Survival Without Sequelae From Severe Acidosis Due to Sepsis and Acute Kidney Injury Following Colitis: A Case Report
Sanjoy George, Nishad Raveendran, Ateeq Omer

TL;DR
A patient with severe acidosis due to sepsis and kidney injury survived without long-term effects thanks to timely treatment and a team-based approach.
Contribution
This case highlights that severe acidosis is not always fatal if treated promptly and effectively.
Findings
A patient with a pH below 6.5 due to acidosis survived with no functional deficits.
Timely resuscitation and a multidisciplinary approach were key to the patient's recovery.
Severe acidosis can be compatible with life when managed aggressively.
Abstract
When the pH is significantly low, metabolic acidosis is considered severe, and such a low level is typically regarded as incompatible with life. Despite being an indication of a bad prognosis, severe acidosis alone is not a strong enough predictor of outcome to support the refusal of resuscitation. Timely interventions can sometimes achieve recovery from extremely severe acidosis. Here, we report a case of severe metabolic acidosis with a pH less than 6.5 associated with sepsis and acute kidney injury, who survived without any functional deficits by timely resuscitation and a multidisciplinary approach.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
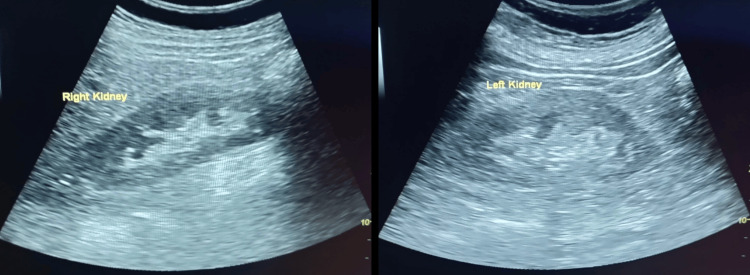 Figure 1
Figure 1| Test | Results | Reference range |
| PH | < 6.500 | 7.350 – 7.450 |
| pCO2 | 25.8 mmHg | 35.0 – 48.0 mmHg |
| pO2 | 169.2 mmHg | 83.0 – 108.0 mmHg |
| cHCO3 | cnc* | 21.0 – 28.0 mmol/L |
| BE(ecf) | cnc* | -2.0 – 3.0 mmol/L |
| cSO2 | cnc* | 94.0 – 98.0 % |
| Na+ | 127 mmol/L | 138 – 146 mmol/L |
| K+ | 7.6 mmol/L | 3.5 – 4.5 mmol/L |
| Ca++ | 0.88 mmol/L | 1.15 – 1.33 mmol/L |
| Cl- | 105 mmol/L | 98 – 107 mmol/L |
| cTCO2 | cnc* | 22.0 – 29.0 mmol/L |
| AGapK | cnc* | 10 – 20 mmol/L |
| Hct | 26 | 38 – 51 % |
| cHgb | 8.9 g/dL | 12.0 – 17.0 g/dL |
| BE(b) | cnc* | -2.0 – 3.0 mmol/L |
| Glu | 182 mg/dL | 74 – 100 mg/dL |
| Lactate | 17.27 mmol/L | 0.56 – 1.39 mmol/L |
| BUN | 58 mg/dL | 8 – 26 mg/dL |
| Crea | 5.99 mg/dL | 0.51 – 1.19 mg/dL |
| BUN/Crea | 9.8 mg/mg | 12.0 – 20.0 mg/dL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRenal function and acid-base balance · Sepsis Diagnosis and Treatment · Abdominal Surgery and Complications
Introduction
Maintaining acid-base balance is essential for healthy physiology. Systemic acid-base balance is typically well-regulated, with arterial pH ranging from 7.36 to 7.44. Transmembrane transport, metabolic enzymes, and several vital cellular functions are all extremely sensitive to pH. Acute metabolic acidosis is common in seriously ill patients and, when severe, can be associated with a poor clinical outcome [1,2]. Acute metabolic acidosis is associated with increased morbidity and mortality because of its depressive effects on cardiovascular function, facilitation of cardiac arrhythmias, decreased cardiac output, arterial dilatation with hypotension, impaired oxygen delivery, decreased adenosine triphosphate (ATP) production, stimulation of inflammation, suppression of the immune response, and other adverse effects [3,4]. Metabolic acidosis is considered severe when the pH is less than 7.2, and a very low pH is usually considered incompatible with life [5]. Severe metabolic or mixed acidemia was associated with a mortality rate of 57% in the ICU [6].
Case presentation
A 76-year-old woman presented to us with complaints of loose stools and vomiting for two days. She has a history of type 2 diabetes mellitus and systemic hypertension for the last eight years and was on insulin and the tablet amlodipine 5 mg twice daily. There was no history of any other significant illness in the past. Her complaints started following the consumption of pork meat two days prior to presentation. She had eight to 10 episodes of loose stools per day for the last two days. She was not on metformin, and there was no history suggestive of any toxin ingestion. On arrival at the hospital, her Glasgow Coma Scale was 4/15. Her pulse was 98 beats per minute, blood pressure was 60/40 mmHg, temperature was 98.6°F, and SpO_2_ was 52% on room air. Arterial blood gas analysis showed a pH of less than 6.5, bicarbonate was undetectable, lactate was 17.27 mmol/L, potassium was 7.6 mmol/L (Table 1), and serum creatinine was 6.4 mg/dL.
The patient had a triple acid-base disorder: high anion gap metabolic acidosis, respiratory acidosis, and metabolic alkalosis. Her serum albumin was 3.3 mg/dl, and lipase was 88. Her random blood glucose level was 180 mg/dl, and HbA1c was 8.8%. Hemogram showed neutrophilic leukocytosis (hemoglobin 8.5, total count 15300, platelet count 289000) and increased C-reactive protein (CRP) 54.25 and procalcitonin (3.66).
She was intubated and started on mechanical ventilatory support. A bolus of intravenous (IV) fluid was given, and as blood pressure was not maintained, norepinephrine and vasopressin support were started. Intravenous bicarbonate was given, and she was started on broad-spectrum antibiotics after taking blood samples for culture and sensitivity. Her blood sugar levels were closely monitored, and insulin infusion was given. After six hours, she remained anuric, and a repeat arterial blood gas (ABG) showed mild improvement in pH (6.54), but lactate had increased to 21 mmol/L. Even though continuous renal replacement therapy (CRRT) is the preferred modality for treating patients in shock due to its superior hemodynamic stability and reduced risk of dialysis disequilibrium syndrome [7], she was taken for sustained low-efficiency dialysis (SLED) as the facility for CRRT was not available. Ultrasonography of the abdomen showed normal-sized kidneys with no evidence of obstruction (Figure 1) and diffuse wall thickening of the small and large intestines, suggestive of colitis.
Ultrasound of the abdomen image showing both kidneys
Her condition improved with intravenous antibiotics and other supportive measures, and two sessions of SLED and ionotropic supports were tapered and stopped. She was weaned off ventilatory support and was extubated. Blood and stool cultures didn’t yield any growth, and lactate came down to 2.4.
She had a complete neurological recovery without any deficits, even though she didn’t remember the events. She had adequate urine output and didn’t require further renal replacement therapy. She was discharged home in a stable condition. On her follow-up visit, her serum creatinine had decreased to 3.3 mg/dl with good urine output. She was lost to follow-up after that.
Discussion
Few studies in the literature have, as far as we are aware, documented a patient who survived a very low arterial blood pH due to metabolic acidosis. A case with an arterial blood pH of 6.48, which developed following status epilepticus and in which the patient recovered successfully, is reported [8]. A 62-year-old man who was taking metformin was reported to have hypothermia (core body temperature of 29ºC) and uncompensated respiratory acidosis and lactic acidosis coupled with an arterial blood pH of 6.38 [9]. Another case report is of a 24-year-old man who, following near-drowning cardiac arrest, developed severe metabolic acidosis with an arterial blood pH of 6.33 [10]. The lowest arterial blood pH reported in the literature (6.30) was described as occurring in an 84-year-old man and was related to metformin use, but more data are not available [11]. Our patient was an elderly female with significant comorbidities who presented with features of severe sepsis. The presence of hypotension, lactic acidosis, and renal failure is associated with poor outcomes in patients with sepsis. A very low pH is considered incompatible with life. However, timely and stepwise treatment, including renal replacement therapy, led to the patient's complete recovery. Even though survival without any deficit from a very low pH is rare, unbiased, timely, and protocol-based multidisciplinary resuscitation may often lead to favorable outcomes.
Conclusions
Even simple gastroenteritis can progress to sepsis, multi-organ dysfunction, and death, especially in the elderly. Prompt protocol-based resuscitation is crucial for surviving sepsis. Survival without sequelae from very low pH may be rare, but not impossible. A very low pH should not be a reason to discontinue resuscitation. Decisions about resuscitation and treatment should be guided by the results of an overall clinical evaluation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lactate versus non-lactate metabolic acidosis: a retrospective outcome evaluation of critically ill patients Crit Care Gunnerson KJ Saul M He S Kellum JA 010200610.1186/cc 3987 PMC 155083016507145 · doi ↗ · pubmed ↗
- 2Occurrence and adverse effect on outcome of hyperlactatemia in the critically ill Crit Care Khosravani H Shahpori R Stelfox HT Kirkpatrick AW Laupland KB 013200910.1186/cc 7918 PMC 271746119523194 · doi ↗ · pubmed ↗
- 3Treatment of acute metabolic acidosis: a pathophysiologic approach Nat Rev Nephrol Kraut JA Madias NE 589601820122294549010.1038/nrneph.2012.186 · doi ↗ · pubmed ↗
- 4Metabolic acidosis: pathophysiology, diagnosis and management Nat Rev Nephrol Kraut JA Madias NE 274285620102030899910.1038/nrneph.2010.33 · doi ↗ · pubmed ↗
- 5Diagnosis and management of metabolic acidosis: guidelines from a French expert panel Ann Intensive Care Jung B Martinez M Claessens YE 92920193141809310.1186/s 13613-019-0563-2PMC 6695455 · doi ↗ · pubmed ↗
- 6Severe metabolic or mixed acidemia on intensive care unit admission: incidence, prognosis and administration of buffer therapy. A prospective, multiple-center study Crit Care Jung B Rimmele T Le Goff C 015201110.1186/cc 10487 PMC 333478921995879 · doi ↗ · pubmed ↗
- 7Handbook of Dialysis Daugirdas JT Blake PG Ing TS 300Philadelphia, PA Wolters Kluwer Health 2025 https://play.google.com/store/books/details?pcampaignid=books_read_action&id=Vrh SEQAAQBAJ&pli=1
- 8Surviving the impossible: a case report on critically low arterial blood p H of 6.48 that recovered successfully Chest Hadid R Chandramohan S Saoji A Al Hassan S 01562019