A case of eosinophilic pustular folliculitis involving palmoplantar successfully treated by apremilast
Jing Xu, Yue-meng Wu, Shang-shang Wang

TL;DR
A man with a rare skin condition called eosinophilic pustular folliculitis was successfully treated with apremilast, a drug that may be effective when traditional treatments fail.
Contribution
This case demonstrates apremilast's effectiveness in treating EPF, especially in areas like palms and soles where treatment is challenging.
Findings
Apremilast successfully treated EPF in a patient with lesions on the face, palms, and soles.
The treatment was effective when traditional therapies had failed.
This supports growing evidence for apremilast in managing EPF.
Abstract
We presented a man with EPF involving the face, palms and soles, successfully treated by apremilast, a phosphodiesterase-4 (PDE4) inhibitor. Apremilast’s efficacy in this case adds to emerging evidence supporting its use in EPF, particularly when traditional treatments fail. Eosinophilic pustular folliculitis (EPF) is a rare inflammatory dermatosis that predominantly affects seborrheic areas. The condition’s pathogenesis is linked to T helper 2-driven eosinophilic inflammation. We presented a man with EPF involving the face, palms and soles, successfully treated by apremilast, a phosphodiesterase-4 inhibitor. Apremilast’s efficacy in this case adds to emerging evidence supporting its use in EPF, particularly when traditional treatments fail.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
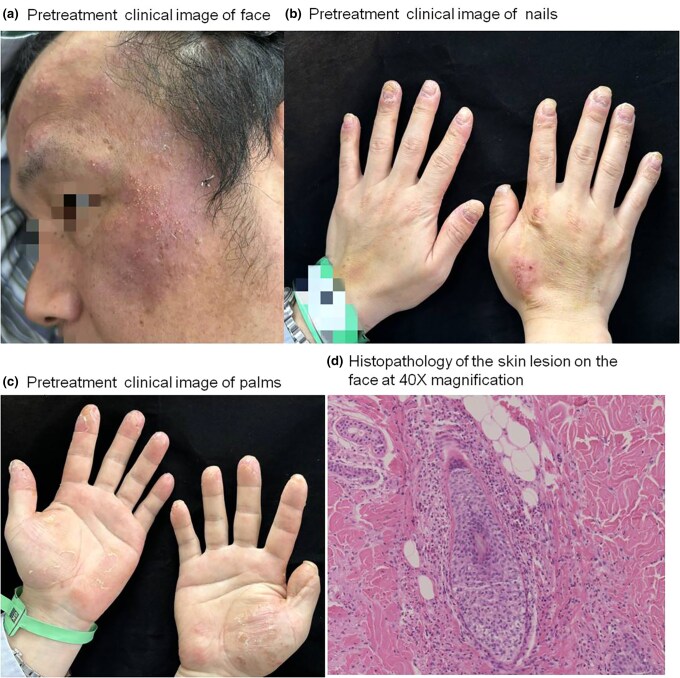 Figure 1
Figure 1 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEosinophilic Disorders and Syndromes · Nail Diseases and Treatments · Cutaneous lymphoproliferative disorders research
Introduction
Eosinophilic pustular folliculitis (EPF) was first described in 1965 by Ofuji and is characterized by recurrent papulopustular eruptions, typically involving seborrheic areas of the body such as the scalp, face and trunk.^1^ It is a rare inflammatory condition, with several subtypes, including classical EPF, immunosuppression-associated EPF and infantile EPF.^2^ Although lesions are primarily confined to hair-bearing areas, atypical presentations involving non-seborrheic sites such as the palms, soles and nails are exceedingly rare.^3^
The exact pathogenesis of EPF remains incompletely understood, but it may be a non-specific response to various antigenic stimuli that impair the immune system.^4^ This inflammatory milieu causes pustule formation, tissue damage and the chronic relapsing nature of the disease. Given the rarity of the condition, especially when involving non-seborrheic areas, EPF is often misdiagnosed as other dermatoses like palmoplantar pustulosis or psoriasis, leading to delays in appropriate treatment.
Management of EPF remains challenging due to its relapsing nature and the lack of standardized therapeutic protocols. Treatments ranging from indomethacin and dapsone to corticosteroids and immunomodulators have been utilized with varying success.^5^ Recently, apremilast, a selective inhibitor of phosphodiesterase-4 (PDE4), has emerged as a potential treatment option due to its anti-inflammatory effects. This case report describes a patient with EPF involving the face, palms and soles who responded favourably to apremilast after not improving with conventional treatments.
Case report
A 40-year-old man presented with a 6-month history of pruritic erythematous papules and pustules on the palms and soles, with subsequent involvement of the face 1 month later. The patient reported exacerbation of the lesions after wearing rubber gloves, although no definitive triggers were identified. In addition to cutaneous manifestations, the patient also exhibited periungual erythema and nail deformities, including thickening and ridging (pachyonychia) (Figure 1a,b,c).
Pretreatment clinical presentation of the eosinophilic pustular folliculitis (EPF) patient: (a) face, (b) nails and (c) palms. (d) Pathological appearance of biopsy specimens from the face.
Initial treatment with acitretin (an oral retinoid), topical triamcinolone acetonide, and econazole nitrate cream and tacrolimus ointment for more than 6 weeks provided no significant improvement, leading to further diagnostic evaluation. A skin biopsy from the cheek revealed a dense eosinophilic infiltrate in both the superficial and deep dermis, with evidence of folliculocentric inflammation (Figure 1d). Laboratory tests demonstrated marked eosinophilia (792 × 10^6^/L), but total immunoglobulin E was within the normal range. Viral serologies, including HIV, hepatitis B and hepatitis C, were negative.
A diagnosis of eosinophilic pustular folliculitis (EPF) was made based on clinical, histopathological and laboratory findings. Given the patient’s refractory response to previous treatments, apremilast was initiated with a gradual titration over 5 days. Significant clinical improvement was noted within 2 weeks, with complete remission of skin lesions by week 12 (Figure 2), laboratory tests demonstrated that eosinophil count has decreased to the normal range (86 × 10^6^/L). The patient continued to be followed for 6 months without recurrence, and no adverse effects were reported during treatment.
After 2 weeks treatment clinical image of (a) face and (b) palms, and after 12 weeks treatment clinical image of (c) face and (d) palms.
Discussion
EPF, particularly with palmoplantar involvement, presents a diagnostic challenge due to its rarity and resemblance to other dermatoses.^1^ In this case, the patient was initially misdiagnosed with palmoplantar pustulosis, a more common condition characterized by pustules on the palms and soles. However, the presence of eosinophilia and histopathological findings consistent with eosinophilic infiltration led to the correct diagnosis of EPF.
EPF has been historically treated with a wide range of therapies, including indomethacin, dapsone and topical or systemic corticosteroids.^5^ However, these treatments often provide only partial relief, and relapses are common. The underlying pathophysiology of EPF suggests that T helper 2 (Th2)-mediated eosinophilic inflammation plays a critical role in the disease process, making therapies that target Th2 cytokines, such as interleukin (IL)-4, IL-5 and IL-13, potentially effective.^6^ Immunohistochemistry or serology to these cytokines before and after treatment can be performed to verify the efficacy.
Emerging treatments for EPF include biologic agents and small-molecule inhibitors. Dupilumab, an IL-4 receptor antagonist, has been reported to successfully treat EPF by inhibiting Th2-driven inflammation.^6^ Similarly, mepolizumab (an anti-IL-5 monoclonal antibody) and adalimumab [a tumour necrosis factor alpha (TNF-α) inhibitor], have shown promise in reducing eosinophilic infiltration and alleviating symptoms of EPF.^7,8^ Abrocitinib, a Janus kinase inhibitor, has also been used successfully in recent cases of EPF.^9^
Apremilast, a PDE4 inhibitor, works by reducing the production of pro-inflammatory cytokines, including TNF-α, IL-17 and IL-23, which are involved in various inflammatory skin diseases.^10^ Its efficacy in this case is noteworthy, as the patient achieved complete remission without significant adverse effects. This adds to a growing body of evidence supporting the use of apremilast in eosinophilic dermatoses, particularly in cases refractory to conventional treatments.
This case highlights the importance of considering eosinophilic pustular folliculitis in the differential diagnosis of palmoplantar dermatoses. The successful treatment of this patient with apremilast underscores the potential of PDE4 inhibitors in managing EPF, a condition for which no standardized treatment guidelines currently exist. Further research is needed to explore the long-term efficacy and safety of apremilast and other emerging therapies in EPF.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Angelo VM, Giovanni G. Eosinophilic dermatoses: recognition and management. Am J Clin Dermatol 2020; 21:525–39.32394361 10.1007/s 40257-020-00520-4 · doi ↗ · pubmed ↗
- 2Nomura T, Katoh M, Yamamoto Y et al Eosinophilic pustular folliculitis: a published work-based comprehensive analysis of therapeutic responsiveness. J Dermatol 2016; 43:919–27.26875627 10.1111/1346-8138.13287 · doi ↗ · pubmed ↗
- 3Noriko UA, Tanemoto S, Tanese K et al Eosinophilic pustular folliculitis with palmoplantar lesions and nail deformity. J Dermatol 2020; 47:e 357–9.32677109 10.1111/1346-8138.15503 · doi ↗ · pubmed ↗
- 4Nomura T, Katoh M, Yamamoto Y et al Eosinophilic pustular folliculitis: the transition in sex differences and interracial characteristics between 1965 and 2013. J Dermatol 2015; 42:343–52.25675987 10.1111/1346-8138.12783 · doi ↗ · pubmed ↗
- 5Li Y, Chen G, Zhou X et al Clinical and pathological analysis of 10 cases of eosinophilic pustular folliculitis. Clin Cosmet Investig Dermatol 2023; 16:2467–72.10.2147/CCID.S 427718 PMC 1050351537719931 · doi ↗ · pubmed ↗
- 6Marie O, Marine V, Nathalie CL, Thierry P. Successful treatment of eosinophilic pustular folliculitis with dupilumab. JAMA Dermatol 2024; 160:114–5.37910114 10.1001/jamadermatol.2023.4305 · doi ↗ · pubmed ↗
- 7Filippo C, Enrico Z, Vanessa M et al Mepolizumab therapy for eosinophilic pustular folliculitis (Ofuji disease). J Eur Acad Dermatol Venereol 2024;38:e 993–6.38687252 10.1111/jdv.20047 · doi ↗ · pubmed ↗
- 8Ramondetta A, Giuffrida G, Vincenzo SD et al A case of eosinophilic pustular folliculitis successfully treated with adalimumab. Dermatol Ther 2022; 35:e 15550.35508711 10.1111/dth.15550 · doi ↗ · pubmed ↗