Sex differences based on the timing of invasive management among patients with non-ST-elevation acute coronary syndrome: an individual patient data meta-analysis
Graziella Pompei, Gregory B Mills, Christos P Kotanidis, Shamir Mehta, Denise Tiong, Erik A Badings, Thomas Engstrøm, Arnoud W J van‘t Hof, Dan Høfsten, Lene Holmvang, Alexander Jobs, Lars Køber, Dejan Milasinovic, Aleksandra Milosevic, Goran Stankovic, Holger Thiele

TL;DR
This study finds no significant sex differences in outcomes for heart patients treated with early or delayed invasive strategies.
Contribution
The study is the first to investigate sex differences in outcomes of NSTE-ACS patients based on timing of invasive management using individual patient data meta-analysis.
Findings
No sex differences in the composite endpoint of death or MI with early invasive strategy.
Delayed invasive strategy showed higher risk of recurrent ischaemia and bleeding in females in univariable analysis.
Multivariable analysis did not confirm sex differences in outcomes for delayed invasive strategy.
Abstract
Studies investigating the timing of coronary angiography in non-ST-elevation acute coronary syndrome (NSTE-ACS) have not evaluated sex differences. This study aims to investigate the sex-related differences in outcomes of NSTE-ACS patients undergoing early or delayed invasive management. An individual patient data (IPD) meta-analysis was performed after systematic review of randomized controlled trials (RCTs) comparing early vs. delayed invasive strategy among NSTE-ACS patients. The primary endpoint was a composite of all-cause death or myocardial infarction (MI) at 6 months. Secondary endpoints included all-cause death, MI, recurrent ischaemia, stroke, and major bleeding. One-stage, random-effects Cox models were conducted. This meta-analysis was registered with PROSPERO (CRD42023468604). Six RCTs including 6654 patients were identified, of whom 2257 (33.9%) were females with a median…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
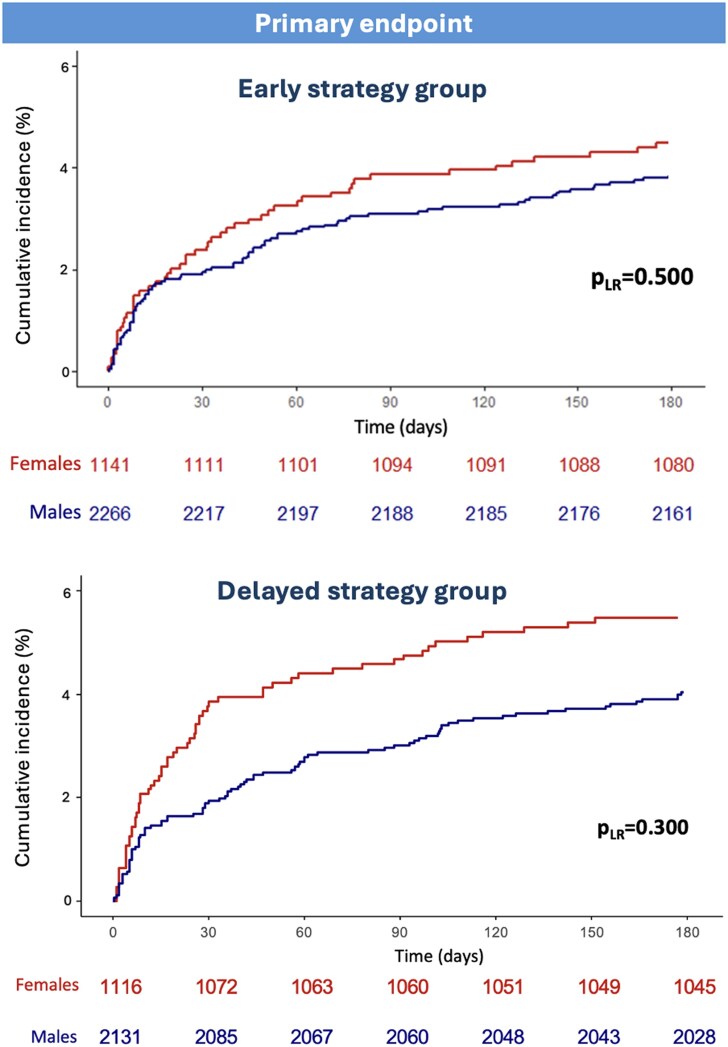 Figure 1
Figure 1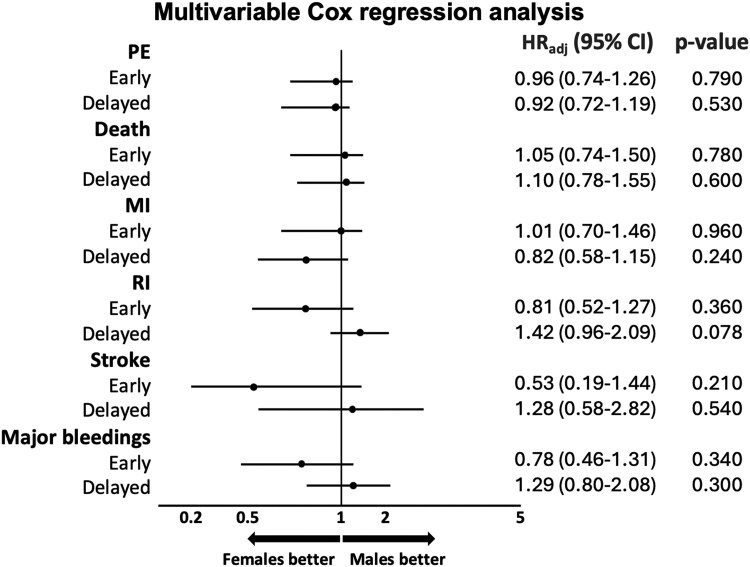 Figure 2
Figure 2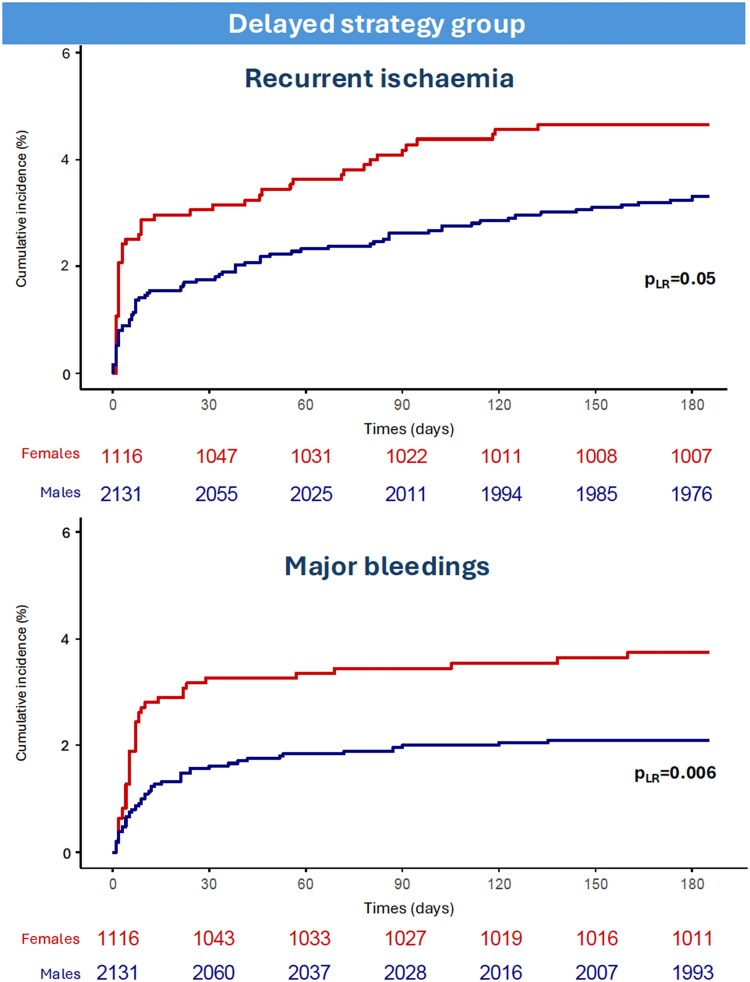 Figure 3
Figure 3| Study | Patients | Invasive strategy timing | Primary endpoint | Secondary endpoints | Non-fatal MI | Recurrent ischaemia | Bleeding |
|---|---|---|---|---|---|---|---|
| ELISA |
|
| Enzymatic infarct size | Death and recurrent MI at 30 days |
| Requirement for repeat angiography and subsequent repeat TLR |
|
| TIMACS |
|
| First occurrence of composite of death, new MI, or stroke at 6 months | First occurrence of composite of death, MI, or refractory ischaemia and the composite of death, MI, stroke, refractory ischaemia, or repeat intervention at 6 months |
|
|
Fatal bleed Symptomatic intracranial bleed Retroperitoneal bleed Intraocular bleed leading to significant vision loss Decrease in Hb ≥ 3.0 g/dL Bleed requiring transfusion of 2 or more RBCs units or equivalent of whole blood Bleeding requiring surgical intervention |
| LIPSIA-NSTEMI |
|
| CK-MB activity during index hospitalization for each patient. In addition, the infarct size was estimated based on the AUC of CK-MB release | Composite of (i) death and non-fatal MI; (ii) death, non-fatal MI, and refractory ischaemia; and (iii) death, non-fatal MI, refractory ischaemia, and rehospitalization for UA within 6 months |
new Q-waves in ≥2 contiguous leads plus ischaemic symptoms >20 min new ST ↑ in ≥2 contiguous leads plus symptoms >20 min; or ↑ CK-MB >5 ULN. In patients with CK-MB >5 ULN at randomization an increase >50% was required |
|
|
| ELISA-3 |
|
| Combined incidence of all-cause death, reinfarction and/or recurrent ischaemia at 30 days | Enzymatic infarct size assessed by cardiac Tn T (72–96 h after admission or at discharge) per cent of patients without a rise in CK-MB during admission |
| Recurrent chest pain associated with new/recurrent ECG changes requiring urgent or repeat angiography or repeat hospitalization |
|
|
| |||||||
| Badings | Immediate group: | ||||||
| Delayed group: |
| ||||||
|
| |||||||
| Bleeding complications | |||||||
|
| |||||||
| RIDDLE-NSTEMI |
|
| Composite of all-cause death or new MI at 30 days | Combined incidence of death, new MI, and/or recurrent ischaemia at 30 days and 1 year, as well as death or new MI at 1 year |
|
Patient on OMT ECG changes indicative of ongoing ischaemia Required invasive intervention |
|
| Milosevic | Immediate-intervention group: | ||||||
|
| |||||||
| Delayed intervention group: |
| ||||||
| Individual components of the primary and secondary endpoints and major bleedings at 30 days and 1 year |
| ||||||
|
| |||||||
| VERDICT |
|
| Combination of all-cause death, non-fatal recurrent MI, hospital admission for refractory myocardial ischaemia or HF | Invasive procedure complications during index hospitalisation (death, bleeding by the BARC criteria, non-fatal acute MI, stroke, or TIA) in addition to the occurrence of each of the following at any time: death, non-fatal acute MI, admission for refractory myocardial ischaemia, repeat coronary revascularization, or admission for HF | Occurrence of any of the following 3: ↑ and/or ↓ of cardiac biomarkers with at least 1 value >99th percentile ULN (if ↑ biomarkers at baseline, a further ↑ ≥20% is required and the peak value must exceed the previously stated limit), plus the evidence of ischaemia from at least 1 of the following: Symptoms of ischaemia ECG changes in two contiguous leads New Q-waves in two contiguous ECG leads Evidence of a new loss of viable myocardium or wall motion abnormality Sudden/unexpected cardiac death, involving cardiac arrest, often with symptoms suggestive of myocardial ischaemia, but occurring before blood samples could be obtained, or at a time before the appearance of biomarkers in the blood and accompanied by: Presumably new ST ↑ New LBBB Evidence of fresh thrombus Pathological findings of a MI |
| |
| Kofoed | Very early group: | ||||||
| Standard group: |
| ||||||
|
|
| Variables | Female patients | Male patients |
|
|---|---|---|---|
|
|
| ||
| Demographic data and clinical measures | |||
| Age, years [IQR] | 69 [60, 76] | 64.5 [55, 72.1] | <0.001 |
| BMI, kg m−2[IQR] | 26.1 [23.4, 29.4] | 26.9 [24.6, 29.8] | <0.001 |
| GRACE score [IQR] | 136 [117, 157] | 131 [113, 151] | <0.001 |
| HR [IQR] | 78 [68, 90] | 75 [65, 87] | <0.001 |
| Systolic BP, mmHg [IQR] | 141 [127, 160] | 140 [125, 157] | 0.009 |
| Creatinine, µmol/L [IQR] | 67 [58, 80] | 83 [72, 96] | <0.001 |
| Past medical history | |||
| Former or current smoking, (%) | 489 (21.7) | 1504 (34.2) | <0.001 |
| Missing data, (%) | 0 (0.0) | 3 (0.1) | |
| Previous MI, (%) | 328 (14.5) | 903 (20.5) | <0.001 |
| Previous CABG, (%) | 100 (4.4) | 371 (8.4) | <0.001 |
| Previous PCI, (%) | 255 (11.3) | 743 (16.9) | <0.001 |
| Missing data, (%) | 1 (0.0) | 3 (0.1) | |
| Previous stroke, | 144 (6.4) | 307 (7.0) | 0.448 |
| Missing data, (%) | 128 (5.7) | 271 (6.2) | |
| Hypertension, | 1535 (68.0) | 2607 (59.3) | <0.001 |
| Missing data, (%) | 1 (0.0) | 3 (0.1) | |
| Diabetes mellitus, | 615 (27.2) | 931 (21.2) | <0.001 |
| Medical therapy at discharge | |||
| Aspirin, | 1860 (82.4) | 3870 (88.0) | <0.001 |
| Missing data, (%) | 100 (4.4) | 189 (4.3) | |
| Clopidogrel, | 1087 (48.2) | 2416 (54.9) | <0.001 |
| Missing data, (%) | 99 (4.4) | 192 (4.4) | |
| Ticagrelor, | 350 (15.5) | 807 (18.4) | 0.008 |
| Missing data, (%) | 226 (10.0) | 461 (10.5) | |
| Prasugrel, | 7 (0.3) | 34 (0.8) | 0.053 |
| Missing data, | 1326 (58.8) | 2526 (57.4) | |
| BBs, | 1489 (66.0) | 3098 (70.5) | <0.001 |
| Missing data, | 276 (12.2) | 562 (12.8) | |
| ACEis, | 1025 (45.4) | 2147 (48.8) | 0.006 |
| Missing data, | 277 (12.3) | 567 (12.9) | |
| ARBs, | 254 (11.3) | 415 (9.4) | 0.049 |
| Missing data, | 382 (16.9) | 793 (18.0) | |
| CCBs, | 438 (19.4) | 706 (16.1) | 0.003 |
| Missing data, | 379 (16.8) | 782 (17.8) | |
| Statin, | 1632 (72.3) | 3321 (75.5) | <0.001 |
| Missing data, | 275 (12.2) | 562 (12.8) | |
| Procedural characteristics | |||
| Involved vessels, | <0.001 | ||
| 0 | 662 (29.3) | 565 (12.8) | |
| 1 | 636 (28.2) | 1418 (32.2) | |
| 2 | 422 (18.7) | 1044 (23.7) | |
| 3 | 326 (14.4) | 863 (19.6) | |
| LM | 123 (5.4) | 377 (8.6) | |
| Missing data, | 88 (3.9) | 130 (3.0) | |
| Time to angiography, hours [IQR] | 20 [3.9, 50.7] | 20 [3.7, 51] | 0.732 |
| Time to PCI, hours [IQR] | 12.4 [2.4, 48.1] | 14.4 [3, 49.7] | 0.137 |
| Time to CABG, days [IQR] | 10.3 [6, 15] | 8.5 [1.2, 13.1] | 0.002 |
| Treatment strategy, | <0.001 | ||
| Medical | 927 (41.1) | 973 (22.1) | |
| PCI | 1024 (45.4) | 2591 (58.9) | |
| CABG | 224 (9.9) | 703 (16.0) | |
| No angio | 82 (3.6) | 129 (2.9) | |
| Missing data | 0 (0.0) | 1(0.0) | |
| Hospital stay, days [IQR] | 4 [3, 8] | 4 [3, 9] | 0.545 |
| Early strategy ( | Delayed strategy ( | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Endpoints | Females ( | Males ( | HR |
| HR adjusted |
| Females ( | Males ( | HR |
| HR adjusted |
|
|
| Primary endpoint | 86 (7.5) | 157 (6.9) | 1.08 (0.83–1.41) | 0.560 | 0.96 (0.74–1.26) | 0.790 | 103 (9.2) | 178 (8.4) | 1.12 (0.88–1.43) | 0.350 | 0.92 (0.72–1.19) | 0.530 | 0.850 |
| All-cause death | 51 (4.5) | 86 (3.8) | 1.18 (0.83–1.66) | 0.360 | 1.05 (0.74–1.50) | 0.780 | 61 (5.5) | 86 (4.0) | 1.38 (0.99–1.91) | 0.056 | 1.10 (0.78–1.55) | 0.600 | 0.510 |
| Myocardial infarction | 46 (4) | 79 (3.5) | 1.15 (0.80–1.66) | 0.440 | 1.01 (0.70–1.46) | 0.960 | 53 (4.7) | 105 (4.9) | 0.97 (0.70–1.35) | 0.860 | 0.82 (0.58–1.15) | 0.240 | 0.490 |
| Recurrent ischaemia | 32 (2.8) | 80 (3.5) | 0.84 (0.56–1.27) | 0.420 | 0.81 (0.52–1.27) | 0.360 | 51 (4.6) | 69 (3.2) | 1.52 (1.06–2.19) | 0.023 | 1.42 (0.96–2.09) | 0.078 | 0.011 |
| Stroke | 5 (0.4) | 17 (0.8) | 0.56 (0.21–1.52) | 0.260 | 0.53 (0.19–1.44) | 0.210 | 12 (1.1) | 16 (0.8) | 1.46 (0.69–3.08) | 0.320 | 1.28 (0.58–2.82) | 0.540 | 0.150 |
| Major bleeding | 22 (1.9) | 51 (2.3) | 0.84 (0.51–1.38) | 0.480 | 0.78 (0.46–1.31) | 0.340 | 41 (3.7) | 44 (2.1) | 1.88 (1.22–2.87) | 0.004 | 1.29 (0.80–2.08) | 0.300 | 0.019 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Myocardial Infarction Research · Antiplatelet Therapy and Cardiovascular Diseases · Venous Thromboembolism Diagnosis and Management
Introduction
Ischaemic heart disease is the leading cause of mortality in females globally.^1^ Females presenting with myocardial infarction (MI) have higher risk of major adverse events compared with males.^2,3^ Females with non-ST-elevation acute coronary syndrome (NSTE-ACS) are older than males, and have a higher burden of comorbidities and complications following invasive strategy.^4–7^ Despite international guidelines recommending equality in the management of ACS regardless of sex,^8^ females are under-represented in studies investigating different interventional strategies and are less likely to receive evidence-based therapies.^4,8–11^
The use of routine invasive coronary angiography for high-risk NSTE-ACS, in comparison to a selective or ‘ischaemia-guided’ strategy, is associated with reductions in ischaemic outcomes.^12–14^ Current guidelines recommend (Class IIa) an early invasive strategy (within 24 h) in the presence of any high-risk criteria, such as diagnosis of non-ST-elevation myocardial infarction (NSTEMI) based on high-sensitivity cardiac troponin, dynamic ST-segment/T waves changes, transient ST-elevation, and Global Registry of Acute Coronary Events (GRACE) risk score >140.^8^ Over the past decade, several studies have reinforced the recommendation that complete coronary revascularization should be the preferred approach over culprit-only revascularization in ACS patients with multivessel disease. This strategy, irrespective of the timing of intervention, is aimed at reducing the risk of cardiovascular mortality, recurrent MI, and ischaemia-driven revascularization.^15,16^ We recently showed that an early invasive management in females with NSTE-ACS, compared with a delayed invasive management, was not associated with a significant reduction in the hazard for all-cause mortality or MI.^17^ In pre-specified subgroup analysis, high-risk females as assessed with GRACE score >140 or elevated cardiac biomarkers experienced significant reductions in all-cause mortality or MI at 6 months following early invasive management.^17^ However, the sex-related differences in adverse clinical outcomes between females and males with NSTE-ACS undergoing early or delayed invasive management is not known.^18–23^ This individual patient data (IPD) meta-analysis aims to investigate the sex-related differences in adverse clinical outcomes among patients undergoing early or delayed invasive strategy for the management of their NSTE-ACS.
Methods
Search strategy and selection criteria
The present study consists of a post-hoc analysis using IPD of randomized controlled trials (RCTs) enrolling NSTE-ACS patients randomly allocated to early or delayed invasive management, with a specific focus on sex-related differences. The inclusion criteria were: (1) patients with a diagnosis of unstable angina or NSTEMI (according to international guidelines in place at the time of each trial) hospitalized within 24 h after ischaemic symptoms. Diagnostic criteria included (i) electrocardiographic changes compatible with ischaemia [new ST-segment depression >1 millivolt (mV), transient ST-segment elevation or T waves inversion] and/or (ii) elevated biomarkers [troponin T > 0.05 ng/mL, troponin I greater than the upper limit of normal, myoglobin >150 µg/L, creatine kinase muscle brain (CK-MB) fraction >6% of total CK]; (2) comparison between early vs. delayed invasive strategy; (iii) random allocation; (iv) at least 30-day follow-up; and (v) minimum of 200 participants and/or 50 females. Randomized controlled trials were selected by searching MEDLINE, Web of Science and Scopus without language and date restriction. Detailed search algorithm is provided in the Supplementary material online, Supplementary methods.
Studies were screened for eligibility by two independent reviewers (GBM and VK). After systematic evaluation of the inclusion and exclusion criteria, the principal investigators of all eligible studies were invited to share published and/or unpublished IPD. Variables of interest were selected at the study protocol stage according to clinical relevance and consistency across trials. Data accuracy was assessed for completeness and integrity before being merged into a single database. This IPD meta-analysis was conducted according to the Preferred Reporting Items of Systematic Reviews and Meta-analyses (PRISMA) statement (see Supplementary material online, Table S1). The protocol was registered on the International Prospective Register of Systematic Reviews (PROSPERO, CRD42023468604).
Comparison groups and outcomes
Early and delayed invasive strategies were defined according to the original definitions of each randomized controlled trial (RCT) and based on the time interval between randomization and coronary angiography. In case of studies randomizing patients to three different arms, patients allocated to the immediate invasive strategy arm were combined with those undergoing an early invasive strategy.
All patients were prescribed optimal medical therapy regardless of the revascularization strategy. A median follow-up was used according to the follow-up length reported in each RCT. The primary endpoint was a composite of all-cause death or MI. The secondary endpoints included individual clinical outcomes such as all-cause death, MI, stroke, recurrent ischaemia, and major bleeding events. Clinical endpoints were as defined originally by the included trials (Table 1). Overall, across the RCTs recurrent ischaemia was defined as recurrent chest pain despite optimal medical therapy associated with or without electrocardiogram (ECG) changes and requiring repeat hospitalization or additional intervention. The definition is heterogeneous across the studies, but it did not coincide with those used to define MI.
Each definition of MI took into account different biomarker cut-offs based on the time of onset of symptoms from randomization, associated or not with pathological Q-waves or ECG changes. Troponin T or I may have been used for the diagnosis if CK-MB was not available. A definition for periprocedural MI is provided, discerning patients with already elevated enzymes from those without (Table 1).
Statistical analysis
For all main analyses, only variables with missingness <10% were considered. For categorical variables, an extra level to depict a missing value was created. Categorical variables were reported as counts and percentages and compared by either χ^2^ or Fisher's exact test. The distribution of continuous variables was evaluated through the Shapiro–Wilk test and reported as mean and standard deviation or median and interquartile range (IQR) for normal and non-normal distribution, respectively, and compared using either Student's t-test or Mann–Whitney U-test, as appropriate.
Time-to-first event was used to assess outcomes, and the analyses followed the intention-to-treat principle. Kaplan–Meier analysis was used to outline cumulative adverse events along with numbers at risk. To obtain the risk of each endpoint, one-stage, random-effects Cox proportional hazards regression models with shared frailty were conducted for comparisons, with treatment strategy assignment as the fixed component and the original RCT as the random component. Risk estimates were reported as hazard ratios (HR) and 95% confidence intervals (CI) with respective P-values and P for interaction between sex and treatment strategy. All tests were two-sided, with P < 0.05 considered significant. The analyses were performed in early and delayed cohorts with sex as predictor variable. As pre-specified, multivariable adjustment was based on the random effects Cox model taking into account age, diabetes mellitus, biomarkers status, and GRACE score. Further fixed-effect Cox proportional hazards models were computed as sensitivity analysis. As an exploratory analysis, the overall population was stratified by GRACE score. Low-risk and high-risk were defined by GRACE score ≤140 or >140, respectively. The analyses using random-effects Cox proportional hazards regression models were then performed within early and delayed cohorts, using sex as predictor variable.
The Cochrane Risk-of-Bias 2 (RoB 2) tool was used to evaluate potential sources of bias. Statistical between-trial heterogeneity was assessed through tau^2^ (τ^2^) and I^2^ tests. In case of high between-trial heterogeneity, additional analyses were performed to explore which of the included studies were sources of heterogeneity. Publication bias was assessed by Egger's regression test and visual assessment of funnel plots, using Trim-and-Fill method to correct the results for those endpoints suspected of publication bias. The analyses were conducted using R version 4.3.1 and R Studio version 1.4.1106 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Out of the 2232 results identified from literature source, 1292 titles and abstracts were screened. After exclusion of 1274 studies, 18 were evaluated for eligibility. Supplementary material online, Table S2 provides a list of further 12 excluded studies. Six RCTs were included and provided IPD (see Supplementary material online, Tables S3–S8). The Leipzig Immediate vs. early and late PercutaneouS coronary Intervention triAl in NSTEMI (LIPSIA-NSTEMI) randomly assigned patients to three arms: immediate, early, and selectively invasive. Patients allocated to the latter were not included. A total of 6654 patients with complete follow-up data were analysed (see Supplementary material online, Figure S1). Three out of the six trials used a strategy of immediate invasive procedure for the early group (LIPSIA-NSTEMI, RIDDLE-NSTEMI, and ELISA-3), whereas for the other studies the median time to angiography in the early cohort consisted of a larger interval, up to 24 h after randomization. There was overlap between the IQR of the time to angiography in both the arms of LIPSIA-NSTEMI study and the early strategy of the other trials (see Supplementary material online, Figure S2). The median follow-up was 185 days (6 months).
Heterogeneity test and publication bias
The between-trial heterogeneity was low for the primary endpoint (τ^2^ < 0.001, I^2^ 10%), death (τ^2^ 0.000, I^2^ 0%), stroke (τ^2^ < 0.000, I^2^ 0%), and major bleeding (τ^2^ < 0.004, I^2^ 0%). Conversely, MI and recurrent ischaemia were associated with high between-trial heterogeneity (MI: τ^2^ 0.356, I^2^ 62.9%; recurrent ischaemia: τ^2^ 0.139, I^2^ 56.8%). Therefore, for the endpoints MI and recurrent ischaemia, a two-stage meta-analysis was conducted, excluding the RCTs identified as the most influential and responsible for between-trial heterogeneity. The results indicated that the pooled effect remained non-significant, confirming consistency with the previous findings (see Supplementary material online, Figures S5–S10).
No significant sign of publication bias was detected for the primary endpoint (P-value = 0.726), death (P-value = 0.799), MI (P-value = 0.904), and recurrent ischaemia (P-value = 0.736). While Egger's test showed publication bias for stroke (P-value < 0.001) and major bleeding (P-value = 0.047), Trim-and-Fill correction did not identify any significant difference (stroke P-value = 0.549, major bleeding P-value = 0.379). Supplementary material online, Figure S11 displays the funnel plots for visual estimation of the publication bias result reported for each endpoint.
Risk of bias
All trials had a low risk of bias. Considering the non-blinded allocation to different timing does not represent a high-risk feature, the authors judged the effect of assignment to intervention section to be low risk. However, it should be taken into account that blinding the treatment strategy was not possible since patients and medical staff were aware of the timing (see Supplementary material online, Figure S12).
Baseline characteristics
Out of the total 6654 patients, 2257 (33.9%) were female with a median age of 69 years (IQR 60–76), significantly higher than male patients (64.5 years, IQR 55–72, P < 0.001). There were significant differences in baseline characteristics between females and males as shown in Table 2. Fewer females were former or current smokers (21.7 vs. 34.2%, P < 0.001) and had a past medical history positive for previous MI (14.5 vs. 20.5%, P < 0.001), coronary artery bypass grafting (CABG) (4.4. vs. 8.4%, P < 0.001), and percutaneous coronary intervention (PCI) (11.3 vs. 16.9%, P < 0.001) compared with males. In contrast, more females had hypertension (68 vs. 59.3%, P < 0.001) and diabetes mellitus (27.2 vs. 21.2%, P < 0.001) than males. Higher GRACE scores were identified in females compared with males [136 (IQR 117–157) vs. 131 (IQR 113–151), P < 0.001]. Non-obstructive coronaries were reported more frequently in females (29.3 vs. 12.8%, P < 0.001). Compared with females, males had a higher incidence of three-vessel disease (19.6 vs. 14.4%, P < 0.001) and left main involvement (8.6 vs. 5.4%, P < 0.001). Significant differences in secondary prevention medications at discharge were found, with females more frequently receiving calcium channel blockers (19.4 vs. 16.1%, P = 0.003) and angiotensin-receptor blockers (11.3 vs. 9.4%, P = 0.049), whereas males were more often prescribed beta-blockers (70.5 vs. 66%, P < 0.001), angiotensin-converting enzyme inhibitors (48.8 vs. 45.4%, P = 0.006), and statins (75.5 vs. 72.3%, P < 0.001) (Table 2).
Sex differences in outcomes in the early strategy
Among patients allocated to the early invasive strategy, no difference in the risk and incidence of the primary endpoint (females: 7.5% vs. males: 6.9%, HR 1.08, 95% CI 0.83–1.41, P = 0.560) was found using random-effects Cox regression models at both univariable and multivariable analysis (Figure 1 and Table 3). There was also no difference in the individual risk of all-cause death, MI, recurrent ischaemia, stroke, and major bleeding (Table 3, Supplementary material online, Figure S3, Figure 2). Similar findings were obtained using fixed-effect model (see Supplementary material online, Table S9).
Primary endpoint events in patients undergoing early and delayed invasive strategy stratified by sex. Abbreviations: pLR = P-log rank.
Multivariable Cox regression analysis using random effect in the early and delayed invasive strategy groups stratified by sex. Forest plots show multivariable Cox regression analysis using random effect, adjusted for age, diabetes mellitus, biomarkers status, and Global Registry of Acute Coronary Events score. Abbreviations: PE, primary endpoint; MI, myocardial infarction; RI, recurrent ischaemia; HRadj, hazard ratio adjusted; CI, confidence interval; GRACE, Global Registry of Acute Coronary Events.
Sex differences in outcomes in the delayed strategy
Among patients allocated to the delayed invasive strategy, no difference in the risk and incidence of the primary endpoint (females: 9.2% vs. males: 8.4%, HR 1.12, 95% CI 0.88–1.43, P = 0.350) was found (Table 3 and Figure 1). There was also no difference in the risk of all-cause death, MI and stroke (see Supplementary material online, Figure S4).
Female sex vs. male sex was associated with increased risk and incidence of recurrent ischaemia (4.6 vs. 3.2%, HR 1.52, 95% CI 1.06–2.19, P = 0.023) and major bleeding (3.7 vs. 2.1%, HR 1.88, 95% CI 1.22–2.87, P = 0.004) using univariable analysis (Table 3 and Figure 3). Multivariable analysis did not confirm these differences as statistically significant (Table 3 and Figure 2). Tests for interaction between sex and treatment strategy were statistically significant for recurrent ischaemia and major bleeding (P-value for interaction 0.011 and 0.019, respectively) (Table 3). Similar findings were obtained using fixed-effect model (see Supplementary material online, Table S9).
Recurrent ischaemia and major bleeding events in patients undergoing delayed invasive strategy stratified by sex. Abbreviations: pLR = p-log rank.
Sex differences within early and delayed strategy groups stratified by Global Registry of Acute Coronary Events score
Risk stratification using GRACE score was available in 95.8% (n = 6372) of patients. No significant difference in the primary and secondary endpoints between females and males was reported in patients undergoing early invasive strategy, regardless of the level of risk.
Among low-risk patients allocated to delayed invasive strategy, female sex vs. male sex was associated with increased incidence and the risk of major bleeding (3.2 vs. 1.4%, HR 2.34, 95% CI 1.23–4.46, P = 0.010) (see Supplementary material online, Table S10). Among high-risk patients allocated to delayed strategy, female sex vs. male sex was associated with an increased incidence and risk of recurrent ischaemia (5.8 vs. 3.9%, HR 1.69, 95% CI 1.01–2.83, P = 0.048) (see Supplementary material online, Table S11). These findings were confirmed by the analyses performed using fixed-effect model (see Supplementary material online, Tables S12 and S13).
Discussion
Among patients undergoing early or delayed invasive strategy for the management of NSTE-ACS, there were no differences in the risk of primary endpoint between females and males. Among patients undergoing delayed invasive strategy, female sex was associated with increased risk of recurrent ischaemia and major bleeding using univariable analysis but not using multivariable analysis.
This IPD meta-analysis confirms that female NSTE-ACS patients present with different cardiovascular risk factors, past medical history, and are treated with different secondary prevention medications at discharge compared with male patients as well as a different revascularization strategy, a finding consistent with prior studies.^24–28^ In both early and delayed groups, females had a slightly higher composite risk of all-cause mortality and MI compared with males, although this difference did not reach statistical significance.
The variation in the timing of early intervention across the included RCTs obscures the true impact of treatment on new MI occurrence. Furthermore, the significant difference in the rate of revascularization (PCI or CABG) females and males underwent (55.3 vs. 74.9%, respectively), as well as the differences in multivessel disease, may have impacted on this result. A meta-regression revealed that a wider time interval between early and delayed treatment is associated with lower risk of new MI in patients allocated to early invasive strategy. This association was shown to be stronger in studies with higher PCI rates, indicating a positive effect of early treatment in a population suffering from a more severe coronary artery disease (CAD).^29^
In the current analysis, the difference in the median time to PCI between early and delayed groups in both sexes corresponded to 45.4 h, equivalent to approximately half of the ISAR-COOL trial, excluded from the present meta-analysis due to the long time period in the delayed group.^30^ We reported three-vessel disease and left main involvement more frequently in men compared with women and, as a consequence, a significantly higher percentage of men underwent revascularization compared with women, resulting in stabilization of such a great number of severe CAD including unstable/significant plaques in male patients.
The univariable Cox regression analysis confirmed the association between female sex and the risk of recurrent ischaemia and major bleeding among patients receiving delayed strategy. In NSTE-ACS, ruling out epicardial CAD is the first step towards establishing a diagnosis of myocardial infarction with non-obstructive coronary arteries (MINOCA) occurring more frequently in females.^31^ In our study, females had more non-obstructive CAD (29.3 vs. 12.8%, P < 0.001) than males. This spectrum encompasses a heterogeneous group of underlying causes, including both extracardiac and cardiac origins, with the latter arising from coronary or non-coronary mechanisms. Therefore, a prompt pathophysiological characterization in the female population with an early invasive strategy, aims to control symptoms and prevent recurrent ischaemia, but also to tailor pharmacological therapy to address specific pathophysiological mechanisms (such as vasospastic angina and coronary microvascular dysfunction) and decrease bleeding risk.
Female sex is often associated with criteria defining high bleeding risk, such as older age, kidney disease, and anaemia.^32,33^ In our study, among patients undergoing delayed strategy females experience bleeding complications more frequently than males. The multivariable analysis did not confirm the association between female sex and the risk of recurrent ischaemia and major bleedings in patients receiving delayed invasive strategy. This finding suggests the potential influence of confounding variables not fully accounted for in the present analysis. The time interval between the onset of symptoms and presentation in hospital has been demonstrated to be longer in females compared with males.^34^ Females experience delays secondary to lack of awareness, socio-economic barriers, and underestimated risk. These factors, in addition to the older age and higher GRACE score, should be taken into account and added to the prolonged time in the delayed invasive strategy arm, leading to recurrent symptoms during the follow-up. Moreover, it is also important to take into consideration the role of concomitant conditions rather than an independent biological association between female sex and haemorrhagic risk.^35^
We showed that in patients with a higher baseline ischaemic risk profile (defined by GRACE score >140) in whom invasive management was delayed, female sex was associated with higher risk of recurrent ischaemia (see Supplementary material online, Tables S10 and S11). On the other hand, in low-risk patients (GRACE score ≤140) and a delayed procedure, females were more prone to develop major bleeding. These findings underscore a potentially differential role of baseline risk stratification for male and female NSTE-ACS patients, with a need to define coronary anatomy early in females to tailor treatment and initiate further diagnostic tests if needed, particularly given the fact that nearly one-third of females have non-obstructive CAD.
Regardless of risk stratification, the increased risk of recurrent ischaemia in females compared with males undergoing delayed strategy does not correlate with subsequent higher rate of MI events. This is supported by a large meta-analysis which reported a significant reduction in the risk of recurrent ischaemia among NSTE-ACS patients using an early strategy compared with a delayed strategy.^36^ Taken altogether, it seems fair to speculate that the higher proportion of females with non-obstructive disease may reflect that recurrent ischaemia could be caused by other pathophysiological entities (such as coronary microvascular dysfunction).
Strengths and limitations
This post-hoc analysis provides important findings given the availability of patient-level data, which allowed for more complex statistical approaches and greater statistical power to investigate interactions between treatment strategies and covariates. However, this study has several limitations. Heterogeneity across the studies with respect to inclusion criteria, timing of invasive strategy, endpoint definitions, and follow-up might have had an impact on the results. The definitions of recurrent ischaemia differed between trials, and data on major bleeding were available in only four studies. There was lack of universal definition of non-fatal MI across the trials. Risk stratification was performed using GRACE score, since data on high-sensitivity c Troponin and ST-elevation were missing in five studies. Previous studies have demonstrated sex-specific limitations of the GRACE 2.0 score, exemplified by a systematic underestimation of in-hospital mortality risk in females.^5^ Data on dynamic ST-segment/T waves changes was not available. Variables regarding procedural characteristics (access site, anticoagulation dose, and procedural time) and comorbidities to better investigate sex-based differences are lacking, as are data on time interval between symptom onset and presentation. Furthermore, relevant clinical covariates, such as kidney failure and antithrombotic therapy, were not considered in the multivariable analysis, which was limited to variables pre-specified in PROSPERO. The findings should be interpreted with caution due to the limitations of post-hoc analyses, which may not fully exclude bias or confounding factors related to sex-based comparisons. Two out of the six endpoints, MI and recurrent ischaemia, were associated with high between-trial heterogeneity, while stroke and major bleeding may have been influenced by publication bias. However, Trim-and-Fill correction provided consistent outcomes. Lastly, the median follow-up was 185 days, and further long-term evidence is needed.
Conclusion
In this IPD meta-analysis, no sex-related differences in the composite of all-cause death or MI were identified among NSTE-ACS patients undergoing early and delayed invasive management. Among patients treated with a delayed invasive strategy, female sex was associated with increased risk of recurrent ischaemia and major bleeding using univariable analysis but not using multivariable analysis (Graphical abstract). The present post-hoc analysis should encourage physicians to take into account and expect different adverse clinical outcomes between sexes in cases where a delayed invasive strategy is adopted. There is a need to focus on subsets of patients who are typically under-represented and under-investigated in most RCTs, such as women with cardiovascular disease, highlighting the impact of female biology on specific treatments to overcome delays in management. Further large-scale research using contemporary treatment strategies is needed to investigate sex-related differences in long-term clinical outcomes and to inform optimal care among females.
Supplementary Material
oeaf059_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Vogel B, Acevedo M, Appelman Y, Bairey Merz CN, Chieffo A, Figtree GA, Guerrero M, Kunadian V, Lam CSP, Maas AHEM, Mihailidou AS, Olszanecka A, Poole JE, Saldarriaga C, Saw J, Zühlke L, Mehran R. The Lancet women and cardiovascular disease Commission: reducing the global burden by 2030. Lancet 2021;397:2385–2438.34010613 10.1016/S 0140-6736(21)00684-X · doi ↗ · pubmed ↗
- 2Lawless M, Appelman Y, Beltrame JF, Navarese EP, Ratcovich H, Wilkinson C, Kunadian V. Sex differences in treatment and outcomes amongst myocardial infarction patients presenting with and without obstructive coronary arteries: a prospective multicentre study. Eur Heart J Open 2023;3:oead 033.10.1093/ehjopen/oead 033PMC 1011452837090058 · doi ↗ · pubmed ↗
- 3Canton L, Fedele D, Bergamaschi L, Foa A, Di Iuorio O, Tattilo FP, Rinaldi A, Angeli F, Armillotta M, Sansonetti A, Stefanizzi A, Amicone S, Impellizzeri A, Suma N, Bodega F, Cavallo D, Bertolini D, Ryabenko K, Casuso M, Belmonte M, Gallinoro E, Casella G, Galiè N, Paolisso P, Pizzi C. Sex- and age-related differences in outcomes of patients with acute myocardial infarction: MINOCA vs. MIOCA. Eur Heart J Acute Cardiovasc Care 2023;12:604–614.37261384 10.1093/ehjacc/zuad · doi ↗ · pubmed ↗
- 4Sarma AA, Braunwald E, Cannon CP, Guo J, Im K, Antman EM, Gibson CM, Newby LK, Giugliano RP, Morrow DA, Wiviott SD, Sabatine MS, O’Donoghue ML. Outcomes of women compared with men after non-ST-segment elevation acute coronary syndromes. J Am Coll Cardiol 2019;74:3013–3022.31865968 10.1016/j.jacc.2019.09.065 · doi ↗ · pubmed ↗
- 5Wenzl FA, Kraler S, Ambler G, Weston C, Herzog SA, Raber L, Muller O, Camici GG, Roffi M, Rickli H, Fox KAA, de Belder M, Radovanovic D, Deanfield J, Lüscher TF. Sex-specific evaluation and redevelopment of the GRACE score in non-ST-segment elevation acute coronary syndromes in populations from the UK and Switzerland: a multinational analysis with external cohort validation. Lancet 2022;400:744–756.36049493 10.1016/S 0140-6736(22)01483-0 · doi ↗ · pubmed ↗
- 6Nadarajah R, Ludman P, Laroche C, Appelman Y, Brugaletta S, Budaj A, Bueno H, Huber K, Kunadian V, Leonardi S, Lettino M, Milasinovic D, Gale CP. Sex-specific presentation, care, and clinical events in individuals admitted with NSTEMI: the ACVC-EAPCI EORP NSTEMI registry of the European Society of Cardiology. Eur Heart J Acute Cardiovasc Care 2024;13:36–45.37926912 10.1093/ehjacc/zuad 134 · doi ↗ · pubmed ↗
- 7Jackson J, Alkhalil M, Ratcovich H, Wilkinson C, Mehran R, Kunadian V. Evidence base for the management of women with non-ST elevation acute coronary syndrome. Heart 2022;108:1682–1689.35064048 10.1136/heartjnl-2021-320533 · doi ↗ · pubmed ↗
- 8Byrne RA, Rossello X, Coughlan JJ, Barbato E, Berry C, Chieffo A, Claeys MJ, Dan G-A, Dweck MR, Galbraith M, Gilard M, Hinterbuchner L, Jankowska EA, Jüni P, Kimura T, Kunadian V, Leosdottir M, Lorusso R, Pedretti RFE, Rigopoulos AG, Rubini Gimenez M, Thiele H, Vranckx P, Wassmann S, Wenger NK, Ibanez B, Halvorsen S, James S, Abdelhamid M, Aboyans V, Marsan NA, Antoniou S, Asteggiano R, Bäck M, Capodanno D, Casado-Arroyo R, Cassese S, Čelutkienė J, Cikes M, · doi ↗ · pubmed ↗