Efficacy and Safety of Direct Oral Anticoagulants Versus Vitamin K Antagonists for Left Ventricular Thrombus: A Systematic Review and Meta-Analysis
Momina Khan, Kinnari Patel, Given E Edim, Maryam Mazhar, Hafiza Zanish Iram, Sandipkumar S Chaudhari, Calvin R Wei, Areeba Khan

TL;DR
This study compares the effectiveness and safety of new blood thinners (DOACs) to older ones (VKAs) for treating heart clots, finding similar effectiveness but fewer bleeding risks with DOACs.
Contribution
The study provides a meta-analysis showing DOACs are as effective as VKAs for left ventricular thrombus resolution with reduced bleeding risk.
Findings
DOACs and VKAs showed comparable efficacy in resolving left ventricular thrombus.
DOACs were associated with significantly lower bleeding risk compared to VKAs.
Subgroup analyses confirmed consistent results across study designs.
Abstract
Left ventricular thrombus (LVT) is a serious complication associated with myocardial infarction and cardiomyopathy. While vitamin K antagonists (VKAs) have been the standard treatment, direct oral anticoagulants (DOACs) offer potential advantages. This meta-analysis compares the efficacy and safety of DOACs versus VKAs in patients with LVT. We conducted a systematic search of PubMed, Excerpta Medica database (Embase), Scopus, Web of Science, and Cochrane Central Register of Controlled Trials (CENTRAL) from inception to April 2025. Studies comparing DOACs with VKAs in adult patients with LVT were included. The primary outcome was LVT resolution; secondary outcomes included stroke or systemic embolism (SSE) and bleeding events. Random-effects models were used to calculate pooled risk ratios (RRs) with 95% confidence intervals. Thirty-five studies (five RCTs and 30 observational) with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
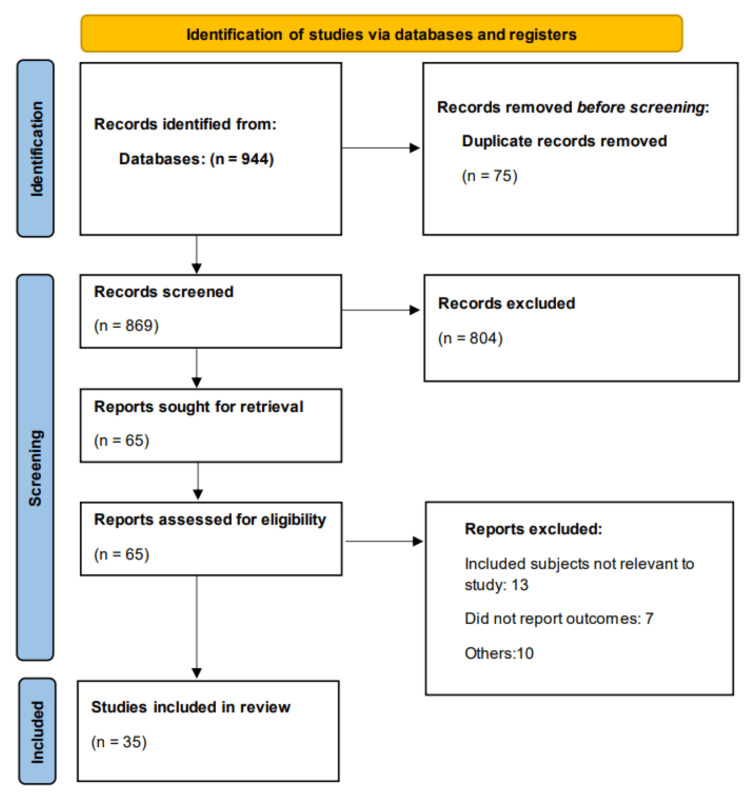 Figure 1
Figure 1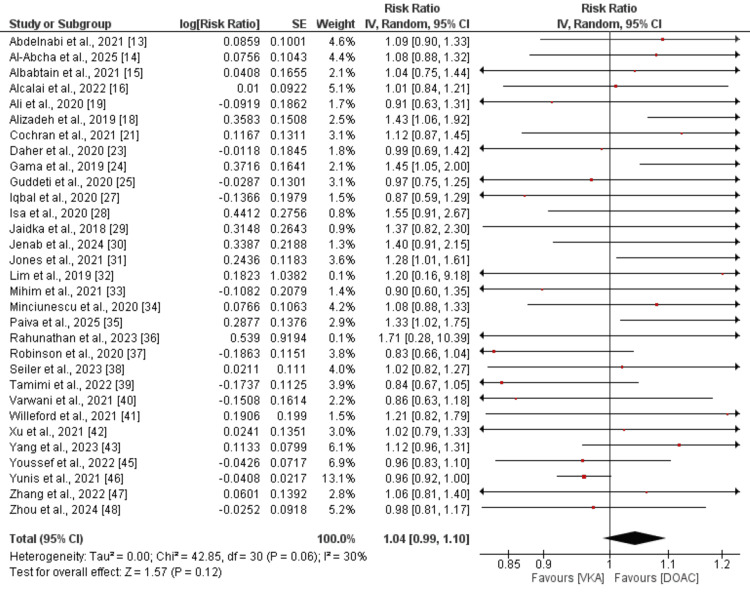 Figure 2
Figure 2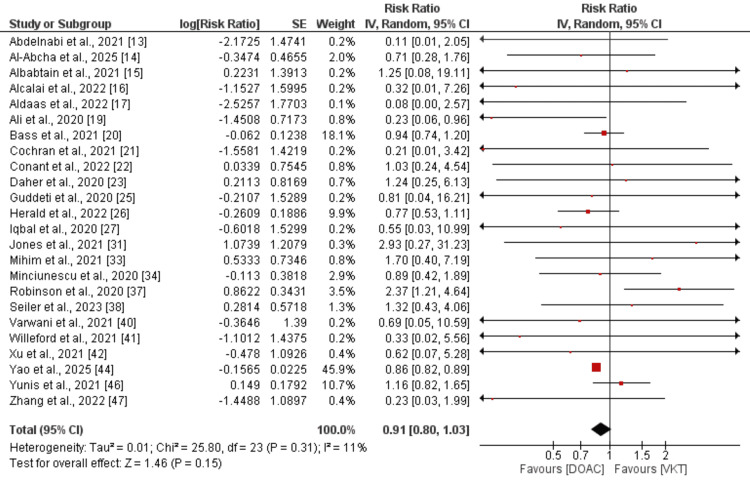 Figure 3
Figure 3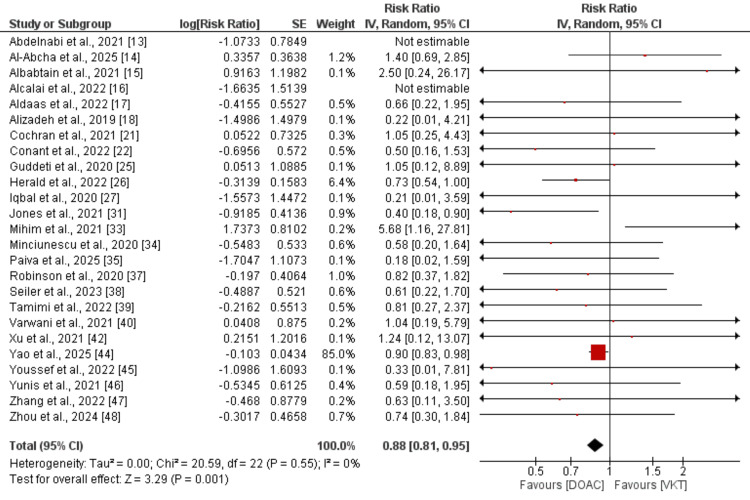 Figure 4
Figure 4| Author | Year | Region | Study Design | Groups | Sample Size | Type of DOAC | Follow-up Duration |
| Abdelnabi et al. [ | 2021 | Africa | RCT | DOAC | 39 | Rivaroxaban | 6 Months |
| VKA | 40 | ||||||
| Al-Abcha et al. [ | 2025 | United States | Retrospective Observational | DOAC | 46 | Apixaban, rivaroxaban, dabigatran, or edoxaban | NR |
| VKA | 143 | ||||||
| Albabtain et al. [ | 2021 | Saudi Arabia | Retrospective Observational | DOAC | 28 | Rivaroxaban | 9.5 Months |
| VKA | 35 | ||||||
| Alcalai et al. [ | 2022 | Israel | RCT | DOAC | 18 | Apixaban | 3 Months |
| VKA | 17 | ||||||
| Aldaas et al. [ | 2022 | United States | Retrospective Observational | DOAC | 75 | NR | 10.0 Months |
| VKA | 142 | ||||||
| Alizadeh et al. [ | 2019 | United Kingdom | Prospective Observational | DOAC | 38 | Apixaban, rivaroxaban, or edoxaban | 21.6 Months |
| VKA | 60 | ||||||
| Ali et al. [ | 2020 | United States | Retrospective Observational | DOAC | 32 | Apixaban, rivaroxaban and dabogatran | 12 Months |
| VKA | 60 | ||||||
| Bass et al. [ | 2021 | United States | Retrospective Observational | DOAC | 180 | Apixaban, rivaroxaban and dabogatran | 3 Months |
| VKA | 769 | ||||||
| Cochran et al. [ | 2021 | United States | Retrospective Observational | DOAC | 14 | Apixaban, rivaroxaban, dabigatran, or edoxaban | 12 Months |
| VKA | 59 | ||||||
| Conant et al. [ | 2022 | United States | Retrospective Observational | DOAC | 29 | NR | NR |
| VKA | 135 | ||||||
| Daher et al. [ | 2020 | France | Retrospective Observational | DOAC | 17 | Apixaban, rivaroxaban and dabogatran | 64.8 Months |
| VKA | 42 | ||||||
| Gama et al. [ | 2019 | Portugal | Retrospective Observational | DOAC | 12 | NR | 6 Months |
| VKA | 52 | ||||||
| Guddeti et al. [ | 2020 | United States | Retrospective Observational | DOAC | 19 | Apixaban, rivaroxaban and dabogatran | 10.4 Months |
| VKA | 80 | ||||||
| Herald et al. [ | 2022 | United States | Retrospective Observational | DOAC | 134 | Apixaban, rivaroxaban, dabigatran, or edoxaban | 40.8 Months |
| VKA | 299 | ||||||
| Iqbal et al. [ | 2020 | United Kingdom | Retrospective Observational | DOAC | 22 | NR | 36 Months |
| VKA | 62 | ||||||
| Isa et al. [ | 2020 | Malaysia | RCT | DOAC | 14 | Apixaban | 3 Months |
| VKA | 13 | ||||||
| Jaidka et al. [ | 2018 | United Kingdom | Retrospective Observational | DOAC | 12 | Apixaban, rivaroxaban and dabogatran | 6 Months |
| VKA | 37 | ||||||
| Jenab et al. [ | 2025 | Iran | RCT | DOAC | 26 | Rivaroxaban | 3 Months |
| VKA | 24 | ||||||
| Jones et al. [ | 2021 | United Kingdom | Retrospective Observational | DOAC | 41 | Apixaban, rivaroxaban, or edoxaban | 26.4 Months |
| VKA | 60 | ||||||
| Lim et al. [ | 2019 | Malaysia | Retrospective Observational | DOAC | 5 | NR | 24 Months |
| VKA | 18 | ||||||
| Mihim et al. [ | 2021 | United States | Retrospective Observational | DOAC | 33 | Apixaban, rivaroxaban, dabigatran, or edoxaban | 6 Months |
| VKA | 75 | ||||||
| Minciunescu et al. [ | 2020 | United States | Retrospective Observational | DOAC | 57 | NR | NR |
| VKA | 140 | ||||||
| Paiva et al. [ | 2025 | Portugal | Retrospective Observational | DOAC | 99 | Apixaban, rivaroxaban, dabigatran, or edoxaban | 24 Months |
| VKA | 72 | ||||||
| Rahunathan et al. [ | 2023 | United Kingdom | Retrospective Observational | DOAC | 14 | NR | 4.66 Months |
| VKA | 4 | ||||||
| Robinson et al. [ | 2020 | United States | Retrospective Observational | DOAC | 121 | Apixaban | 11.7 Months |
| VKA | 236 | ||||||
| Seiler et al. [ | 2023 | Switzerland | Retrospective Observational | DOAC | 48 | Apixaban and Rivaroxaban | 31.3 Months |
| VKA | 53 | ||||||
| Tamimi et al. [ | 2022 | United States | Retrospective Observational | DOAC | 48 | Apixaban, rivaroxaban, or edoxaban | 6 Months |
| VKA | 116 | ||||||
| Varwani et al. [ | 2021 | Kenya | Retrospective Observational | DOAC | 36 | Apixaban, rivaroxaban and dabogatran | 12 Months |
| VKA | 25 | ||||||
| Willeford et al. [ | 2021 | United States | Retrospective Observational | DOAC | 22 | Apixaban, rivaroxaban, dabigatran, or edoxaban | 8.5 Months |
| VKA | 129 | ||||||
| Xu et al. [ | 2021 | China | Retrospective Observational | DOAC | 25 | Dabigatran and rivaroxaban | 28.44 Months |
| VKA | 62 | ||||||
| Yang et al. [ | 2023 | China | Retrospective Observational | DOAC | 91 | NR | 3 Months |
| VKA | 33 | ||||||
| Yao et al. [ | 2025 | United Kingdom | Retrospective Observational | DOAC | 19885 | Apixaban, rivaroxaban, dabigatran, or edoxaban | 3 Months |
| VKA | 19885 | ||||||
| Youssef et al. [ | 2023 | Saudi Arabia | RCT | DOAC | 25 | Apixaban | 6 Months |
| VKA | 25 | ||||||
| Yunis et al. [ | 2020 | United States | Retrospective Observational | DOAC | 64 | NR | 24 Months |
| VKA | 200 | ||||||
| Zhang et al. [ | 2022 | China | Retrospective Observational | DOAC | 33 | Rivaroxaban | 8.5 Months |
| VKA | 31 | ||||||
| Zhou et al. [ | 2024 | China | Retrospective Observational | DOAC | 111 | Apixaban, rivaroxaban and dabogatran | 6 Months |
| VKA | 129 |
| Author ID | Groups | Total Population | Mean Age (Years) | Female (n) | Diabetes (n) | Hypertension (n) |
| Abdelnabi et al., 2021 [ | DOAC | 39 | NR | NR | NR | NR |
| VKA | 40 | |||||
| Al-Abcha et al., 2025 [ | DOAC | 46 | 62.8 | 9 | 15 | 31 |
| VKA | 143 | 60.8 | 38 | 49 | 100 | |
| Albabtain et al., 2021 [ | DOAC | 28 | 58.25 | 4 | 12 | 13 |
| VKA | 35 | 59 | 1 | 16 | 19 | |
| Alcalai et al., 2022 [ | DOAC | 18 | 55.2 | 5 | 8 | 7 |
| VKA | 17 | 58.8 | 2 | 5 | 7 | |
| Aldaas et al., 2022 [ | DOAC | 75 | NR | NR | NR | NR |
| VKA | 142 | |||||
| Alizadeh et al., 2019 [ | DOAC | 38 | NR | NR | NR | NR |
| VKA | 60 | |||||
| Ali et al., 2020 [ | DOAC | 32 | 59.2 | 6 | 12 | NR |
| VKA | 60 | 58 | 11 | 18 | ||
| Bass et al., 2021 [ | DOAC | 180 | 63.4 | 55 | NR | NR |
| VKA | 769 | 61.6 | 224 | |||
| Cochran et al., 2021 [ | DOAC | 15 | 51.5 | 3 | 7 | NR |
| VKA | 59 | 62 | 14 | 23 | ||
| Conant et al., 2022 [ | DOAC | 29 | NR | NR | NR | NR |
| VKA | 135 | |||||
| Daher et al., 2020 [ | DOAC | 17 | 57 | 3 | 2 | 10 |
| VKA | 42 | 61 | 7 | 9 | 17 | |
| Gama et al., 2019 [ | DOAC | 12 | NR | NR | NR | NR |
| VKA | 52 | |||||
| Guddeti et al., 2020 [ | DOAC | 19 | 60.7 | 4 | NR | NR |
| VKA | 80 | 61.3 | 25 | |||
| Herald et al., 2022 [ | DOAC | 134 | 66 | 18 | 45 | 90 |
| VKA | 299 | 65 | 57 | 124 | 217 | |
| Iqbal et al., 2020 [ | DOAC | 22 | 62 | 2 | 19 | 9 |
| VKA | 62 | 62 | 7 | 19 | 18 | |
| Isa et al., 2020 [ | DOAC | 14 | 55.36 | 1 | 7 | 8 |
| VKA | 13 | 55 | 1 | 9 | 9 | |
| Jaidka et al., 2018 [ | DOAC | 12 | 57.2 | 3 | 1 | 2 |
| VKA | 37 | 61.3 | 9 | 7 | 18 | |
| Jenab et al., 2025 [ | DOAC | 26 | 55 | 4 | 7 | 9 |
| VKA | 24 | 55 | 5 | 5 | 14 | |
| Jones et al., 2021 [ | DOAC | 41 | 58.73 | 8 | 7 | 23 |
| VKA | 60 | 60.81 | 9 | 10 | 22 | |
| Lim et al., 2019 [ | DOAC | 5 | NR | NR | NR | NR |
| VKA | 18 | |||||
| Mihim et al., 2021 [ | DOAC | 33 | 63.3 | 10 | 8 | 24 |
| VKA | 75 | 60.3 | 21 | 20 | 56 | |
| Minciunescu et al., 2020 [ | DOAC | 57 | 60.4 | 11 | 15 | 46 |
| VKA | 140 | 59.5 | 34 | 39 | 97 | |
| Paiva et al., 2025 [ | DOAC | 99 | 55.4 | 13 | 20 | 47 |
| VKA | 72 | 65.9 | 17 | 10 | 67 | |
| Rahunathan et al., 2023 [ | DOAC | 14 | 58.5 | 2 | 3 | 4 |
| VKA | 4 | 63.5 | 1 | 1 | 0 | |
| Robinson et al., 2020 [ | DOAC | 121 | 58.1 | 27 | 36 | 86 |
| VKA | 236 | 58.2 | 66 | 92 | 177 | |
| Seiler et al., 2023 [ | DOAC | 48 | 64.3 | 6 | 8 | 24 |
| VKA | 53 | 62.2 | 12 | 11 | 31 | |
| Tamimi et al., 2022 [ | DOAC | 48 | NR | NR | NR | NR |
| VKA | 116 | |||||
| Varwani et al., 2021 [ | DOAC | 36 | NR | NR | NR | NR |
| VKA | 25 | |||||
| Willeford et al., 2021 [ | DOAC | 22 | 54 | 5 | 4 | 8 |
| VKA | 129 | 56 | 25 | 37 | 54 | |
| Xu et al., 2021 [ | DOAC | 25 | 59.4 | 6 | 6 | 10 |
| VKA | 62 | 61.9 | 15 | 12 | 27 | |
| Yang et al., 2023 [ | DOAC | 91 | NR | NR | NR | NR |
| VKA | 33 | |||||
| Yao et al., 2025 [ | DOAC | 19885 | 61.8 | 6320 | 7575 | 14983 |
| VKA | 19885 | 61.6 | 6310 | 7560 | 14997 | |
| Youssef et al., 2023 [ | DOAC | 25 | 52 | NR | 12 | 11 |
| VKA | 25 | 53 | 11 | 10 | ||
| Yunis et al., 2020 [ | DOAC | 64 | NR | NR | NR | NR |
| VKA | 200 | |||||
| Zhang et al., 2022 [ | DOAC | 33 | 60.3 | 9 | 10 | 23 |
| VKA | 31 | 61.3 | 8 | 5 | 11 | |
| Zhou et al., 2024 [ | DOAC | 111 | 56 | 19 | 41 | 48 |
| VKA | 129 | 55 | 10 | 46 | 63 |
| Author ID | Selection | Comparison | Assessment | Overall Grade |
| Al-Abcha et al., 2025 [ | 4 | 1 | 3 | Good |
| Albabtain et al., 2021 [ | 4 | 1 | 2 | Good |
| Aldaas et al., 2022 [ | 3 | 0 | 2 | Fair |
| Alizadeh et al., 2019 [ | 3 | 0 | 3 | Fair |
| Ali et al., 2020 [ | 3 | 0 | 2 | Good |
| Bass et al., 2021 [ | 3 | 1 | 2 | Fair |
| Cochran et al., 2021 [ | 3 | 1 | 3 | Good |
| Conant et al., 2022 [ | 3 | 2 | 2 | Good |
| Daher et al., 2020 [ | 3 | 1 | 3 | Good |
| Gama et al., 2019 [ | 3 | 1 | 2 | Good |
| Guddeti et al., 2020 [ | 3 | 2 | 3 | Good |
| Herald et al., 2022 [ | 3 | 1 | 3 | Good |
| Iqbal et al., 2020 [ | 3 | 2 | 3 | Good |
| Jaidka et al., 2018 [ | 3 | 0 | 3 | Fair |
| Jones et al., 2021 [ | 3 | 1 | 3 | Good |
| Lim et al., 2019 [ | 3 | 0 | 2 | Good |
| Mihim et al., 2021 [ | 3 | 1 | 3 | Good |
| Minciunescu et al., 2020 [ | 3 | 1 | 2 | Fair |
| Paiva et al., 2025 [ | 4 | 2 | 3 | Good |
| Rahunathan et al., 2023 [ | 3 | 1 | 3 | Good |
| Robinson et al., 2020 [ | 3 | 1 | 3 | Good |
| Seiler et al., 2023 [ | 4 | 1 | 3 | Good |
| Tamimi et al., 2022 [ | 2 | 0 | 2 | Poor |
| Varwani et al., 2021 [ | 3 | 1 | 3 | Good |
| Willeford et al., 2021 [ | 3 | 1 | 3 | Good |
| Xu et al., 2021 [ | 3 | 0 | 3 | Fair |
| Yang et al., 2023 [ | 4 | 1 | 3 | Good |
| Yao et al., 2025 [ | 4 | 1 | 3 | Good |
| Yunis et al., 2020 [ | 3 | 0 | 2 | Fair |
| Zhang et al., 2022 [ | 3 | 1 | 3 | Good |
| Zhou et al., 2024 [ | 3 | 1 | 2 | Fair |
| Outcomes | Subgroups | RR (95% CI) | I-Square |
| LVT Resoultion | RCT | 1.05 (0.93 to 1.19) | 19% |
| Observational | 1.04 (0.98 to 1.10) | 22% | |
| Stroke | RCT | 0.18 (0.02 to 1.52) | 0% |
| Observational | 0.91 (0.80 to 1.03) | 6% | |
| Bleeding Events | RCT | 0.31 (0.09 to 1.07) | 0% |
| Observational | 0.88 (0.81 to 0.95) | 0% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAtrial Fibrillation Management and Outcomes · Cardiac tumors and thrombi · Cardiac Arrhythmias and Treatments
Introduction and background
Left ventricular thrombus (LVT) is a serious and potentially life-threatening complication commonly associated with conditions such as anterior myocardial infarction, heart failure with reduced ejection fraction, and non-ischemic cardiomyopathy [1,2]. The formation of a thrombus in the left ventricle predisposes patients to systemic embolization, including stroke, and therefore mandates timely and effective anticoagulation therapy [3]. Traditionally, vitamin K antagonists (VKAs), such as warfarin, have been the cornerstone of treatment for LVT due to their established efficacy in thrombus resolution and prevention of thromboembolic events [4]. However, VKAs require regular monitoring, have a narrow therapeutic index, and are associated with multiple drug and dietary interactions, which limit their utility in real-world clinical practice [5].
Anticoagulation is critical in preventing devastating complications of LVT, particularly ischemic stroke and peripheral embolism [2]. Recent interest has focused on direct oral anticoagulants (DOACs) as potential alternatives to VKAs, given their predictable pharmacokinetics, fixed dosing, and fewer interactions [4]. Despite these advantages, the evidence supporting DOAC use in LVT remains limited and evolving. Current guidelines, such as those from the American College of Cardiology and the European Society of Cardiology, continue to recommend VKAs as the standard of care, highlighting the need for robust comparative data to inform clinical decision-making [6].
In recent years, DOACs, including agents such as apixaban, rivaroxaban, dabigatran, and edoxaban, have emerged as alternatives to VKAs in various thromboembolic conditions, including atrial fibrillation and venous thromboembolism [6]. DOACs offer several advantages over VKAs, including fixed dosing, fewer drug-food interactions, and no need for routine coagulation monitoring. These benefits have led to growing interest in their potential role in the management of LVT [7]. Despite the increasing off-label use of DOACs for LVT, current international guidelines remain cautious, citing limited high-quality evidence to support their routine use in this indication.
VKAs exert their anticoagulant effect by inhibiting the enzyme vitamin K epoxide reductase, which is essential for the post-translational carboxylation of clotting factors II, VII, IX, and X [8]. This inhibition reduces the synthesis of these vitamin K-dependent coagulation factors, thereby impairing thrombin generation and clot formation [8]. In contrast, DOACs provide targeted inhibition of key components in the coagulation cascade. Dabigatran directly inhibits thrombin (factor IIa), while apixaban, rivaroxaban, and edoxaban selectively inhibit activated factor X (Xa) [9]. By directly targeting specific coagulation factors, DOACs offer a more predictable pharmacological profile, fewer interactions, and rapid onset of action, eliminating the need for routine coagulation monitoring [10]. These pharmacologic differences have raised the question of whether DOACs can serve as a reliable alternative to VKAs for indications such as LVT.
To date, few comprehensive meta-analyses have assessed the comparative effectiveness and safety of DOACs versus VKAs specifically for LVT [11,12]. New studies have been conducted since then. Given the clinical importance of preventing systemic embolism while minimizing bleeding complications, a better understanding of the relative benefits and risks of these agents in this population is urgently needed through analyzing recent evidence. Therefore, the aim of this systematic review and meta-analysis is to evaluate and compare the efficacy of DOACs and VKAs in achieving LVT resolution, as well as their impact on stroke prevention and bleeding events.
Review
Methodology
Literature Search and Search Strategy
A comprehensive literature search was conducted to identify all relevant studies comparing direct oral anticoagulants (DOACs) with vitamin K antagonists (VKAs) in the treatment of left ventricular thrombus (LVT). We systematically searched PubMed, Excerpta Medica database (Embase), Scopus, Web of Science, and the Cochrane Central Register of Controlled Trials (CENTRAL) from inception to 10 April 2025. The search strategy included combinations of keywords and Medical Subject Headings (MeSH) related to “left ventricular thrombus,” “LVT,” “direct oral anticoagulants,” “DOACs,” “non-vitamin K oral anticoagulants,” “NOACs,” “apixaban,” “rivaroxaban,” “dabigatran,” “edoxaban,” and “warfarin.” Boolean operators (AND, OR) were used to optimize the search sensitivity. Reference lists of relevant reviews and eligible studies were also manually screened for additional studies. All search and screening steps were independently performed by two reviewers. Discrepancies were resolved through discussion or in consultation with a third reviewer.
Study Selection
All identified citations were imported into EndNote (Clarivate Plc, PA, USA) for deduplication. Two reviewers independently screened titles and abstracts for eligibility. Full-text articles of potentially relevant studies were then assessed to determine inclusion. Studies were included if they enrolled adult patients (≥18 years) with a diagnosis of LVT, compared DOACs with VKAs, and reported at least one of the following outcomes: LVT resolution, stroke, or bleeding events. Both randomized controlled trials (RCTs) and observational studies were considered. Exclusion criteria included case reports, reviews, editorials, conference abstracts without full data, and studies lacking comparative outcome data. Any disagreement between the reviewers regarding eligibility was resolved by consensus or discussion with a third reviewer.
Data Extraction and Outcomes
Two reviewers independently extracted data using a standardized data collection form. Extracted information included study characteristics (author, publication year, country, study design), patient demographics (sample size, mean age, proportion of females), clinical features (presence of diabetes, hypertension), details of anticoagulant treatment, and length of follow-up. Outcomes of interest included LVT resolution (primary outcome), stroke, and bleeding events (secondary outcomes), as defined by each study. Both adjusted and unadjusted effect estimates (RRs, ORs, HRs) along with 95% confidence intervals (CIs) were extracted. Where effect estimates were not reported, they were calculated from raw data when available. Disagreements in data extraction were resolved by discussion between the reviewers or by involving a third reviewer.
Statistical Analysis
Statistical analyses were performed using random-effects models (DerSimonian and Laird method) to account for potential heterogeneity among studies. Pooled risk ratios (RRs) with 95% CIs were calculated for dichotomous outcomes. A p-value less than 0.05 was considered significant. Heterogeneity was assessed using the I² statistic, with thresholds of 25%, 50%, and 75% representing low, moderate, and high heterogeneity, respectively. Subgroup analyses based on study design (randomized controlled trial vs. observational) were conducted to assess the consistency of effect estimates. All statistical analyses were conducted using Review Manager (RevMan version 5.4.1, The Cochrane Collaboration, London, UK).
Results
Figure 1 shows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowchart of study selection. Overall, 944 studies were identified through online database searching. After removing 75 duplicates, the remaining records were initially screened. The full text of 65 studies was obtained, and a detailed assessment was done. Finally, 35 studies were included in the meta-analysis. Table 1 presents characteristics of the included studies. Out of all included studies, five were RCTs and 30 were observational (one prospective observational and 29 retrospective observational), with sample sizes ranging from 18 to 949. Follow-up duration of included studies ranged from three to 64.8 months. The included studies were published between 2018 and 2025. A total of 35 studies were conducted across diverse geographic regions. The majority originated from the United States (14 studies), followed by the United Kingdom (five), China (four), Saudi Arabia (two), Portugal (two), Malaysia (two), and one study each from Iran, Israel, Kenya, Switzerland, France, and various African nations. Table 2 presents demographic characteristics of participants enrolled in the included studies. The mean or median age across studies was generally comparable between groups, ranging from the early 50s to mid-60s in both arms. Female representation varied but was generally lower. Among studies reporting comorbidities, diabetes and hypertension were frequently documented. Diabetes prevalence in the DOAC arms ranged from one to 45 individuals, while in the warfarin arms it ranged from one to 124 individuals. Similarly, hypertension was common across both groups, with up to 90 patients in the DOAC arms and up to 217 in the warfarin arms being affected. However, several studies had missing or unreported data for one or more baseline characteristics. Despite variability, the demographic and clinical profiles between DOAC and warfarin users appeared broadly similar across the studies. Table 3 presents the quality assessment of included studies.
PRISMA flowchart PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Meta-analysis of Outcomes
LVT resolution: Comparison of LVT resolution between DOAC and VKA was done by performing a pooled analysis of 31 studies, and the results are presented in Figure 2. Pooled analysis showed that LVT resolution was not significantly different in subjects receiving DOAC compared to VKA (RR: 1.04, 95% CI: 0.99 to 1.10). Moderate heterogeneity was reported among the study results (I-Square: 30%).
Comparison of thrombus resolution between DOAC and LVTDOAC: direct oral anticoagulant; LVT: left ventricular thrombus[13-16, 18,19, 21, 23-25, 27-43, 45-48]
Stroke or systemic embolism (SSE): Comparison of SSE between DOAC and VKA was done by performing a pooled analysis of 24 studies, and the results are presented in Figure 3. Pooled analysis showed that the risk of SSE was not significantly different between subjects receiving DOAC compared to VKA (RR: 0.91, 95% CI: 0.80 to 1.03). Low heterogeneity was reported among the study results (I-Square: 11%). As shown in the pooled analysis, most of the weight was carried by one study, i.e., Yao et al. [44]. We performed a sensitivity analysis by removing that study. Pooled effect still showed no significant difference is there between the two groups in terms of risk of SSE (RR: 0.95, 95% CI: 0.79 to 1.15).
Comparison of the risk of SSE between DOAC and VKT[13-17, 19-23, 25-27, 31, 33,34, 37,38, 40-42, 44, 46,47]SSE: systemic embolism; DOAC: direct oral anticoagulant; VKT: vitamin K antagonist
Bleeding events: Comparison of the risk of stroke between DOAC and VKA was done by performing a pooled analysis of 25 studies, and the results are presented in Figure 4. Pooled analysis showed that the risk of bleeding events was lower in subjects receiving DOAC compared to VKA, and this difference was statistically significant (RR: 0.88, 95% CI: 0.81 to 0.95). No heterogeneity was reported among the study results (I-Square: 0%). As shown in the pooled analysis, most of the weight was carried by one study, i.e., Yao et al. [44]. We performed a sensitivity analysis by removing that study. Pooled effect still showed low risk of bleeding event in DOAC group (RR: 0.73, 95% CI: 0.60 to 0.89).
Comparison of the risk of bleeding events between DOAC and VKA[13-18, 21-22, 25-27, 31, 33-35, 37-40, 42, 44-48]DOAC: direct oral anticoagulants; VKA: vitamin K antagonist
Subgroup Analysis
Subgroup analyses based on study design (RCTs vs. observational studies) were conducted for the outcomes of LVT resolution, stroke, and bleeding events, and the results are presented in Table 4. For LVT resolution, both RCTs and observational studies demonstrated no significant difference between DOACs and VKAs. The pooled RR from RCTs was 1.05 (95% CI: 0.93 to 1.19; I² = 19%), and from observational studies was 1.04 (95% CI: 0.98 to 1.10; I² = 22%), indicating consistent findings with low heterogeneity across both study designs.
In terms of stroke prevention, DOACs showed a potentially protective effect in RCTs, with an RR of 0.18 (95% CI: 0.02 to 1.52; I² = 0%), although the wide CI suggests imprecision due to a small sample size. Observational studies showed a modest trend favoring DOACs, with an RR of 0.91 (95% CI: 0.80 to 1.03; I² = 6%), though the effect was not statistically significant. Regarding bleeding events, DOACs were associated with a lower risk compared to VKAs. In RCTs, the pooled RR was 0.31 (95% CI: 0.09 to 1.07; I² = 0%), suggesting a trend toward reduced bleeding with DOACs, albeit not statistically significant. Observational studies provided stronger evidence, showing a significant reduction in bleeding risk with an RR of 0.88 (95% CI: 0.81 to 0.95; I² = 0%).
These subgroup findings support the overall trend that DOACs may offer similar efficacy to VKAs for LVT resolution and stroke prevention, while potentially conferring a lower risk of bleeding, especially in real-world observational settings.
Discussion
This systematic review and meta-analysis aimed to compare the efficacy and safety of DOACs versus VKAs in patients with LVT. Our findings suggest that DOACs are comparable to VKAs in terms of efficacy for LVT resolution and stroke prevention. Furthermore, DOACs demonstrated a favorable safety profile, with a lower risk of bleeding events compared to VKAs.
Multiple prior meta-analyses have similarly demonstrated that there is no statistically significant difference in LVT resolution rates between DOACs and VKAs. For example, a meta-analysis by Li et al. [49], which included 17 studies, reported an RR of 1.07 for LVT resolution with DOACs compared to VKAs (95% CI: 0.97-1.18; p = 0.193). In another meta-analysis encompassing 21 studies, Huang et al. [50] observed a comparable effect size, with an RR of 1.06 (95% CI: 0.98-1.13; p = 0.13), reinforcing the conclusion that both anticoagulant strategies yield similar outcomes in promoting LVT resolution. Our current meta-analysis updates these findings by including recently conducted RCTs and observational studies.
The most effective anticoagulation strategy for managing LVT remains uncertain. Existing clinical guidelines continue to advocate for the use of warfarin as the standard treatment in this setting. Despite its proven efficacy, warfarin presents several drawbacks that limit its practicality, such as the need for regular INR monitoring, significant interactions with food and other medications, a prolonged half-life, and challenges with maintaining patient adherence due to its narrow therapeutic range [51].
Our meta-analysis demonstrated that the rate of LVT resolution is similar between patients receiving DOACs and those treated with VKAs. Achieving thrombus resolution is a critical therapeutic goal, as the presence of LVT is associated with a substantially worse prognosis, including an increased risk of major adverse cardiovascular events, serious bleeding, overall mortality, and a higher likelihood of embolic events [52].
The optimal length of anticoagulant therapy in patients with LVT has yet to be clearly defined. Evidence suggests that the risk of thromboembolic events is particularly elevated during the initial two weeks following a myocardial infarction, while the likelihood of LVT recurrence peaks within the first three months post-infarction [53]. Recent guidance from the American Heart Association recommends follow-up imaging around the three-month mark after acute myocardial infarction, with the discontinuation of anticoagulation if no thrombus is observed [3]. In individuals with dilated cardiomyopathy complicated by LVT, a minimum treatment duration of three to six months is typically advised [54].
In conclusion, this meta-analysis provides evidence supporting the use of DOACs as a treatment option for LVT. Our findings suggest that DOACs offer similar efficacy to VKAs while potentially providing a better safety profile with reduced bleeding risk. Nonetheless, confirmation through large-scale randomized controlled trials with sufficient sample sizes and extended follow-up periods remains necessary.
This meta-analysis has several important limitations that temper the confidence in recommending DOACs as a first-line alternative for LVT management. Firstly, most included studies were retrospective, with variable follow-up durations and clinical settings, introducing potential bias and limiting causal inference. Considerable heterogeneity was observed across studies in terms of patient populations, antithrombotic regimens, and imaging modalities, complicating direct comparisons and the generalizability of results. Most studies relied on echocardiography for assessing LVT resolution, which may overestimate thrombus clearance compared to more sensitive imaging methods like cardiac MRI. There was also substantial variability in antiplatelet therapy use, and due to insufficient data, we could not assess outcomes of anticoagulation alone versus combination therapy with antiplatelets. Similarly, the optimal DOAC dosing strategies and treatment durations remain unclear, as these were inconsistently reported and not uniformly evaluated across studies. Subgroup analyses based on clinical scenarios such as acute coronary syndrome (ACS) or percutaneous coronary intervention (PCI) were not feasible due to the lack of detailed stratified data. These gaps highlight the need for further investigation in specific patient subgroups, standardized imaging methods, and clearer documentation of adjunctive therapies. Although some findings appeared consistent across RCTs and observational studies, this consistency varied by outcome and study design. For example, the observed bleeding risks were more pronounced in observational data, suggesting potential differences in patient selection or unmeasured confounding.
Overall, while the results provide valuable insights, they must be interpreted cautiously. Future large-scale, high-quality RCTs are essential to definitively establish the comparative efficacy and safety of DOACs versus VKAs in LVT treatment. These should also explore tailored treatment approaches based on patient characteristics, DOAC dosing regimens, and concurrent antiplatelet use to inform optimal clinical decision-making.
Conclusions
This comprehensive meta-analysis of 35 studies comparing DOACs to VKAs in patients with LVT demonstrates that DOACs provide comparable efficacy in thrombus resolution and stroke prevention while offering a superior safety profile with significantly reduced bleeding risk. These findings challenge the current paradigm of VKAs as the exclusive standard of care for LVT management. The consistent results across randomized controlled trials and observational studies strengthen the validity of our conclusions. However, limitations in study design, follow-up duration, and imaging techniques necessitate cautious interpretation. Further large-scale randomized controlled trials with extended follow-up periods are essential to definitively establish DOACs as a first-line alternative to VKAs for LVT management and to determine optimal dosing regimens and treatment durations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Emerging trends in left ventricular thrombus: a comprehensive review of non-ischemic and ischemic cardiopathies, including eosinophilic myocarditis, Chagas cardiomyopathy, amyloidosis, and innovative anticoagulant approaches Diagnostics (Basel) Colle B Demeure F Higny J 9481420243873236110.3390/diagnostics 14090948 PMC 11083388 · doi ↗ · pubmed ↗
- 2Advancing clinical management of left ventricular thrombosis: prevention, detection and treatment modalities in the modern era Heart Zhang Q Zheng H Zhang Z Xu Y Zhang W 202510.1136/heartjnl-2024-324605 PMC 1222906539938942 · doi ↗ · pubmed ↗
- 3Management of patients at risk for and with left ventricular thrombus: a scientific statement from the American Heart Association Circulation Levine GN Mc Evoy JW Fang JC 023146202210.1161/CIR.000000000000109236106537 · doi ↗ · pubmed ↗
- 4Left ventricular thrombus therapy with direct oral anticoagulants versus vitamin K antagonists: a systematic review and meta-analysis J Cardiovasc Pharmacol Ther Saleiro C Lopes J De Campos D Puga L Costa M Gonçalves L Teixeira R 2332432620213325923510.1177/1074248420977567 · doi ↗ · pubmed ↗
- 5Non-vitamin K antagonist oral anticoagulants: considerations on once- vs. twice-daily regimens and their potential impact on medication adherence Europace Vrijens B Heidbuchel H 5145231720152569453810.1093/europace/euu 311 · doi ↗ · pubmed ↗
- 6Safety of direct oral anticoagulants versus traditional anticoagulants in venous thromboembolism J Thromb Thrombolysis Giustozzi M Franco L Vedovati MC Becattini C Agnelli G 4394534820193110419410.1007/s 11239-019-01878-x · doi ↗ · pubmed ↗
- 7Direct oral anticoagulant use: a practical guide to common clinical challenges J Am Heart Assoc Chen A Stecker E A Warden B 09202010.1161/JAHA.120.017559 PMC 767054132538234 · doi ↗ · pubmed ↗
- 8Evaluation of oral anticoagulants with vitamin K epoxide reductase in its native milieu Blood Chen X Jin DY Stafford DW Tie JK 1974198413220183008962810.1182/blood-2018-05-846592 PMC 6213321 · doi ↗ · pubmed ↗