Best foot forward: podiatrists’ insight and awareness of melanoma of the foot—a questionnaire study
Brian Nolan, Cathal O’Connor, Michelle Murphy

TL;DR
This study explores how often podiatrists encounter and handle melanoma on the feet, finding that most feel undertrained in this area.
Contribution
The study provides new insight into podiatrists' roles and training gaps in identifying and referring melanoma cases.
Findings
67.6% of podiatrists review pigmented lesions.
Only 57.8% feel comfortable contacting a patient’s general practitioner about suspicious lesions.
82.2% of podiatrists report inadequate melanoma training.
Abstract
A significant proportion of melanomas arise on the lower limb, which may present to podiatrists. In this study, two-thirds (67.6%) of podiatrists reported reviewing pigmented lesions, and two-thirds (69.6%) reported identifying a lesion suspicious for melanoma. Only 57.8% of podiatrists felt comfortable contacting their patient’s general practitioner, and most podiatrists (82.2%) felt they received inadequate training in melanoma.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
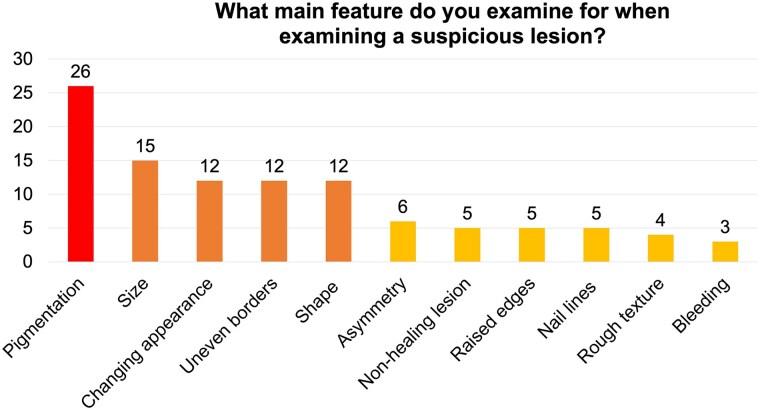 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCutaneous Melanoma Detection and Management · Nail Diseases and Treatments · Forest Insect Ecology and Management
Dear Editor, Melanoma is the fourth most common cancer in the Republic of Ireland, representing 4% of cancers in male patients and 5% in female patients.^1^ The incidence of melanoma is increasing worldwide, credited to earlier detection of thin melanomas.^2^ Nearly 30% of melanomas affect the lower limbs,^3–5^ and melanoma of the foot or toenails can masquerade as ulcers, congealed blood and inflammatory conditions,^6,7^ potentially delaying diagnosis and increasing mortality. Allied healthcare professionals (HCPs) can play a key role in melanoma detection.^8^ We aimed to assess the experience and confidence of podiatrists in diagnosing melanoma of the lower limb.
A 17-question web survey was designed by the authors to assess the demographics, experience and confidence of podiatrists in relation to melanoma of the lower limb. The survey investigated the frequency of presentation of suspicious lesions, the perceived characteristics of suspicious lesions, the current management of suspicious lesions, and suggestions to improved detection of melanoma among podiatrists. The survey was distributed to all members of the Irish Chiropodists/Podiatrists Organisation (ICPO) (Supplementary File S1). The survey was conducted using Google Forms and data were exported to SPSS for analysis.
The survey had a 61.8% response rate (n = 247), with 80.2% (n = 198) having at least 20 years’ experience, with an average of 30 patients seen per week. Two-thirds (67.6%, n = 167) reported being asked to review pigmented lesions, and 41.3% (n = 102) reported frequently examining pigmented lesions. Over two-thirds (69.6%, n = 172) reported identifying a lesion suspicious for melanoma. Of 66 podiatrists who reported the most frequent site where they identified suspicious pigmented lesions, 20% (n = 13) noted the plantar foot to be the most common site, followed by toes and toenails (18%, n = 12 each). Of 105 podiatrists who selected the key feature that they assessed when examining suspicious pigmented lesions, 24.8% (n = 26) assessed pigmentation, 14.3% (n = 15) assessed size, and 11.4% (n = 12 each) assessed evolution, appearance, borders and shape (Figure 1). Of 50 podiatrists who described their routine management of suspicious lesions, 88% (n = 44) advised general practitioner (GP) referral, 8% (n = 4) advised dermatology referral, 2% (n = 1) took a biopsy and 2% (n = 1) took photographs for ‘mole-mapping’. Of 172 podiatrists who reported identifying lesions concerning for melanoma, just 17.4% (n = 30) reported receiving feedback on outcomes from subsequent medical assessment. Only 57.9% (n = 143) of all podiatrists reported feeling comfortable contacting a patient’s GP if they identified a suspicious lesion, only 54.7% (n = 135) reported feeling comfortable discussing photoprotection with patients and only 44.5% (n = 110) felt comfortable discussing tanning or sunbeds. Most podiatrists (82.2%, n = 203) felt they received inadequate training in melanoma during their training. Suggested methods for improving their management of melanoma included undergraduate teaching (12.6%, n = 31), improved referral pathways (3.2%, n = 8), educational seminars (1.6%, n = 4) and direct feedback from GPs/dermatologists regarding outcomes (1.6%, n = 4).
This study shows that most podiatrists have been asked to review pigmented lesions, and that most have identified a lesion that they believed to represent a melanoma. Podiatrists may be the first healthcare providers to review melanoma of the lower limb, given their role as community HCPs, and given pressure on general practice and hospital services. Podiatrists identified a concerning lack of confidence and training in dealing with melanoma of the lower limb. Most podiatrists said that they would advise their patient to attend their GP, and a lack of a direct pathway from podiatrists to GPs or specialty care was highlighted. Moreover, nearly half of podiatrists did not feel comfortable directly contacting a GP to refer a patient. Even fewer had received an update on a patient with a suspicious pigmented lesion after advising review with their GP, a missed opportunity for continuous professional development. In the UK, NICE (National Institute for Health and Care Excellence) guidelines emphasize that lesions suspicious for melanoma should be seen in specialized pigmented lesion clinics within 2 weeks of detection. The referral to a specialist melanoma service may be delayed if the patient does not attend their GP in a timely manner. Many of these patients are older, and may have lower health literacy and be at greater risk of being lost to follow-up if referral mechanisms are convoluted. Health systems in other regions may facilitate direct referrals from podiatry to specialist pigmented lesion clinics.
Strengths of this study include a high response rate from this national professional society and the lack of previous work in this area. Limitations include the lack of outcome data relating to the patients seen by the respondents and the lack of deeper qualitative characterization of surprising findings, such as the discomfort felt around contacting GPs directly.
This research highlights a disconnect in communication between community-based podiatrists, GPs and melanoma services. Avenues for future research or quality improvement include strategies for optimizing management of pigmented lesions in podiatry such as educational seminars or dermoscopy training, improved referral pathways and other policies to enhance detection of melanoma of the lower limb. Podiatrists have a key role in the early identification of melanoma. Dermatologists should support podiatrists with education on assessment and management of suspicious lesions of the lower limb, facilitating timely and efficient referral.
Supplementary Material
vzaf008_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1National Cancer Registry Ireland . Cancer in Ireland 1994-2020: Annual Statistical Report of the National Cancer Registry. Cork, Ireland: NCRI, 2022.
- 2Arnold M, Singh D, Laversanne M et al Global burden of cutaneous melanoma in 2020 and projections to 2040. JAMA Dermatol 2022; 158:495–503.35353115 10.1001/jamadermatol.2022.0160 PMC 8968696 · doi ↗ · pubmed ↗
- 3Piñero-Madrona A, Cerezuela-Fuentes P, Ruiz-Merino G et al Lower limb cutaneous melanoma surgery: location matters. Arch Dermatol Res 2023; 315:1971–8.36862181 10.1007/s 00403-023-02571-z PMC 10366258 · doi ↗ · pubmed ↗
- 4Nam KW, Bae YC, Nam SB et al Characteristics and treatment of cutaneous melanoma of the foot. Arch Plast Surg 2016; 43:59–65.26848447 10.5999/aps.2016.43.1.59PMC 4738130 · doi ↗ · pubmed ↗
- 5Sanlorenzo M, Osella-Abate S, Ribero S et al Melanoma of the lower extremities: foot site is an independent risk factor for clinical outcome. Int J Dermatol 2015; 54:1023–9.25660506 10.1111/ijd.12730 · doi ↗ · pubmed ↗
- 6André J, Moulonguet I, Goettmann-Bonvallot S. In situ amelanotic melanoma of the nail unit mimicking lichen planus: report of 3 cases. Arch Dermatol 2010; 146:418–21.20404232 10.1001/archdermatol.2010.43 · doi ↗ · pubmed ↗
- 7Sondermann W, Zimmer L, Schadendorf D et al Initial misdiagnosis of melanoma located on the foot is associated with poorer prognosis. Medicine (Baltimore) 2016; 95:e 4332.27442685 10.1097/MD.0000000000004332 PMC 5265802 · doi ↗ · pubmed ↗
- 8Quinlan C, Gill R, Murphy M. Increasing melanoma awareness among health and social care professionals in secondary care in an era of reduced skin cancer referrals due to COVID-19. Clin Exp Dermatol 2020; 45:920–1.32485048 10.1111/ced.14323 PMC 9213959 · doi ↗ · pubmed ↗