and bile function, highlighting potential complications and the need for further research.
Contribution
The paper provides a comprehensive review of ketamine's hepatobiliary effects and proposes future research directions.
Findings
Ketamine use is linked to liver enzyme changes and biliary disruptions.
Discontinuation of ketamine often leads to improvement in liver function.
Possible mechanisms include bile flow issues and oxidative stress.
Abstract
Ketamine has been utilized in various medical contexts, particularly for its effects on the nervous system. Over time, its applications have expanded beyond its initial use, with emerging interest in its potential to influence mood and cognition. In certain clinical populations, it has been associated with a rapid reduction in depressive symptoms and suicidal thoughts, particularly when conventional treatments have proven insufficient. Despite these promising therapeutic effects, concerns remain regarding possible adverse consequences, including those related to liver and biliary function. This review explores the current understanding of how ketamine use may impact hepatic and biliary health, with a focus on observed complications, possible underlying mechanisms, clinical manifestations, and available management strategies. A structured examination of existing medical literature was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
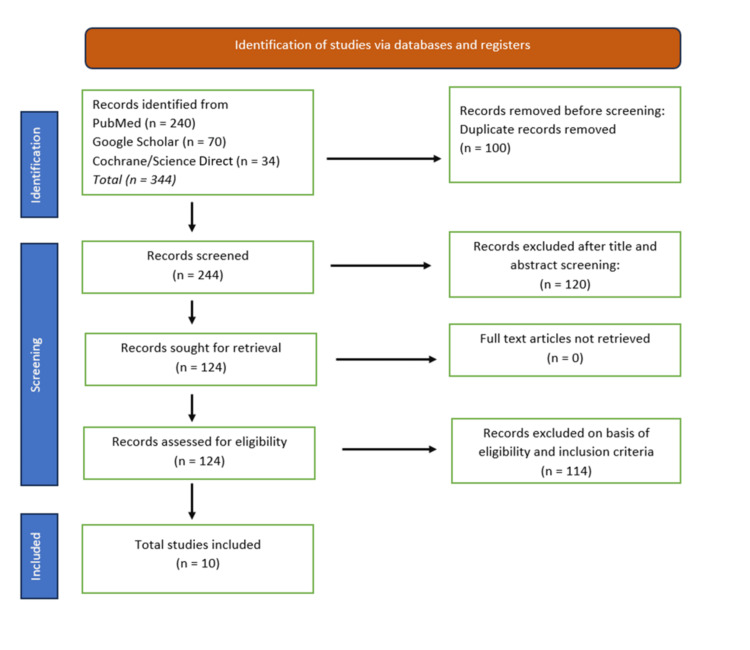 Figure 1
Figure 1| Study | Year | Country | Study type | Articles screened | Articles included | Epidemiology | Pharmacokinetics | Pharmacodynamics | CYP450 system effects | Acute side effects | Chronic side effects | Patient outcomes | Primary endpoint (PE) | Secondary endpoint (SE) | Conclusion |
| Teymouri et al. [ | 2024 | Iran | Systematic review | 4,512 | 143 | Increasing prevalence of ketamine-induced biliary disease, mostly in chronic users (avg. use 3-15 years). High risk in males and those with co-existing alcohol abuse | Hepatic metabolism, biliary excretion, delayed clearance in chronic users | NMDA-R antagonist also affects opioid and dopamine pathways. Long-term use linked to persistent LFT abnormalities | Chronic ketamine exposure leads to CYP3A4 and CYP2C9 upregulation, resulting in increased liver stress and cholestasis | GI distress, nausea, jaundice, and transient LFT elevation | Persistent biliary strictures, liver fibrosis, increased risk of cholangiocarcinoma (rare but reported) | Approximately 88% improved after stopping ketamine, 12% had persistent cholangiopathy requiring intervention | Characterizing biliary complications in ketamine abusers | Correlation between disease severity and duration of ketamine use | Ketamine-induced biliary dysfunction can persist even after drug cessation. Early diagnosis and intervention are crucial |
| Schep et al. [ | 2023 | New Zealand | Systematic review | 5,268 | 185 | Ketamine use is increasing, particularly in the dance/rave scene and among recreational drug users in the US, Europe, and Asia. High prevalence in young adults (18-35 years) | Rapid absorption, metabolized extensively in the liver by CYP enzymes, half-life 1.5-5 hours, primarily eliminated via kidneys | NMDA receptor antagonist, induces dissociative anesthesia, maintains respiratory drive, causes hallucinations at low doses | Metabolized by CYP2B6, CYP3A4, CYP2C9; converted to norketamine → hydroxynorketamine and dehydronorketamine; affecting metabolism and liver function | Hallucinations, dizziness, irrational behavior, vomiting, abdominal pain, tachycardia, hypertension | Cholangiopathy, cystitis, cognitive impairment, hepatobiliary dysfunction, recurrent GI issues, increased risk of depression | Variable: some improve with abstinence, others developed chronic liver or bladder damage | Characterize the toxicity, metabolism, and long-term effects of ketamine | Understand the role of CYP enzymes in ketamine metabolism and its impact on the hepatobiliary system | Ketamine induces liver and biliary dysfunction, affecting CYP metabolism. More research is needed on long-term effects and treatment strategies |
| Study | Year | Country | Study design | No. of patients | Mean age ± SD | Male (%) | Female (%) | Common symptoms | Imaging modality and findings | Significant findings | Primary endpoint (PE) | Secondary endpoint (SE) | Treatment | Outcome (% improved, worsened, recurrence) |
| Nyirenda et al. [ | 2020 | United Kingdom | Case report | 1 | 32 | 100% | 0% | Jaundice, cholangitis, rigors | MRCP: diffuse mural irregularity of bile ducts, recurrent cholangitis | Liver dysfunction progressed despite ketamine cessation | Effectiveness of biliary stenting in ketamine-induced cholangitis | Long-term outcomes after stenting | Biliary stenting, supportive care | 0% improved, 100% recurrence |
| Wong et al. [ | 2009 | Hong Kong | Case series | 3 | 24 ± 3 | 50% | 50% | Recurrent epigastric pain | US, CT, ERCP, MRCP: CBD dilation mimicking choledochal cyst | Symptoms correlated with ketamine use; ERCP showed smooth tapered CBD dilation | Relationship between ketamine abuse and CBD dilation | Effects of ketamine cessation on imaging findings | Nasobiliary drain, conservative | 67% improved, 33% recurrence |
| Garkusha et al. [ | 2024 | United States | Case series | 6 | 26 ± 6.2 | 50% | 50% | Abdominal pain, nausea, weight loss, urinary symptoms | US, MRCP, EUS: CBD dilation up to 17 mm, sclerosing cholangitis features | LFT abnormalities persisted in some cases | Identifying sclerosing cholangitis-like changes in ketamine users | Differences in disease progression between males and females | Supportive, ERCP, biliary drainage | 50% improved, 33% worsened, 17% recurrence |
| Pappachan et al. [ | 2014 | United Kingdom | Case report | 1 | 59 | 100% | 0% | Cachexia, hepatobiliary dysfunction, renal failure | US, CT, MRCP: Mild CBD dilation, hepatobiliary dysfunction, periportal hyperechogenicity | Multisystem involvement: GI, liver, kidney, cachexia | Multisystem effects of chronic ketamine abuse | Impact of nutritional status on recovery outcomes | Hydration, drug rehab | 100% improved |
| Yu et al. [ | 2014 | Hong Kong | Retrospective | 26 | 31 ± 4.1 | 42.30% | 57.70% | Abdominal pain | CT, MRCP: Fusiform CBD dilation (69%), non-dilated intrahepatic ducts | Severity of dilation correlated with duration of ketamine abuse | Prevalence of ketamine-related cholangiopathy | Reversibility of imaging findings with abstinence | Abstinence, supportive care | 73% improved, 27% worsened |
| Lo et al. [ | 2011 | United Kingdom | Case series | 3 | 27 ± 2.5 | 100% | 0% | Obstructive jaundice | US, MRCP, ERCP: Biliary dilatation up to 1.4 cm | Ketamine metabolite detected in urine; recurrent biliary symptoms post-exposure | Clinical course of ketamine-induced biliary obstruction | Effectiveness of ERCP in symptom relief | ERCP, stenting | 0% improved, 100% recurrence |
| Poon et al. [ | 2010 | Hong Kong | Retrospective | 37 | 25 ± 3.6 | 67.20% | 32.80% | Epigastric pain | Endoscopy: gastritis, normal endoscopy in some cases | Abstinence significantly associated with symptom relief (OR 12.5) | Association between ketamine use and upper GI symptoms | Effect of | Abstinence | 92% improved, 8% no improvement |
| Wong et al. [ | 2014 | Hong Kong | Cross-sectional | 297 | 25 ± 4 | 47% | 53% | Hepatobiliary dysfunction | MRCP, US, biopsy: CBD dilation, fibrosis, bile duct injury | 9.8% had liver injury; bile duct injury observed in all biopsied cases; 2 had bridging fibrosis | Histopathological features of ketamine-related liver injury | Gender differences in risk of fibrosis | Supportive, monitoring | 91% improved, 9% worsened |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTreatment of Major Depression · Diet and metabolism studies · Alcoholism and Thiamine Deficiency
Introduction and background
Ketamine is a glutamate N-methyl-D-aspartate receptor (NMDA-R) antagonist that has been clinically used since the 1960s, primarily as an anesthetic. Chemically, it consists of two enantiomers, R-ketamine and S-ketamine, the latter having a higher affinity to NMDA-R [1]. Ketamine is mostly administered intravenously, but it can also be administered subcutaneously, intramuscularly, transdermal, intranasally, intrarectally, or orally [2]. It acts primarily through glutamate modulation, affecting NMDA and AMPA receptors, and activating BDNF and mTOR signaling pathways [3]. Ketamine's unique pharmacology allows it to maintain cardiorespiratory stability while providing effective sedation and analgesia [4]. In recent years, ketamine has shown promise as a rapid-acting antidepressant, particularly for treatment-resistant depression and potentially for reducing suicidal ideation [3]. While ketamine has shown promise for its antidepressant effects and potential application in other areas, its widespread use remains limited due to side effects and risk of abuse [5,6]. Common acute effects include dissociation, nausea, dizziness, sedation, and cardiovascular stimulation [7,8]. Long-term use or high doses can lead to neurotoxicity, cognitive dysfunction, and uropathic effects [9]. The incidence and severity of these side effects can vary based on factors like age, gender, and dosage [10]. Among these adverse effects, ketamine’s impact on the hepatobiliary system is of particular concern, with reports of liver enzyme elevation and cholestasis [11]. Given the increasing use of ketamine in both clinical and nonclinical settings, understanding its potential hepatobiliary toxicity is crucial for patient safety and informed clinical decision-making. More studies are needed to explore such potential side effects as well as mitigation strategies to reduce side effects and increase tolerability. This literature review aims to evaluate the current evidence on ketamine-associated hepatobiliary side effects, focusing on their prevalence, underlying mechanisms, clinical presentations, and possible management strategies.
Review
Methods
A comprehensive literature search was conducted using multiple databases, including PubMed, Google Scholar, Science Direct, and Cochrane Library, to identify relevant studies on ketamine-associated hepatobiliary side effects. The search strategy employed keywords such as "ketamine", "hepatobiliary side effects", "liver injury", "cholestasis", and "liver enzymes" to capture all potential articles. The initial search yielded 344 articles. These were screened based on their titles and abstracts, and after applying the inclusion and exclusion criteria, 10 articles were selected for full-text review and inclusion in the final analysis. The selected articles were reviewed to assess the limitations reported by the authors. A narrative synthesis approach was used to analyze and summarize the findings from the selected studies, with an emphasis on identifying patterns, prevalence, mechanisms, and clinical implications of ketamine-induced hepatobiliary side effects. The complete search strategy and selection of studies are depicted in the research flowchart shown in Figure 1.
Flowchart depicting the study selection process for the scoping review
Eligibility Criteria
The inclusion criteria for this review focused on studies involving human subjects to ensure direct clinical relevance, specifically targeting articles that examined hepatobiliary side effects or hepatotoxicity associated with ketamine use, including liver enzyme elevation, cholestasis, biliary tract abnormalities, or liver failure. Only original research articles, case reports, case series, clinical trials, cohort studies, and retrospective analyses were considered, provided they were peer-reviewed to uphold a high standard of scientific rigor. Additionally, studies had to be published in English to maintain accessibility and consistency in data interpretation. Conversely, the exclusion criteria eliminated studies involving nonhuman subjects, unless they provided significant mechanistic insights applicable to humans. Research not specifically addressing hepatobiliary side effects or hepatotoxicity related to ketamine use was excluded, along with studies involving multi-drug-induced injuries or polypharmacy, where the role of ketamine could not be isolated. Reviews, editorials, opinion pieces, and studies lacking original data or quantitative analysis were also excluded. Furthermore, studies with insufficient data, unclear methodologies, or non-peer-reviewed sources were not included, and articles in languages other than English were excluded to prevent translation bias and ensure consistent interpretation of results.
Results
Our literature indicates that a growing body of evidence suggests that ketamine, while therapeutically valuable, poses risks of significant hepatobiliary complications. The studies reviewed highlight various aspects of ketamine-associated liver and biliary tract injuries, shedding light on the clinical manifestations, underlying mechanisms, and potential outcomes. A systematic review comprehensively examined 11 cases of ketamine-associated biliary disease, providing one of the most robust assessments of this issue to date [12]. The cases primarily involved young males, with a mean age of 25 years, and the median duration of ketamine abuse was 24 months. The most common clinical presentation was abdominal pain in 71% of patients, often accompanied by elevated liver enzymes and biliary tract abnormalities. Expanding on these clinical presentations, a compelling case study described a middle-aged man with chronic ketamine abuse, presenting with persistent cholangiopathy [13]. The patient experienced recurrent abdominal pain, jaundice, and abnormal liver function tests. Imaging revealed bile duct strictures, and despite initial conservative treatments, the patient ultimately required endoscopic retrograde cholangiopancreatography (ERCP) and stenting to manage recurring cholangitis. Further extending the temporal scope of research, a systematic review covering studies from 1950 to 2023 identified 185 articles linking chronic ketamine use to a wide array of side effects, including impaired verbal processing, cystitis, and cholangiopathy [14]. The review emphasized the prevalence of gastrointestinal (GI) symptoms, particularly abdominal pain and vomiting, in patients with ketamine-associated cholangiopathy, reinforcing the notion that ketamine can trigger substantial hepatobiliary dysfunction, often resembling GI pathologies. Wong et al. provided further clinical insight through a case series documenting three patients with over a year of ketamine abuse [15]. These patients presented with a combination of urinary symptoms and cholestasis, along with fusiform dilation of the bile duct, which mimicked the appearance of a choledochal cyst. These rare presentations emphasize the diverse clinical manifestations of ketamine toxicity, which may extend beyond typical hepatobiliary symptoms. Building on these findings, a case series documented six young adults with chronic ketamine use, all of whom developed severe cholestasis and cholangiopathy [16]. These patients presented with abdominal pain and biliary duct dilation suggestive of sclerosing cholangitis. Another individual case report discussed that a patient’s alkaline phosphatase, gamma-glutamyl transferase, and alanine transaminase levels were significantly elevated at 970 IU/L, 1796 IU/L, and 46 IU/L, respectively, during the acute phase of ketamine abuse [17]. However, these values decreased to near-normal levels after 60 days of abstinence and appropriate medical management, demonstrating the potential for biochemical recovery once ketamine use ceases. Further supporting the link between ketamine use and biliary damage, Yu et al. reported fusiform dilation of the common bile duct (CBD) with smooth distal tapering as the most common imaging feature in ketamine-induced cholangiopathy [18]. These radiologic findings are pivotal for clinicians, as they provide diagnostic confirmation for identifying ketamine-related biliary abnormalities. Another noteworthy study described three young males with chronic ketamine use, each presenting with cholestasis and biliary tract abnormalities [19]. This study highlighted fluctuating liver function and dilated biliary systems on CT imaging, with one patient exhibiting elevated bilirubin levels exceeding 3 µmol/L. This fluctuation in liver biochemistry underscores that ketamine-related liver dysfunction can be of an episodic nature as well. In addition to these individual case reports and series, a retrospective study involving 37 chronic ketamine users revealed that 73% of participants experienced upper GI symptoms, predominantly epigastric pain [20]. Endoscopic evaluations showed that 85.7% of these patients had gastritis. Interestingly, the cessation of ketamine use led to a significant improvement in symptoms, with a p-value of 0.027 and an odds ratio (OR) of 12.5 (95% CI 1.20, 130.6), indicating a strong association between ketamine cessation and symptom relief. A cross-sectional survey of 297 chronic ketamine abusers with urinary tract dysfunction identified liver injury in 9.8% of the cases, all of which were classified as cholestatic [21]. Liver biopsies performed on seven patients revealed bile duct injury, and in two cases, there was evidence of bridging fibrosis. Additionally, imaging of six patients indicated CBD dilation in three cases, though no obstructions were found. This large-scale study adds further weight to the link between chronic ketamine use and liver injury, particularly in the context of co-occurring urinary tract dysfunction. The results of the systematic reviews are summarized in Table 1, while the findings from other studies are compiled in Table 2.
Discussion
Our literature review highlights that while ketamine is beneficial for pain management, sedation, and emerging treatments in psychiatric conditions, it is also associated with significant hepatobiliary side effects. The evidence collected underscores a range of hepatobiliary issues linked to ketamine use, including cholestasis, biliary duct abnormalities, and liver enzyme elevations. Understanding the pathophysiology of ketamine-induced liver and hepatobiliary injury is crucial, as it will serve as the cornerstone for developing future guidelines for treatment, prevention, and safer use of ketamine in clinical settings. The exact mechanisms of ketamine-induced hepatobiliary injury remain unknown, though several hypotheses exist in the literature. One prevailing hypothesis is that ketamine influences the activity of NMDA ionotropic receptors located on smooth muscle in the biliary tract [22]. It has been postulated that ketamine abuse leads to bile duct injury, cholestasis, and CBD dilation, either through a direct effect on biliary smooth muscle or via central actions [23]. Another potential mechanism involves the disruption of gallbladder motility through central pathways [24]. Additionally, ketamine has been found to induce oxidative stress and apoptosis in hepatocytes, further contributing to hepatic damage [25]. Since ketamine is metabolized by the cytochrome P450 system in the liver and excreted in bile and urine, direct toxic injury to the surface epithelium has also been suggested as a plausible mechanism [13]. The association between elevated C-reactive protein levels and abnormal liver biochemistry suggests that a chronic inflammatory process may play a role. However, despite the presence of multiple hypotheses, it is clear that research in this area is limited. Expanding research on ketamine's effects on other organs, such as the urinary tract, could also provide valuable insights into the biochemical mechanisms behind its hepatobiliary toxicity. The clinical implications of ketamine-induced liver injury emphasize the need for comprehensive liver assessments in patients using ketamine, whether for recreational, medical, or surgical purposes. Managing ketamine-induced hepatobiliary damage effectively requires a multifaceted approach that addresses both the immediate and long-term consequences of liver injury. In the acute phase, immediate cessation of ketamine is essential to prevent further hepatic damage. Supportive care, including fluid administration, electrolyte replacement, and close monitoring of liver function, plays a vital role in stabilizing the patient's condition. For patients with more severe or persistent liver damage, pharmacological interventions may be necessary. Ursodeoxycholic acid, a bile acid that improves bile flow and reduces inflammation, has shown potential in managing ketamine-induced cholestatic liver injury [25]. In addition to pharmacological treatments, lifestyle modifications and strict adherence to abstinence from ketamine are critical for long-term management. Educating patients about the importance of a healthy diet, avoiding alcohol and other hepatotoxic substances, and maintaining a regular exercise routine can support liver regeneration and overall health [26]. In conclusion, ketamine abuse can lead to a range of liver injuries, from CBD dilation to bile duct damage and even significant liver fibrosis. Further research is necessary to explore the natural history, underlying mechanisms, and potential therapeutic targets for ketamine-induced hepatobiliary injuries.
Limitations
This review has several limitations, including a limited number of studies that restrict the generalizability of findings and significant heterogeneity in study designs, patient populations, and reported outcomes, which complicates comparisons. The reliance on case reports and series introduces potential biases and may not fully represent the range of ketamine's hepatobiliary effects. The exclusion of non-English language studies and lack of long-term follow-up data may result in an incomplete understanding of ketamine's impact on the liver. Additionally, confounding factors such as polypharmacy and pre-existing liver conditions were not consistently accounted for, potentially affecting the interpretation of the results.
Conclusions
This review underscores the potential for significant hepatobiliary toxicity associated with ketamine use, ranging from mild liver enzyme elevation to severe cholestasis and biliary tract abnormalities. While ketamine's therapeutic benefits are notable, its safety profile requires careful consideration. The findings suggest a need for further research to clarify the underlying mechanisms, establish risk factors, and develop strategies to mitigate adverse effects. Clinicians should remain vigilant in monitoring liver function in patients receiving ketamine, ensuring informed decision-making and safe clinical use.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ketamine pharmacology: an update (pharmacodynamics and molecular aspects, recent findings)CNS Neurosci Ther Mion G Villevieille T 3703801920132357543710.1111/cns.12099 PMC 6493357 · doi ↗ · pubmed ↗
- 2Ketamine's mechanism of action: a path to rapid-acting antidepressants Depress Anxiety Abdallah CG Adams TG Kelmendi B Esterlis I Sanacora G Krystal JH 6896973320162706230210.1002/da.22501 PMC 4961540 · doi ↗ · pubmed ↗
- 3Ketamine as an antidepressant: overview of its mechanisms of action and potential predictive biomarkers Ther Adv Psychopharmacol Matveychuk D Thomas RK Swainson J Khullar A Mac Kay MA Baker GB Dursun SM 20451253209166571020203244033310.1177/2045125320916657 PMC 7225830 · doi ↗ · pubmed ↗
- 4Ketamine: 50 years of modulating the mind Front Hum Neurosci Li L Vlisides PE 6121020162796556010.3389/fnhum.2016.00612 PMC 5126726 · doi ↗ · pubmed ↗
- 5A Survey of the Clinical, Off-Label Use of Ketamine as a Treatment for Psychiatric Disorders Am J Psychiatry Wilkinson ST Toprak M Turner MS Levine SP Katz RB Sanacora G 69569617420172866920210.1176/appi.ajp.2017.17020239 PMC 5549850 · doi ↗ · pubmed ↗
- 6Mechanisms of ketamine action as an antidepressant Mol Psychiatry Zanos P Gould TD 8018112320182953279110.1038/mp.2017.255PMC 5999402 · doi ↗ · pubmed ↗
- 7Ketamine for chronic pain: risks and benefits Br J Clin Pharmacol Niesters M Martini C Dahan A 3573677720142343238410.1111/bcp.12094 PMC 4014022 · doi ↗ · pubmed ↗
- 8Long-term safety of ketamine and esketamine in treatment of depression Expert Opin Drug Saf Nikayin S Murphy E Krystal JH Wilkinson ST 7777872120223541610510.1080/14740338.2022.2066651 · doi ↗ · pubmed ↗