Socioeconomic deprivation is associated with worse in-hospital survival after isolated coronary artery bypass grafting in the UK
Jeremy Chan, Pradeep Narayan, Jacie Jiaqi Law, Tim Dong, Gianni D Angelini

TL;DR
In the UK, people from poorer areas have slightly worse survival rates after heart surgery, despite universal healthcare.
Contribution
This study shows that socioeconomic deprivation affects CABG outcomes in a universal healthcare system.
Findings
Patients from the most deprived areas had higher comorbidity rates and urgent surgery rates.
In-hospital mortality was slightly higher in more deprived groups.
Income and education deprivation were most strongly linked to survival outcomes.
Abstract
Previous studies have identified a correlation between socioeconomic deprivation and poorer outcomes following cardiac surgery in the USA, where healthcare is predominantly delivered through private system. However, the influence of socioeconomic deprivation in countries with universal healthcare systems, such as the UK, has been less extensively investigated. Therefore, we used the index of multiple deprivation (IMD) to evaluate the impact of socioeconomic status on early clinical outcomes following coronary artery bypass grafting (CABG) in the UK. All patients who underwent elective/urgent isolated CABG between 2008 and 2019 in the UK were included. The IMD, along with other perioperative characteristics, were incorporated into a regression model to determine factors associated with in-hospital mortality. The analysis included 182 911 patients (median age: 67.3 years, 82.13% male).…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
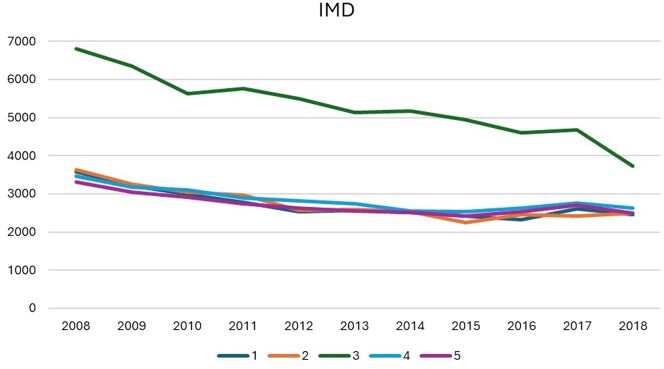 Figure 1
Figure 1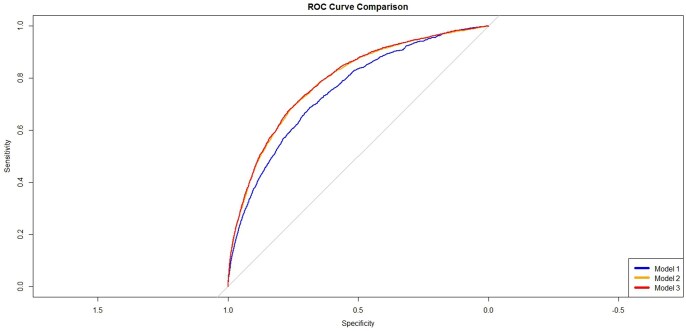 Figure 2
Figure 2| Overall | 1 | 2 | 3 | 4 | 5 |
| |
|---|---|---|---|---|---|---|---|
| On pump | 149 840 (85.00%) | 25 708 (86.72%) | 25 752 (86.73%) | 48 372 (84.37%) | 25 877 (84.53%) | 24 131 (83.24%) | <0.001 |
| XClamp time (mins) (median, IQR) | 47.00 (33.00, 62.00) | 47.00 (33.00, 62.00) | 45.00 (32.00, 60.00) | 49.00 (36.00, 65.00) | 45.00 (32.00, 60.00) | 45.00 (31.00, 61.00) | <0.001 |
| Bypass time (mins) (median, IQR) | 80.00 (60.00, 101.00) | 80.00 (60.00, 101.00) | 79.00 (58.00, 99.00) | 84.00 (63.00 , 105.00) | 78.00 (58.00, 99.00) | 78.00 (57.00, 100.00) | <0.001 |
| Number of grafts (median, IQR) | 3.00 (2.00 , 3.00) | 3.00 (2.00 , 3.00) | 3.00 (2.00 , 3.00) | 3.00 (2.00 , 4.00) | 3.00 (2.00 , 3.00) | 3.00 (2.00 , 3.00) | <0.001 |
| TLOS | 8.00 (6.00 , 13.00) | 9.00 (7.00 , 14.00) | 8.00 (6.00 , 13.00) | 8.00 (7.00 , 13.00) | 8.00 (6.00 , 12.00) | 8.00 (6.00 , 12.00) | <0.001 |
| Multiple arterial grafts | 22 793 (12.46%) | 3059 (10.01%) | 3283 (10.65%) | 8967 (15.16%) | 3742 (11.73%) | 3742 (12.28%) | <0.001 |
| In-hospital mortality | 2246 (1.23%) | 397 (1.30%) | 401 (1.30%) | 734 (1.24%) | 362 (1.14%) | 352 (1.15%) | <0.001 |
| Return to theatre | 6695 (3.91%) | 1194 (4.15%) | 1177 (4.13%) | 2037 (3.73%) | 1186 (3.93%) | 1101 (3.80%) | 0.008 |
| CVA | 0.072 | ||||||
| TIA | 640 (0.39%) | 111 (0.39%) | 102 (0.37%) | 181 (0.34%) | 128 (0.45%) | 118 (0.43%) | |
| Stroke | 863 (0.52%) | 157 (0.56%) | 154 (0.55%) | 285 (0.53%) | 152 (0.53%) | 115 (0.42%) | |
| Postoperative dialysis | 3182 (1.90%) | 581 (2.04%) | 578 (2.04%) | 1067 (1.97%) | 508 (1.74%) | 448 (1.61%) | <0.001 |
| Deep sternal wound infection | 907 (1.02%) | 154 (0.96%) | 148 (1.01%) | 317 (1.18%) | 159 (1.00%) | 129 (0.83%) | 0.009 |
| Mortality | |||
|---|---|---|---|
| Characteristics | Odds ratios | 95% CI |
|
| Age | 1.07 | 1.07–1.08 | <0.001 |
| Sex | |||
| Male | |||
| Female | 1.55 | 1.40–1.70 | <0.001 |
| BMI | 0.99 | 0.98–1.00 | 0.10 |
| Left ventricular function | |||
| Very poor (≤ 20%) | |||
| Poor (21–30%) | 0.43 | 0.22–0.93 | 0.02 |
| Moderate (31–49%) | 0.30 | 0.15–0.68 | 0.002 |
| Good (>50%) | 0.22 | 0.11–0.49 | <0.001 |
| Operative urgency | |||
| Elective | |||
| Urgent | 1.41 | 1.27–1.57 | <0.001 |
| Diabetes | |||
| Non-diabetic | |||
| Diet control | 1.36 | 1.12–1.62 | 0.001 |
| Medication | 1.09 | 0.97–1.22 | 0.13 |
| Insulin use | 1.75 | 1.53–1.99 | <0.001 |
| Smoking | |||
| Non-smoker | |||
| Ex-smoker | 1.01 | 0.92–1.12 | 0.79 |
| Current smoker | 1.17 | 1.00–1.36 | 0.05 |
| History of pulmonary disease | 1.36 | 1.22–1.52 | <0.001 |
| Peripheral vascular disease | 1.73 | 1.56–1.91 | <0.001 |
| Preoperative atrial fibrillation | 1.57 | 1.35–1.83 | <0.001 |
| Neurological dysfunction preoperatively | 0.84 | 0.49–1.50 | 0.53 |
| CCS angina grade | |||
| 0 | |||
| 1 | 0.78 | 0.64–0.96 | 0.02 |
| 2 | 0.74 | 0.64–0.86 | <0.001 |
| 3 | 0.92 | 0.79–1.07 | 0.26 |
| 4 | 1.00 | 0.85–1.19 | 0.97 |
| NYHA status | |||
| 1 | |||
| 2 | 1.16 | 1.03–1.31 | 0.02 |
| 3 | 1.52 | 1.33–1.74 | <0.001 |
| 4 | 2.28 | 1.88–2.77 | <0.001 |
| PCI | |||
| No previous PCI | |||
| PCI < 24 hours before surgery | 1.59 | 0.84–2.72 | 0.12 |
| PCI > 24 hours before surgery; same admission | 1.02 | 0.72–1.40 | 0.90 |
| PCI > 24 hours before surgery; previous admission | 0.94 | 0.82–1.08 | 0.389 |
| Previous MI | |||
| None | |||
| One | 1.28 | 1.13–1.44 | <0.001 |
| Two or more | 1.68 | 1.43–1.98 | <0.001 |
| Poor mobility | 1.42 | 0.82–2.31 | 0.18 |
| The interval between MI and surgery | |||
| No previous MI | |||
| MI < 6 hours | 0.52 | 0.08–1.72 | 0.37 |
| MI 6–24 hours | 1.15 | 0.72–1.73 | 0.54 |
| MI 1–30 days | 0.85 | 0.74–0.97 | 0.02 |
| MI 31–90 days | 1.16 | 0.98–1.37 | 0.09 |
| Ventilation preoperatively | 1.19 | 1.03–1.65 | 0.03 |
| Cardiogenic shock preoperatively | 2.17 | 1.48–3.10 | <0.001 |
| Inotropes used preoperatively | 2.74 | 1.95–3.76 | <0.001 |
| Income deprivation | |||
| 1 | |||
| 2 | 0.8 | 0.64–0.99 | 0.04 |
| 3 | 0.62 | 0.47–0.82 | 0.001 |
| 4 | 0.46 | 0.33–0.64 | <0.001 |
| 5 | 0.48 | 0.33–0.69 | <0.001 |
| Employment deprivation | |||
| 1 | |||
| 2 | 0.96 | 0.77–1.20 | 0.71 |
| 3 | 1.09 | 0.82–1.46 | 0.56 |
| 4 | 1.14 | 0.82–1.60 | 0.43 |
| 5 | 1.14 | 0.78–1.68 | 0.50 |
| Education, skills and training deprivation | |||
| 1 | |||
| 2 | 0.99 | 0.85–1.21 | 0.88 |
| 3 | 0.63 | 0.34–0.88 | 0.002 |
| 4 | 0.57 | 0.21–0.85 | 0.001 |
| 5 | 0.44 | 0.01–0.77 | <0.001 |
| Health deprivation | |||
| 1 | |||
| 2 | 1.15 | 0.96–1.38 | 0.13 |
| 3 | 1.17 | 0.94–1.45 | 0.15 |
| 4 | 1.11 | 0.87–1.41 | 0.40 |
| 5 | 1.1 | 0.84–1.45 | 0.48 |
| Crime | |||
| 1 | |||
| 2 | 0.95 | 0.81–1.11 | 0.51 |
| 3 | 0.92 | 0.79–1.09 | 0.34 |
| 4 | 1.1 | 0.93–1.31 | 0.25 |
| 5 | 0.93 | 0.77–1.12 | 0.44 |
| Barriers to housing | |||
| 1 | |||
| 2 | 1.02 | 0.88–1.19 | 0.78 |
| 3 | 0.94 | 0.81–1.10 | 0.44 |
| 4 | 0.92 | 0.78–1.07 | 0.29 |
| 5 | 0.92 | 0.78–1.07 | 0.29 |
| Services and living environment deprivation | |||
| 1 | |||
| 2 | 1.2 | 1.03–1.39 | 0.02 |
| 3 | 1.16 | 1.00–1.35 | 0.05 |
| 4 | 1.15 | 0.98–1.36 | 0.08 |
| 5 | 1.13 | 0.96–1.33 | 0.15 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Health and Mental Health · Primary Care and Health Outcomes · Geriatric Care and Nursing Homes
INTRODUCTION
Socioeconomic deprivation, also known as socioeconomic distress, has been reported to increase the incidence of perioperative complications, short- and long-term mortality, readmission rate and failure to rescue in cardiac surgery [1–7]. However, there is no universally agreed definition of socioeconomic deprivation, and the specific components included can vary across nations [8]. Existing research also employs diverse definitions when reporting their findings. In addition, there are few contemporary data examining the implication of socioeconomic deprivation on coronary artery bypass grafting (CABG) outcomes from the UK, with most studies originating from the USA, which is a predominantly private healthcare system. Consequently, the findings may not be directly applicable to the UK or European context, where universal public healthcare systems are more common.
The index of multiple deprivation (IMD) is the official measure used by the UK government to assess relative levels of deprivation across the general population residing in small areas of the nation, which are termed low-layer super output areas (LSOA). Each LSOA is scored, with an average population of 1500, ranked based on its weighted summary of 7 key domains. This seven distinct domains includes income deprivation (22.5%), employment deprivation (22.5%), education, skills and training deprivation (13.5%), health deprivation (13.5%), crime (9.3%), barriers to housing (9.3%) and services and living environment deprivation (9.3%). The IMD ranks every small area from 1, indicating the most deprived area, to 32 844, denoting the least deprived area. This is further divided into 10 equal deciles, with decile 1 representing the 10% most deprived area and decile 10 denoting the 10% least deprived area. Deprivation deciles are then further subdivided into five IMD-based deprivation groups, with group 1 encompassing decile 1 and 2, while group 5 includes decile 9 or 10 [9].
Coronary artery disease is strongly associated with major modifiable risk factors such as poorly controlled diabetes, hypertension, smoking and hyperlipidemia. These risk factors are disproportionately prevalent among socioeconomically deprived populations. Utilizing the IMD, we sought to determine if socioeconomic status (SES) is associated with a higher prevalence of modifiable risk factors, poorer in-hospital survival and early clinical outcomes following CABG in the UK. If SES was identified as a significant factor associated to the clinical outcome of interest, this paper will embark on its secondary objectives by examining if the incorporation of SES to EuroScore II would enhance in-hospital mortality risk prediction after cardiac surgery.
METHODS
All patients who underwent elective or urgent isolated CABG from April 2008 to April 2019 were extracted from the National Adult Cardiac Surgery Audit (NACSA) database. The NACSA database prospectively collects data on all major heart operations carried out on National Health Service patients in the UK since April 1996. The definitions of database variables used and a description of the database were previously reported [10]. Essentially, data were imputed by healthcare professionals (surgeons, nurses, anaesthetists and perfusionists) by individual hospitals and then submitted to the NACSA central database. Patients who underwent emergency or salvage CABG, non-isolated CABG and had previous cardiac surgery were excluded to avoid introducing significant variability due to a small subset of the population and distinctive risk factors that do not represent the broader population who had undergone a planned procedure and allow a more homogenous cohort.
The seven domains in the IMD were divided into deciles, with 1 being the most deprived and 5 representing the least. The trend, hospital mortality and short-term clinical outcomes were evaluated against EuroScore II. SES, alongside EuroScore II variables, was input into a logistic regression model to assess the association between in-hospital mortality and socioeconomic deprivation.
SES, alongside EuroScore II variables, was input into logistic regression models to evaluate if it improves model performance. We compared the predictive performance of several models for in-hospital survival. The baseline model (Model 1) used the EuroScore II value. Subsequent models incorporated additional variables: Model 2 included all EuroScore II variables, and Model 3 included Model 2 with the addition of individual IMD components (income, employment, education, health, crime, housing and living environment).
Ethical statement
The study was part of a research project approved by the Health Research Authority and Health and Care Research Wales. As the study included retrospective interrogation of the NICOR database, the need for individual patient consent was waived off (Health and Care Research Wales) (IRAS ID: 278171) in accordance with the research guidance. The study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments.
Statistical analysis
Continuous variables are reported as mean and SD or median and IQR, pending the normality of the data. Categorical variables are reported as frequencies and percentages. The normality of the distribution of continuous data was assessed using the Shapiro–Wilk test.
The parametric analysis of variance (ANOVA) test was used to compare two or more independent normally distributed samples with the Kruskal–Wallis test used as a non-parametric counterpart. Tukey’s Honest Significant Difference test was further performed to control the family-wise error rate when multiple comparisons were performed to identify sub-groups with significant differences. The chi-square test of independence was used for categorical data with pairwise comparisons of proportions using the pairwise proportion test if the results were significant. Bonferroni correction was then applied after multiple pairwise comparisons. Multivariable logistic regression modelling was performed to examine the association between socioeconomic deprivation and in-hospital mortality among patients undergoing CABG. The model was adjusted for other key covariates included in the EuroScore II risk model, such as age, gender, renal function, diabetes and the New York Heart Association (NYHA) class (Table 1) as well as the individual seven components of the IMD. Results are demonstrated as odds ratio (OR) and 95% confidence interval (CI).
To assess whether adding SES improves the performance of the logistic regression model, we plotted a receiver operating characteristic (ROC) curve for each model and compared prediction performance using the area under the curve (AUC). CIs for the AUC were calculated using the DeLong method. R (Version 4.2.3, R Foundation for Statistical Computing, Vienna, Austria) and R Studio (Version 1.4.1103, RStudio, PBC) were used for statistical analysis. Graphs and tables were created using R Studio (Version 1.4.1103, RStudio, PBC) and Microsoft Office 365 (Version 16.0.14026). A P-value of <0.05 is deemed statistically significant.
RESULTS
A total of 182 911 patients (median age 67.3, 82.13% male) were included in the analysis, with 30 564, 30 815, 59 161, 31 891 and 30 480 patients categorized into IMD-based deprivation groups 1, 2, 3, 4 and 5, respectively. The patients’ characteristics are reported in Supplementary Material, Table S1. The number of isolated CABG procedures decreased from 20 777 in 2008 to 13 806 in 2018, with a notable decline in the group 3, where cases fell by 41.18% from 6355 annually. Conversely, the annual number of patients in IMD-based deprivation groups 1, 2, 4 and 5 remained relatively stable, ranging between 2500 and 3500 (Fig. 1).
The number of patients in the 5 IMD-based deprivation groups index (1, 2, 3, 4, 5) of multiple deprivation groups who underwent isolated coronary artery bypass grafting in the UK from 2008–18.
The receiver operating characteristics curve of the 3 models (Model 1: EuroScore II value, Model 2: EuroScore II characteristics, Model 3: Model 2 with individual 7 index of multiple deprivation components.).
The prevalence of urgent surgeries was higher in group 1, with 43.97% compared to 38.55% in group 5 (P < 0.001). Group 1 compared to group 5 also exhibited higher rates of chronic pulmonary disease requiring long-term medication (15.92% vs 9.03%), current smoking prevalence (20.93% vs 6.62%), diabetes management on insulin therapy (10.05% vs 6.10%) and median BMI higher (28.40 vs 27.94, P < 0.001). Additionally, 5.76% of patients in group 1 had a history of stroke, compared to 2.43% in group 5 and a history of myocardial infarction 11.82% vs 6.71% (both, P < 0.001). It is worth noting that the proportion of females who underwent surgical revascularization reduces as SES improves.
Overall in-hospital mortality was 1.23%, and the rates across IMD-based deprivation groups were 1.30% for group 1, 1.30% for group 2, 1.24% for group 3, 1.14% for group 4 and 1.15% for group 5 (P < 0.001). The in-hospital mortality rate decreased as SES improved. In addition, more cases were performed using an off-pump technique as the SES improved. Table 1 outlines the intra- and postoperative characteristics of patients in each IMD-based deprivation groups who underwent isolated CABG during the study period.
Factors associated with in-hospital mortality
Several preoperative characteristics were associated with higher in-hospital mortality after isolated CABG. This includes (but not limited to) age (OR 1.07, 95% CI: 1.07–1.08, P < 0.001), female sex (OR 1.55, 95% CI: 1.40–1.70, P < 0.001), urgent operation (OR 1.41, 95% CI: 1.27–1.57, P < 0.001), diet control diabetes (OR 1.36, 95% CI: 1.12–1.62, P = 0.001) and preoperative atrial fibrillation (OR 1.57, 95% CI: 1.35–1.83, P < 0.001).
In terms of association between socioeconomic deprivation and in-hospital mortality, improvements in deprivation related to income were associated with a 20% reduction in odds of in-hospital mortality following isolated CABG in group 2 (OR 0.80, 95% CI: 0.64–0.99, P = 0.038), group 3 (OR 0.62, 95% CI: 0.47–0.82, P = 0.001), group 4 (OR 0.46, 95% CI: 0.33–0.64, P < 0.001) and group 5 (OR 0.48, 95% CI: 0.33–0.69, P < 0.001). Similarly, higher education levels were also linked to a 37% reduction in odds of in-hospital mortality in group 3 (OR 0.63, 95% CI: 0.34–0.88, P = 0.002), group 4 (OR 0.57, 95% CI: 0.21–0.85, P = 0.001) and group 5 (OR 0.44, 95% CI: 0.01–0.77, P < 0.001) (Table 2).
Model performance with IMD
The AUC for models 1, 2 and 3 was 0.749 (95% CI: 0.739–0.759), 0.786 (95% CI: 0.777–0.796) and 0.789 (95% CI: 0.779–0.799), respectively. There was a small improvement in model performance between models 1,2, and 3. Figure 2 shows the ROC curve including all three models.
DISCUSSION
Our results demonstrated that socioeconomic deprivation, particularly income and education deprivation, was associated with a small increase in in-hospital survival after elective/urgent, first-time, isolated CABG in the UK. The small percentage difference may look clinically irrelevant, but in the context of a large dataset, it equated to many more patients who did not survive the procedure (50 patients between IMD 1 and IMD 5).
Patients from the most socioeconomically deprived areas (Group 1) exhibited markedly higher rates of comorbidities and risk factors, including chronic pulmonary disease, active smoking, insulin-dependent diabetes, elevated BMI and a history of stroke. In addition, these patients also presented more frequently with catastrophic events like acute myocardial infarction and required urgent surgical intervention more frequently than their counterparts from less deprived areas. Notably, our study demonstrated that most patients receiving elective isolated CABG belonged to group 3, with fairly proportionate patient contribution from other IMD-based deprivation groups. Studies have shown that while the incidence and prevalence of cardiovascular disease are higher in greater deprivation groups, access to elective cardiac surgery is associated with less deprived groups. Our study also found that incorporating socioeconomic factors into the predictive model further improved its performance in predicting in-hospital mortality following CABG.
The IMD
The IMD has gained widespread acceptance and is frequently employed to report socioeconomic deprivation across various surgical specialities in the UK. Its comprehensive nature makes it a valuable tool for understanding the multifaceted aspects of deprivation that may impact health outcomes [11, 12].
A similar index, known as the distressed communities index (DCI), has been increasingly used in evaluating economic disparities in the USA. This index consisted of seven components, including no high school diploma, housing vacancy rate, adults not working, poverty rate, median income ratio, changes in employment and changes in establishments. Cities and states were then classified into five tiers of well-being. The DCI has been demonstrated to be an effective tool in predicting survival and clinical outcomes after cardiac surgical and transcatheter procedures [2, 13, 14]. However, the DCI differs from the IMD in its focus and composition. While the DCI primarily emphasizes economic well-being, it does not explicitly incorporate health and living environment factors into its assessment as in the IMD.
Socioeconomic deprivation in patients who underwent isolated CABG
SES comprises a range of factors that can vary significantly across different regions and cultural contexts [15, 16]. In developed countries, four key factors: income, education, employment status and environmental conditions have been consistently shown to be associated with cardiovascular diseases [8]. Our findings align with this trend, indicating that deprivation in both income and education is associated with poorer in-hospital outcomes following surgical revascularization in the UK. Areas with lower-income residents are significant predictors of 30-day mortality following CABG. Additionally, patients hailing from more deprived backgrounds often experience higher burdens of comorbidity and a greater likelihood of undergoing urgent surgeries.
Utilizing data from the US Nationwide Readmissions Database, a study has revealed that lower-income residential areas are significant predictors of 30-day mortality after CABG. Furthermore, similar to our study, patients hailing from more deprived backgrounds often experience higher burdens of comorbidity and a greater likelihood of undergoing urgent surgeries. Socioeconomic deprivation has also been associated with diminished preoperative quality of life [17], increased postoperative length of stay [6] and a reduction in access to cardiac surgery during the COVID-19 pandemic [2].
Although much of the existing (and the above) literature originates from the USA, where healthcare is largely private, the presence of publicly funded healthcare systems in Europe does not negate the existence of socioeconomic disadvantages. For example, a study conducted in 2000 in Italy found that the most socioeconomically disadvantaged groups faced higher 30-day mortality rates compared to those from more affluent backgrounds. This study underscored that universal health coverage does not automatically ensure equitable access to CABG [18]. Similarly, reports from the late 2000s in the UK revealed that lower SES was linked to poorer early outcomes following isolated CABG, as demonstrated by a single-centre study in northeastern Scotland [19]. Lai et al. found that female patients, black individuals and those from the most deprived areas had lower access to CABG and higher postoperative mortality [20]. Benedetto et al. further illustrated that payer status impacts hospital outcomes, highlighting persistent disparities even in countries with publicly funded healthcare systems, such as the UK [21]. Lastly, Dalen and colleagues have demonstrated a strong inverse association between income and mortality following cardiac surgery in Sweden [22].
While our report mainly addresses in-hospital outcomes, SES also affects long-term survival following isolated CABG. Pagano et al. tracked 44 902 adults who underwent cardiac surgery from 1997 to 2007 and identified social deprivation as a significant independent predictor of increased long-term mortality risk [23]. Similarly, Barnard et al. found that social deprivation correlates with reduced mid-term survival [24]. Long-term disparities may reflect ongoing challenges in achieving equity in healthcare delivery, despite advances in medical and surgical care. Future research should continue to explore these long-term outcomes and the underlying factors contributing to socioeconomic disparities in patients undergoing surgical revascularization.
Limitations
Our study has several limitations. First and foremost, the use of the IMD to assess relative deprivation is designed to measure disparities at the area level, which may not accurately reflect individual circumstances. As a result, conclusions drawn at the neighbourhood level may not fully translate to the experiences of individuals within those areas. Second, the IMD is updated periodically rather than continuously. As a result, it may not capture recent changes in deprivation levels, potentially leading to a lag between actual socioeconomic conditions and those represented in our data. However, the highest proportions of neighbourhoods among the most deprived in England have remained largely consistent between the previous and the current IMD results [25] and largely mitigates concerns about the temporal limitations. Our findings are based on the UK healthcare system only, and this limits the generalizability of our results to other healthcare systems or countries with different measures of SES. Results may not be the same using our same methodology in other healthcare datasets. Lastly, accessibility to health care, including readmission after surgery as well as primary care utilization and long-term outcomes such as repeat revascularization, stroke and long-term survival, are not available from the national dataset we used, which limits the ability to assess the full impact of socioeconomic deprivation and other variables on patient outcomes.
CONCLUSION
Socioeconomic deprivation, particularly related to income and education, is associated with a small decrease in in-hospital survival outcomes following isolated CABG. Furthermore, patients from more deprived backgrounds experience higher burdens of comorbidity and a greater likelihood of requiring urgent surgery. These findings underscore the critical need to address socioeconomic disparities in healthcare to improve outcomes for all patients. Ensuring equitable access to care and resources, regardless of SES, is essential for enhancing the effectiveness of surgical interventions.
Supplementary Material
ivaf119_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hoyler MM , Feng TR, Ma X et al Insurance status and socioeconomic factors affect early mortality after cardiac valve surgery. J Cardiothorac Vasc Anesth 2020;34:3234–42.32417005 10.1053/j.jvca.2020.03.044 · doi ↗ · pubmed ↗
- 2Kaplan EF , Strobel RJ, Young AM et al Cardiac surgery outcomes during the COVID-19 pandemic worsened across all socioeconomic statuses. Ann Thorac Surg 2023;115:1511–8.36696937 10.1016/j.athoracsur.2022.12.042PMC 9867828 · doi ↗ · pubmed ↗
- 3Kobayashi J , Kusachi S, Sawa Y et al Socioeconomic effects of surgical site infection after cardiac surgery in Japan. Surg Today 2015;45:422–8.24973059 10.1007/s 00595-014-0969-2 · doi ↗ · pubmed ↗
- 4Koch CG , Li L, Kaplan GA et al Socioeconomic position, not race, is linked to death after cardiac surgery. Circ Cardiovasc Qual Outcomes 2010;3:267–76.20371761 10.1161/CIRCOUTCOMES.109.880377 · doi ↗ · pubmed ↗
- 5Lachonius M , Giang KW, Lindgren M et al Socioeconomic factors and long-term mortality risk after surgical aortic valve replacement. Int J Cardiol Cardiovasc Risk Prev 2023;19:200223.38023350 10.1016/j.ijcrp.2023.200223 PMC 10661603 · doi ↗ · pubmed ↗
- 6Mc Leish T , Seadler BD, Parrado R, Rein L, Joyce DL. The effect of socioeconomic factors on patient outcomes in cardiac surgery. J Card Surg 2022;37:5135–43.36403269 10.1111/jocs.17229 · doi ↗ · pubmed ↗
- 7Strobel RJ , Kaplan EF, Young AM et al; Investigators for the Virginia Cardiac Services Quality Initiative. Socioeconomic distress is associated with failure to rescue in cardiac surgery. J Thorac Cardiovasc Surg 2024;167:1100–14 e 1.36031426 10.1016/j.jtcvs.2022.07.013PMC 9852359 · doi ↗ · pubmed ↗
- 8Schultz WM , Kelli HM, Lisko JC et al Socioeconomic status and cardiovascular outcomes: challenges and interventions. Circulation 2018;137:2166–78.29760227 10.1161/CIRCULATIONAHA.117.029652 PMC 5958918 · doi ↗ · pubmed ↗