Methicillin-Resistant Staphylococcus aureus (MRSA) Strikes Deep: Infected Femoral Aneurysm in a Patient With Deep Vein Thrombosis
George K Annan, Patrick O Berchie, Alex Kumi, Moises Zouain Estevez, Chinenye Egwuonwu

TL;DR
A patient with MRSA infection developed a life-threatening aneurysm in the leg due to deep vein thrombosis, highlighting the need for early imaging and aggressive treatment.
Contribution
This case report highlights MRSA as a cause of mycotic aneurysms in the context of deep vein thrombosis and emphasizes the importance of early diagnosis.
Findings
MRSA bacteremia led to an infected femoral aneurysm in a patient with deep vein thrombosis.
Persistent symptoms despite antibiotic treatment necessitated urgent surgical intervention.
Early imaging and multidisciplinary care are critical to prevent rupture and limb loss.
Abstract
Infectious (mycotic) aneurysms are rare but potentially life-threatening complications of bacteremia. They account for a small percentage of all aneurysms. Early recognition is essential to prevent catastrophic outcomes. We report a case of a 53-year-old man with a history of methicillin-resistant Staphylococcus aureus (MRSA) nasal abscess who presented with fever, vomiting, and progressive right leg swelling. He was febrile and tachycardic. Labs showed neutrophilic leukocytosis (white cell count of 17.4 x 10⁹/L), elevated C-reactive protein (CRP; 127.4 mg/L), and positive blood cultures for MRSA. Doppler ultrasound revealed acute deep vein thrombosis (DVT) in the right femoral and deep veins. Despite vancomycin, he had persistent bacteremia, and antibiotics were escalated to ceftaroline and daptomycin. Computed tomography (CT) angiography obtained for worsening leg swelling revealed a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
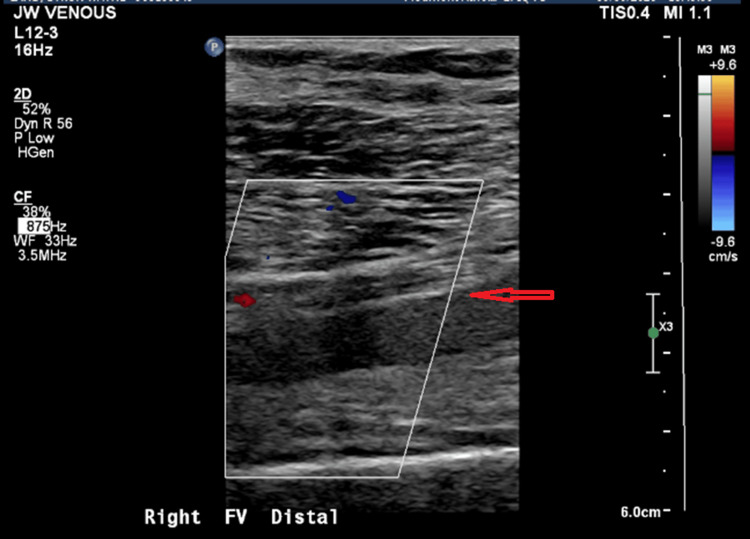 Figure 1
Figure 1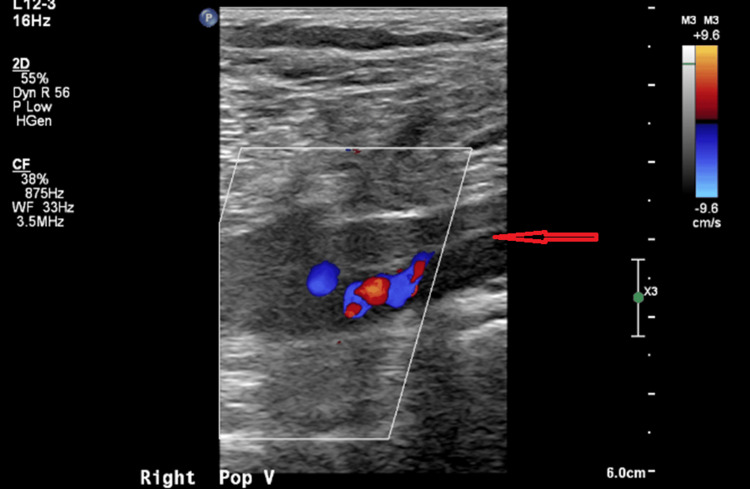 Figure 2
Figure 2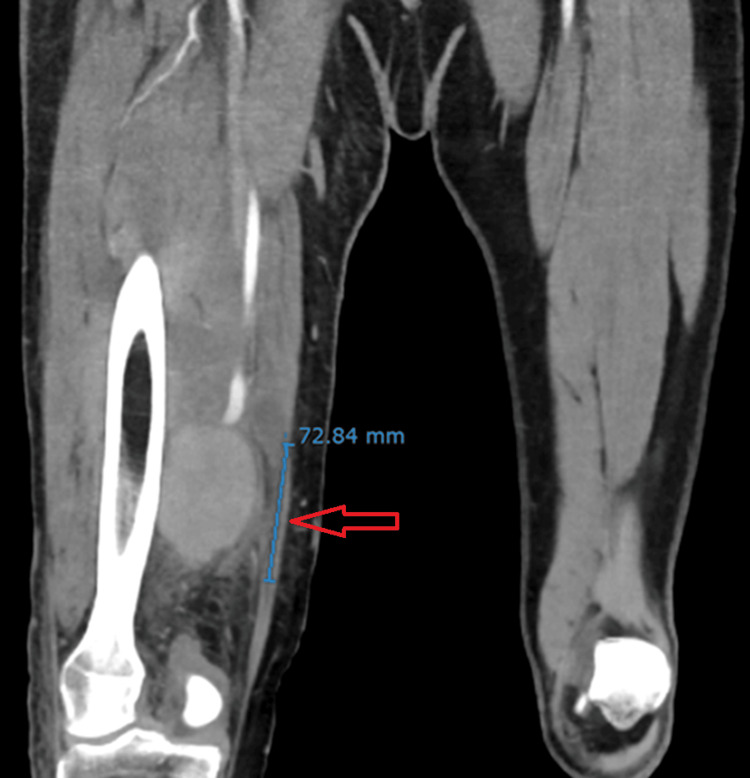 Figure 3
Figure 3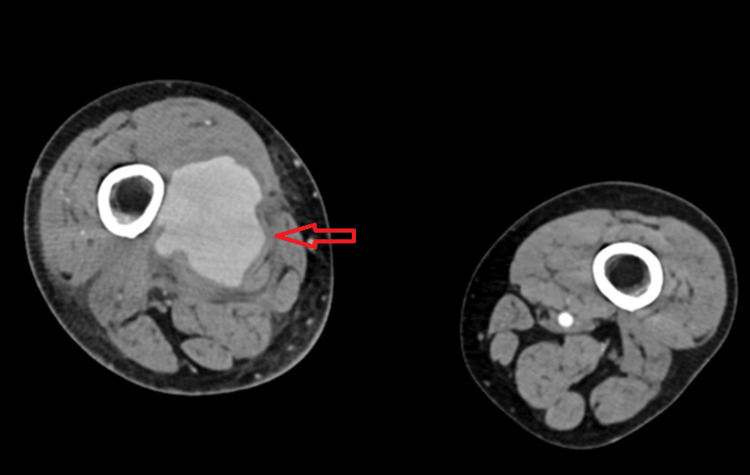 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Aortic and Vascular Conditions · Vascular Procedures and Complications · Infective Endocarditis Diagnosis and Management
Introduction
Infectious (mycotic) aneurysms are rare but potentially life-threatening complications of bacteremia. Bacteremia can lead to arterial wall infection through hematogenous spread, resulting in inflammation and weakening of the vessel wall, which predisposes to aneurysm formation. According to the American Heart Association, mycotic aneurysms are rare overall, and the true incidence is not defined in the general population. The femoral artery is the most involved site among peripheral mycotic aneurysms [1].
When accompanied by deep vein thrombosis (DVT), these cases pose significant diagnostic and therapeutic challenges. If left untreated, an infected aneurysm can rupture, which can lead to a life-threatening hemorrhage [1]. This case highlights the importance of recognizing atypical vascular complications of methicillin-resistant Staphylococcus aureus (MRSA) bacteremia and the need for timely interdisciplinary management.
Case presentation
A 53-year-old man with a history of hypertension, hyperlipidemia, and MRSA nasal abscess presented with a five-day history of right lower extremity pain and swelling, as well as four days of persistent vomiting and high-grade fevers up to 101.7°F. There was no history of trauma, cancer, or known hypercoagulable disorder. He endorsed frequent long-distance travel by road.
He was febrile, with a temperature of 100.4°F, tachycardic, and tachypneic. Physical examination was significant for a warm, swollen, and tender right lower extremity. Laboratory workup revealed neutrophilic leukocytosis with a white cell count of 17.40 ×10⁹/L and elevated C-reactive protein (CRP) of 127.4 mg/L. Blood cultures grew MRSA. Venous Doppler (Figures 1, 2) showed acute DVT involving the distal femoral and distal deep venous system of the right lower extremity. The transthoracic echocardiogram was unremarkable.
Ultrasound image of right distal femoral vein thrombosisCompression ultrasound of the right thigh showing a non-compressible, dilated right distal femoral vein (arrow) with an acute thrombus, consistent with acute deep vein thrombosis.
Ultrasound image of right popliteal vein thrombosisCompression ultrasound of the right popliteal fossa showing a non-compressible, dilated right popliteal vein (arrow), consistent with acute deep vein thrombosis.
He was initially started on vancomycin and intravenous heparin. However, due to persistent bacteremia and concerns about impaired bacterial clearance from the clot, vancomycin was discontinued, and salvage therapy with ceftaroline and daptomycin was initiated. Despite therapeutic anticoagulation and appropriate antibiotics, the patient had persistent bacteremia and worsening swelling in the right lower extremity. A computed tomography (CT) angiogram was obtained, which showed a large right superficial femoral artery aneurysm measuring 6.4 x 6.3 x 7.3 cm (Figures 3, 4). He underwent urgent surgical excision, ligation, and bypass with subsequent serial washout procedures. The swelling in the right extremity markedly improved with defervescence and resolution of bacteremia. CRP and white cell count normalized. He had a peripherally inserted central catheter (PICC line) placed and was discharged home to continue a total of six weeks of intravenous daptomycin with weekly creatinine kinase monitoring. He was also transitioned to Eliquis. At his two-week follow-up visit, he had no swelling of the right lower extremity or fevers.
Coronal CT angiogram of right superficial femoral artery aneurysmContrast-enhanced coronal CT angiography demonstrates a large, saccular aneurysm (red arrow) arising from the right superficial femoral artery, measuring approximately 6.4 × 6.3 × 7.3 cm in cross-section. There is subcutaneous soft tissue stranding in the posterior right thigh and popliteal fossa.
Axial CT angiogram of right superficial femoral artery aneurysmContrast-enhanced axial CT angiography demonstrates a large, saccular aneurysm (red arrow) arising from the right superficial femoral artery, measuring approximately 6.4 × 6.3 × 7.3 cm in cross-section.
Discussion
This case highlights an unusual and severe complication of MRSA bacteremia, an infectious femoral artery aneurysm, occurring in conjunction with extensive lower extremity DVT. Infectious aneurysms are rare, representing <5% of all arterial aneurysms, and typically arise from trauma, intravenous drug use (IVDU), arterial catheterization, or contiguous spread from soft tissue infection [1,2]. The triad of DVT, bacteremia, and infectious arterial aneurysm has been reported but mostly in the context of IVDU, where local tissue necrosis, direct vascular injury, and bacteremia create a favorable environment for both venous thrombosis and arterial infection [1].
In contrast to these more recognized etiologies, our patient had no history of invasive vascular procedures or IVDU, making hematogenous seeding of the arterial wall the most likely mechanism, potentially facilitated by adjacent inflammatory compromise from the infected thrombus. The most implicated pathogens are Staphylococcus aureus (including MRSA) and, less commonly, Gram-negative bacilli such as *Salmonella *species [1,3,4]. Peripheral mycotic aneurysms, including those of the femoral artery as seen in our patient, are less common than aortic mycotic aneurysms. Precise prevalence data are limited due to their rarity and underdiagnosis [1,5].
Ceftaroline plus daptomycin as salvage therapy in MRSA bacteremia is supported by clinical and preclinical evidence, particularly in cases of persistent or refractory bacteremia after failure of standard therapy with vancomycin or daptomycin monotherapy, with trends towards early bacterial clearance [6-8].
The patient’s evolving symptoms and persistent fever despite therapeutic anticoagulation and antibiotics prompted advanced vascular imaging, leading to timely diagnosis and intervention, averting limb loss and life-threatening hemorrhage. This case illustrates that achieving source control in infected aneurysms may require multiple surgical interventions and that aggressive operative management is an essential complement to targeted antibiotic therapy. This case also highlights the critical role of multidisciplinary collaboration, involving internal medicine, infectious disease, and vascular surgery teams, in achieving favorable outcomes through timely surgical debridement with appropriate antimicrobial coverage.
Conclusions
In a patient diagnosed with bacteremia and DVT on therapeutic anticoagulation and antibiotics, progressive limb swelling and persistent bacteremia should prompt the clinician to consider infectious aneurysm in the differential diagnosis. Early vascular imaging, prompt surgical intervention, and coordinated multidisciplinary care are critical to preventing catastrophic outcomes such as hemorrhage or limb loss.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Vascular graft infections, mycotic aneurysms, and endovascular infections: a scientific statement from the American Heart Association Circulation Wilson WR Bower TC Creager MA 060134201610.1161/CIR.000000000000045727737955 · doi ↗ · pubmed ↗
- 2Spontaneous rupture of aortic aneurysm due to Listeria monocytogenes in an immunocompetent patient and review of the literature Diagn Microbiol Infect Dis Robert M Leterrier-Plong M Bouard L 11667311120253977838410.1016/j.diagmicrobio.2024.116673 · doi ↗ · pubmed ↗
- 3Infected aneurysms of neck and limb arteries: a retrospective multicenter study Ann Vasc Surg Patra P Ricco JB Costargent A Goueffic Y Pillet JC Chaillou P 1972051520011126508410.1007/s 100160010047 · doi ↗ · pubmed ↗
- 4Mycotic pseudoaneurysm of the femoral artery in a patient with psoriasis Intern Med Tashtoush B Gonzalez-Ibarra F Abed M 283128345120122303748510.2169/internalmedicine.51.8195 · doi ↗ · pubmed ↗
- 5Infected (mycotic) aneurysms: spectrum of imaging appearances and management Radiographics Lee WK Mossop PJ Little AF Fitt GJ Vrazas JI Hoang JK Hennessy OF 185318682820081900164410.1148/rg.287085054 · doi ↗ · pubmed ↗
- 6Outcomes of daptomycin plus ceftaroline versus alternative therapy for persistent methicillin-resistant Staphylococcus aureus (MRSA) bacteraemia Int J Antimicrob Agents Patel D Brown ML Edwards S Oster RA Stripling J 1067356120233669012410.1016/j.ijantimicag.2023.106735 PMC 10023467 · doi ↗ · pubmed ↗
- 7Dosing considerations for combination antistaphylococcal β-lactam and glyco/lipopeptide salvage therapy for resistant gram-positive infections: a systematic review Ann Pharmacother Reinert JP Brown M Ofori R 1932045620223408821410.1177/10600280211021421 · doi ↗ · pubmed ↗
- 8Antimicrobial salvage therapy for persistent staphylococcal bacteremia using daptomycin plus ceftaroline Clin Ther Sakoulas G Moise PA Casapao AM 131713333620142501718310.1016/j.clinthera.2014.05.061 · doi ↗ · pubmed ↗