Co-occurrence of familial cerebral cavernous malformations and tuberculous meningitis
Bonifacio C Pedregosa II, Herminigildo H Gan, Cyrus G Escabillas, Jose C Navarro

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
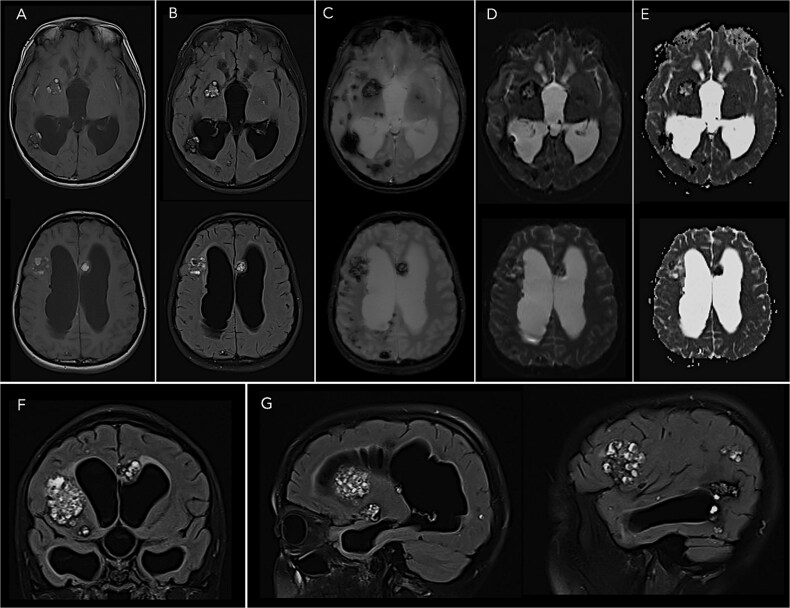 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Malformations Diagnosis and Treatment · Infectious Diseases and Tuberculosis · Spinal Dysraphism and Malformations
A 19-year-old Filipino female presented with generalized tonic–clonic seizures, preceded by a five-week history of progressively worsening holocranial headache accompanied by fever. She was previously well with no known co-morbidities. Neurological examination revealed nuchal rigidity with no other focal deficits. Her father and paternal aunt both had hemorrhagic strokes secondary to cerebral cavernous malformations (CCM).
Biochemical laboratory tests, inflammatory markers, and blood counts were normal. Magnetic resonance imaging demonstrated multiple diffuse CCMs (Fig. 1). Basilar meningeal enhancement and hydrocephalus were also seen. Genetic testing revealed KRIT1 gene mutation, confirming familial CCM. Mycobacterium tuberculosis was recovered from CSF cultures, confirming tuberculous meningitis (TBM). To our knowledge, this is the first report describing familial CCM diagnosed concurrently with TBM.
Characterized by abnormally enlarged capillary cavities without intervening brain parenchyma, CCMs are found in 0.1% to 0.8% of the population [1]. CCMs may occur sporadically as solitary lesions or may be inherited dominantly with incomplete penetrance, usually presenting as multifocal lesions [2]. Familial CCMs constitute 20% of cases and are associated with somatic mutations in one of three CCM genes, with KRIT1 mutations accounting for majority of these cases [2]. CCMs are managed either conservatively or surgically when accessible lesions cause recurrent hemorrhage or seizures [2].
TBM develops when focal tuberculous lesions in communication with the meninges rupture, triggering a dysregulated inflammatory response [3]. In developing countries, TBM is one of the most common causes of subacute to chronic meningitis [3]. Early initiation of antitubercular treatment and corticosteroids increases the likelihood of favorable outcomes; CSF diversion should be considered for progressive hydrocephalus [3, 4].
The patient underwent ventricular drainage and was started on antitubercular agents, corticosteroids, and anti-seizure medications. Her neurological deficits eventually resolved without seizure recurrence. Surveillance neuroimaging revealed regression of hydrocephalus, without any interval change in the size of the CCMs.
Consent
Written informed consent was obtained from the patient for publication of this report and any accompanying images.
Guarantor
Bonifacio C. Pedregosa II, MD.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zafar A, Quadri SA, Farooqui M. et al. Familial cerebral cavernous malformations. Stroke 2019;50:1294–301. 10.1161/STROKEAHA.118.02231430909834 PMC 6924279 · doi ↗ · pubmed ↗
- 2Morrison L, Gutierrez J, Ayata C. et al. Current and future treatment options for cerebral cavernous malformations. Stroke Vasc Interv Neurol 2024;4:e 001140. 10.1161/SVIN.123.001140 · doi ↗
- 3Wilkinson RJ, Rohlwink U, Misra UK. et al. Tuberculous meningitis. Nat Rev Neurol 2017;13:581–98. 10.1038/nrneurol.2017.12028884751 · doi ↗ · pubmed ↗
- 4World Health Organization ed. WHO consolidated guidelines on tuberculosis. Module 4: treatment - drug-susceptible tuberculosis treatment. World Health Organization: Geneva, 2022.35727905 · pubmed ↗