Rowell syndrome following tumor necrosis factor-α (TNF-α) inhibitor therapy
Robin Sia, Maree Micallef

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
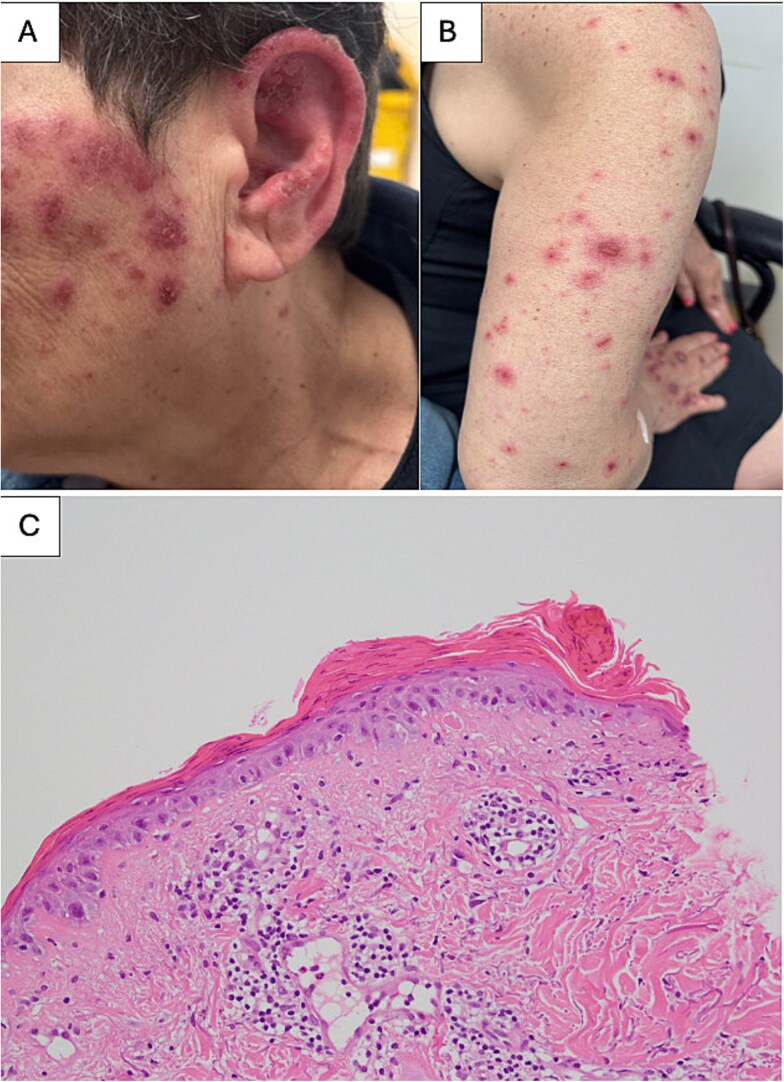 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDrug-Induced Adverse Reactions · Chemotherapy-related skin toxicity · Heparin-Induced Thrombocytopenia and Thrombosis
A 70-year-old woman with long-standing seropositive, nodular rheumatoid arthritis was commenced on adalimumab, a tumor necrosis factor- α (TNF-α) inhibitor for polyarthritis despite treatment with methotrexate and leflunomide. Two weeks later, she developed a widespread non-tender erythematous, scaly, annular and polycyclic rash without oral involvement (Fig. 1A and B).
A skin biopsy showed parakeratosis, attenuated epidermis, apoptotic basal keratinocytes, basal vacuolar change and spongiosis suggestive of acute epidermal necrosis (Fig. 1C). Her rash progressed despite withholding adalimumab. A repeat skin biopsy confirmed a diagnosis of erythema multiforme. Further serology was done and the diagnosis of Rowell syndrome was made based on presence of subacute cutaneous lupus erythematosus erythema multiforme-like lesions supported by positive anti-nuclear antibody (ANA) 1:160 speckled pattern, anti-SS-A/Ro and rheumatoid factor(RF). Her skin lesions responded well to systemic and topical steroid therapy, and she was subsequently started on hydroxychloroquine.
Rowell Syndrome (RS) is a disease characterized by both lupus erythematosus (LE) and erythema multiforme (EM)-like lesions in subjects with a characteristic immunological pattern. Rowell et al. first described a diagnostic criteria for RS which includes presence of discoid lupus erythematosus (DLE) and EM-like lesions, positive RF, speckled ANA and anti-Ro/SS-A positivity [1]. The diagnostic criteria for RS remains unclear to this date with different variants of criteria available including by Lee et al. in 1995, Zeitouni et al. in 2000 and Torchia et al. in 2012 [2–4]. Furthermore, the role of histological findings as part of the diagnostic criteria for RS remains unclear.
This case highlights the possibility of developing Rowell syndrome, an erythema multiforme-variant of cutaneous systemic lupus erythematosus following initiation of TNF-α inhibitors.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rowell NR, Beck JS, Anderson JR. Lupus erythematosus and erythema multiforme-like lesions. Arch Dermatol 1963;88:176–80. 10.1001/archderm.1963.0159020006401214043605 · doi ↗ · pubmed ↗
- 2Lee S, Schloss E, Kowichi J. Rowell’s syndrome: a case report with subacute cutaneous lupus erythematosus and erythema multiforme. Can J Dermatol 1995;7:807–10.
- 3Zeitouni NC, Funaro D, Cloutier RA. et al. Redefining Rowell’s syndrome. Br J Dermatol 2000;142:343–6. 10.1046/j.1365-2133.2000.03306.x 10730772 · doi ↗ · pubmed ↗
- 4Torchia D, Romanelli P, Kerdel FA. Erythema multiforme and Stevens-Johnson syndrome/toxic epidermal necrolysis associated with lupus erythematosus. J Am Acad Dermatol 2012;67:417–21. 10.1016/j.jaad.2011.10.01222101216 · doi ↗ · pubmed ↗