Marginal zone lymphoma masquerading as phymatous acne rosacea: a case study
Hina S Baloch, Zhenghao Wang, Joy U L Staniforth, Azaharry Yaakub

TL;DR
A rare case of marginal zone lymphoma was mistaken for phymatous acne rosacea, highlighting the need for early biopsy in atypical skin conditions.
Contribution
This paper presents a rare case of MZL mimicking phymatous acne rosacea, emphasizing diagnostic challenges and the importance of histological evaluation.
Findings
The patient's skin lesions were initially misdiagnosed as acne rosacea but were later confirmed as cutaneous MZL via biopsy.
Systemic imaging revealed lymph node enlargement and splenomegaly, indicating primary systemic nodal MZL.
Chemotherapy improved both skin and systemic symptoms, but treatment was stopped due to intolerance.
Abstract
Marginal zone lymphoma (MZL) is an indolent B-cell lymphoma characterized by considerable heterogeneity in clinical presentation. Cutaneous MZL typically manifests as papules, plaques or nodules, often affecting the trunk and arms. Rare cases of MZL presenting as acne rosacea have been reported; however, these have been primarily reported as granulomatous rosacea. Specific evidence of MZL presenting as phymatous acne rosacea is extremely rare and not well documented in the medical literature. We report a rare case of primary systemic nodal MZL manifesting alongside cutaneous extra-nodal MZL, mimicking rhinophymatous and otophymatous acne rosacea. An 84-year-old White man with a 13-year history of nodal MZL, under active monitoring, presented with erythematous, swollen lesions on the ears and nose. This was initially diagnosed as acne rosacea; however, conventional treatment proved…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1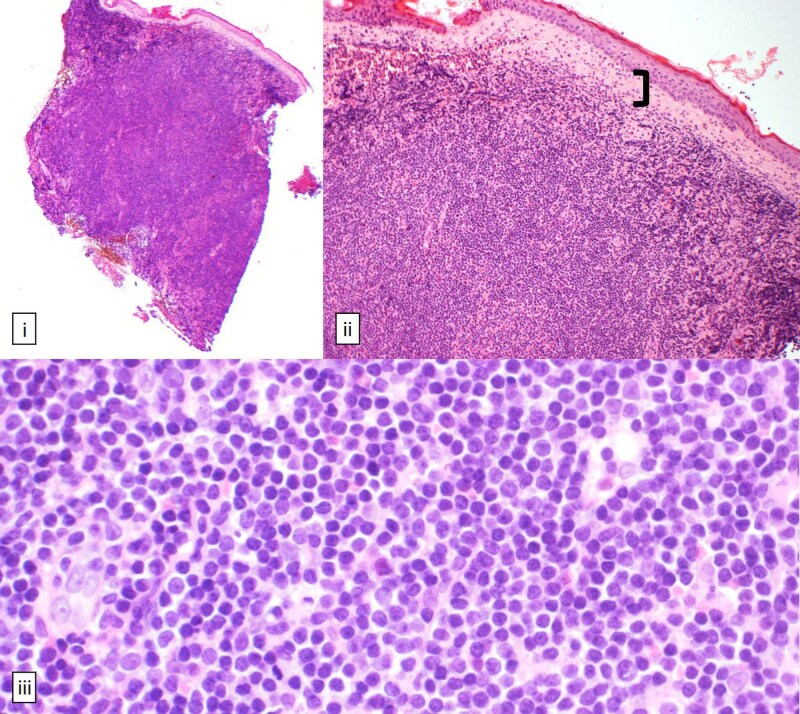 Figure 2
Figure 2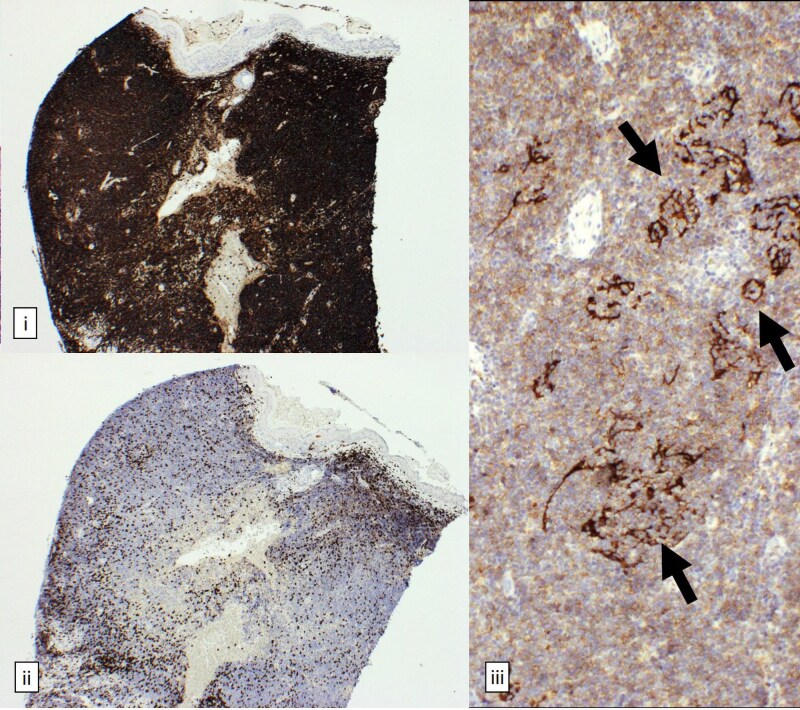 Figure 3
Figure 3 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCutaneous lymphoproliferative disorders research · Acne and Rosacea Treatments and Effects · Autoimmune Bullous Skin Diseases
Marginal zone lymphoma (MZL) is a form of non-Hodgkin B-cell lymphoma and is the second most prevalent form of indolent B-cell lymphoma. Recent years have seen a rise in the incidence of MZL overall as well as in its various subtypes, with the incidence of MZL ranging from 0.5 to 2.92 cases per 100 000 person-years, depending on the geographical region.^1^ MZL is classified into three subtypes: mucosa-associated lymphoid tissue (MALT) lymphoma, which accounts for 70% of cases; splenic MZL, representing 20%; and nodal MZL, making up 10%. In some instances, MZL presents with advanced-stage disease where a distinct pattern of organ involvement cannot be identified, and these cases are typically referred to as disseminated MZL.^2^
MZLs may manifest cutaneously as a primary cutaneous malignancy, or as a result of secondary involvement from noncutaneous MZL. While cutaneous MZL most commonly presents as papules, plaques and nodules seen on the arm or trunk, cutaneous B-cell lymphomas have a broad spectrum of clinical presentations, which makes subsequent diagnosis and management challenging.^3,4^
We report a rare case of primary systemic nodal marginal zone lymphoma manifesting alongside cutaneous extra-nodal MZL, mimicking rhinophymatous and otophymatous acne rosacea. This rare case underscores the heterogeneous presentation of MZL, particularly its phymatous appearance, and highlights the importance of a comprehensive physical examination to identify potential systemic features and the necessity of early histological confirmation in all atypical skin presentations.
Case report
An 84-year-old Caucasian man with a 13-year history of nodal marginal zone lymphoma under active monitoring was observed to have swollen erythematous lesions on his ears and nose during a routine haematology follow-up. An initial diagnosis of acne rosacea was made, which proved non-responsive to two courses of topical therapies. Subsequently, he was started on oxytetracycline in the community and referred to our secondary care dermatology clinic. On examination (Figure 1), he exhibited phymatous changes to the nose and both ears, with redness and firm swelling of the earlobes extending to the helix and antihelix bilaterally. There was redness and swelling of the tip of the nose, along with small papules on the right side of the neck. Systemic examination revealed submandibular lymphadenopathy and splenomegaly.
Bilateral erythema and swelling of both earlobes (otophyma) and redness and swelling of the nose (rhinophyma).
Investigation
Given the atypical presentation inconsistent with classical rosacea, skin biopsies were performed on the left earlobe and right side of the neck. Skin biopsy of the right neck demonstrated granulomatous rosacea. However, histological examination of the left earlobe (Figure 2) revealed a diffuse, dense monomorphic infiltrate of dermis-replacing small lymphoid B cells with rounded nuclei and stippled chromatin. Immunohistochemistry (Figure 3) demonstrated positive expression of CD20, CD79a and BCL2, weak expression of CD21, and no expression of CD3, CD5, CD10, BCL6, cyclin D1 and CD30. There were scattered underlying disrupted CD21-positive follicular dendritic cell meshworks, with no morphological evidence of epithelioid malignancy. These features were in keeping with cutaneous MZL.
Haematoxylin and eosin staining [(i) 40×, (ii) 100×, (iii) 400×]. (ii) Dermal dense cellular infiltrate separated from epidermis by a grenz zone [(ii), bracket]. (iii) Infiltrate comprises small, monomorphic lymphoid cells showing high nuclear-to-cytoplasmic ratios with rounded nuclei and stippled chromatin.
Immunohistochemistry [(i) and (ii) 40×, (iii) 100×]. (i) Infiltrating CD20+ B cells. (ii) Scattered admixed CD3+ T cells and underlying disrupted follicular dendritic cell meshworks [(iii), arrows]. B cells express CD79a and BCL2, weakly express CD21 (iii); and are negative for CD3 (ii).
A computed tomography (CT) scan of the neck, thorax, abdomen and pelvis revealed enlarged lymph nodes both above and below the diaphragm, along with splenomegaly, demonstrating diffuse systemic lymphoma.
Treatment and follow-up
Considering his disseminated MZL, he was started on R-CVP chemotherapy (rituximab, cyclophosphamide, vincristine and prednisolone). After completing four cycles of chemotherapy, his skin condition showed dramatic improvement (Figure 4). Unfortunately, he was unable to tolerate further chemotherapy and now remains under active monitoring. Subsequent CT scans have shown subcentimetre lymph nodes and a reduction in spleen size.
Resolution post-chemotherapy.
Discussion
Phymas, encompassing conditions such as rhinophyma and otophyma, represent an uncommon but significant manifestation of rosacea and illustrate the complex spectrum of acne rosacea presentation. Phymas develop in approximately 5–10% of those affected by acne rosacea, characterized by sebaceous hyperplasia, fibrosis and localized lymphoedema. This commonly affects the nose (rhinophyma), but may also affect the chin (gnathophyma), forehead (metophyma) and ears (otophyma). Cutaneous presentations of MZL include a broad range of clinical manifestations, most commonly nodules, plaques or papules often affecting the trunk or limbs. While there have been rare cases reported of MZL presenting as acne rosacea,^3–5^ these have been reported as primarily granulomatous rosacea, and evidence of MZL presenting specifically as phymatous disease is extremely sparse and not well documented in the medical literature.
This case is notable due to the rare involvement of both the nose and ears, mimicking rhinophyma and otophyma, highlighting the diverse presentation of MZL and emphasizing the importance of a comprehensive physical examination. Conventional therapies for acne rosacea proved ineffective, and referral to secondary care dermatology and skin biopsy was essential for a definitive diagnosis. Atypical phymatous presentations of disease often lead to misdiagnosis, resulting in mismanagement and delays in appropriate treatment. This highlights the critical need for dermatological expertise and prompt histopathological evaluation to differentiate phymas from mimicking conditions such as inflammatory disorders, lymphomas, cryoglobulinaemia and cryofibrinogenaemia, granulomatous disorders such as sarcoidosis, and squamous cell and basal cell carcinomas. While surgical intervention is often required for advanced cases of phymatous rosacea, recognition of the cutaneous MZL allowed early treatment with R-CVP chemotherapy, resulting in a dramatic improvement in the patient’s skin condition and overall systemic disease.
Prognosis of MZL varies significantly depending on the subtype, with MALT lymphomas exhibiting better outcomes than nodal or splenic variants.^6^ In this case, prompt initiation of chemotherapy led to a marked improvement in cutaneous and systemic symptoms. Nevertheless, the involvement of multiple organ systems, including the skin and lymph nodes, necessitates careful monitoring for disease progression and transformation into more aggressive subtypes, such as diffuse large B-cell lymphoma.^7^ Although rare, lymphoma should be considered in the differential diagnosis of all atypical or nonresponsive rosacea. Early histopathological evaluation is crucial to differentiate between benign and malignant conditions.
The rare phymatous presentation of MZL in this report illustrates the need for dermatologists and clinicians to consider lymphoma in the differential diagnosis of persistent, treatment-resistant rosacea-like conditions, and highlights the importance of histological evaluation in patients with persistent or atypical dermatological findings. Although rosacea, especially phymatous forms, can present similarly, clinicians must maintain a high index of suspicion for underlying malignancies in new cases that do not respond to standard therapy. Early biopsy and histopathology are essential to ensure timely diagnosis and treatment.
Additional statements
H.S.B. and Z.W., as co-first authors, contributed equally.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Auñón C, Sanvisens A, Turon E et al Time trends and survival of marginal zone lymphoma over 25 years in Girona, Spain (1994–2018). Cancer Med 2023; 12:12343–53.37076996 10.1002/cam 4.5935 PMC 10278498 · doi ↗ · pubmed ↗
- 2Cheah CY, Seymour JF. Marginal zone lymphoma: 2023 update on diagnosis and management. Am J Hematol 2023; 98:1645–57.37605344 10.1002/ajh.27058 · doi ↗ · pubmed ↗
- 3Gerami P, Wickless SC, Querfeld C et al Cutaneous involvement with marginal zone lymphoma. J Am Acad Dermatol 2010; 63:142–5.20462658 10.1016/j.jaad.2009.07.047 · doi ↗ · pubmed ↗
- 4Agnihotri T, Adotama P, Kalowitz-Bieber A et al A case of primary cutaneous marginal zone lymphoma presenting with rosacea-like eruption. JAAD Case Rep 2020; 6:902–4.32875041 10.1016/j.jdcr.2020.07.018PMC 7452266 · doi ↗ · pubmed ↗
- 5Barzilai A, Feuerman H, Quaglino P et al Cutaneous B-cell neoplasms mimicking granulomatous rosacea or rhinophyma. Arch Dermatol 2012; 148:824–31.22508769 10.1001/archdermatol.2011.3575 · doi ↗ · pubmed ↗
- 6Dalle S, Thomas L, Balme B et al Primary cutaneous marginal zone lymphoma. Crit Rev Oncol Hematol 2010; 74:156–62.19819717 10.1016/j.critrevonc.2009.09.003 · doi ↗ · pubmed ↗
- 7Harris E, Sindel A, Mc Connell I et al Transformation from indolent primary cutaneous marginal zone lymphoma to aggressive primary cutaneous diffuse large B-cell lymphoma: a rare case and review of the literature. Blood 2019; 134:5266.