Successful retrieval of migrated stent via endoscopic ultrasound-guided hepaticogastrostomy with fine-gauge dilation catheter
Kohei Okamoto, Susumu Hijioka, Yoshikuni Nagashio, Shota Harai, Mark Chatto, Yutaka Saito, Takuji Okusaka

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
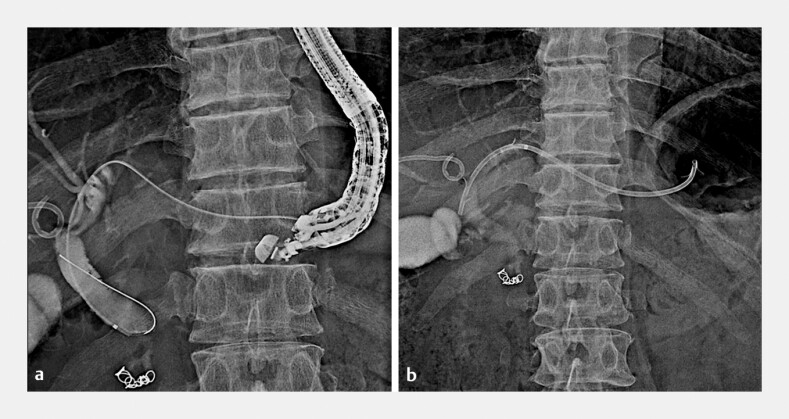 Fig. 1
Fig. 1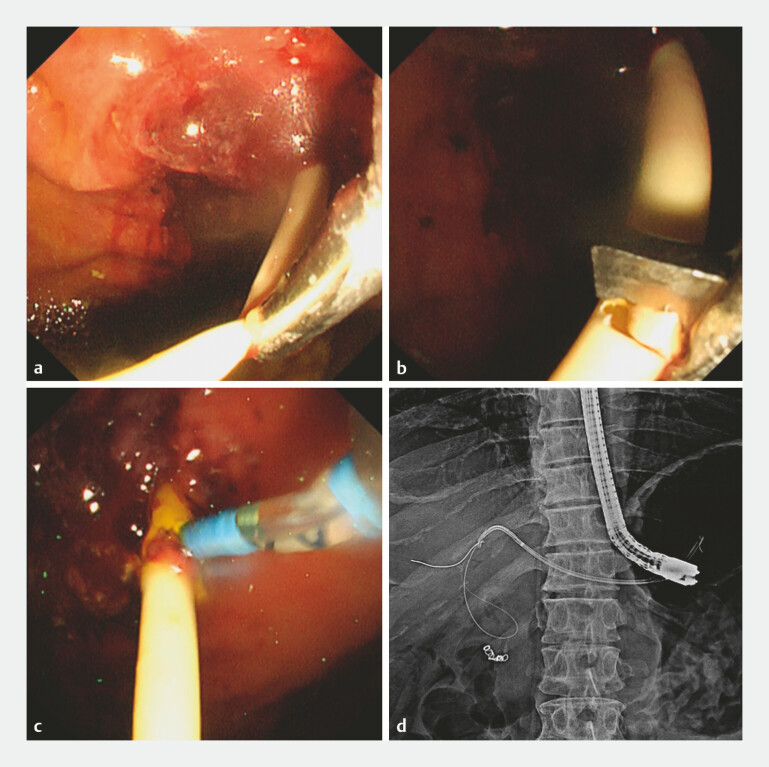 Fig. 2
Fig. 2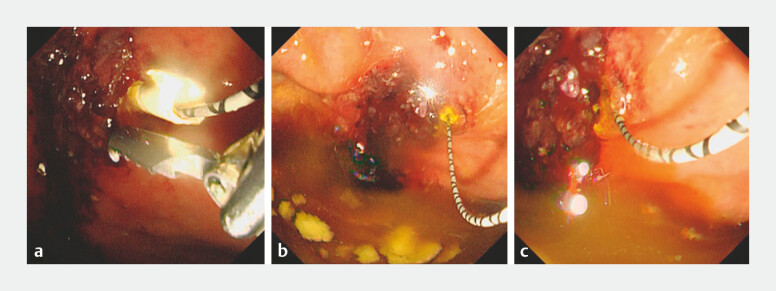 Fig. 3
Fig. 3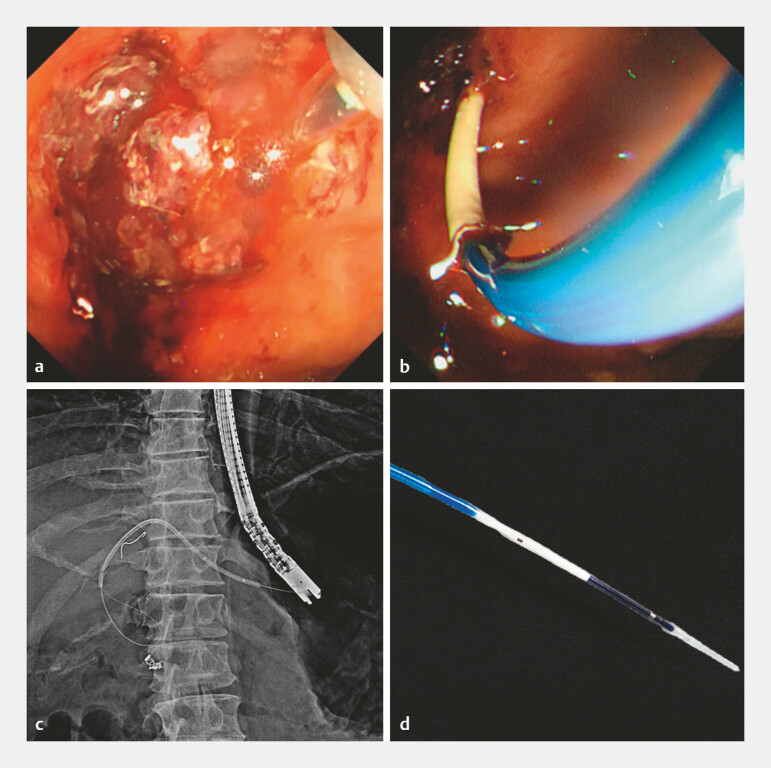 Fig. 4
Fig. 4- —National Cancer Center Research and Development Fund
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Esophageal and GI Pathology · Pediatric Hepatobiliary Diseases and Treatments
Endoscopic ultrasound-guided hepaticogastrostomy (EUS-HGS) has been widely performed; however, serious adverse events occasionally occur. For example, intraoperative or postoperative stent migration occurs in 2.68% of cases 1 . Retrieval by endoscopic approaches is often challenging. In this report, we present a case in which a completely migrated plastic stent (PS) into the intrahepatic bile duct (IBD) through EUS-HGS was safely retrieved endoscopically using a fine-gauge biliary dilation catheter ( Video 1 ).
Successful retrieval of migrated stent via endoscopic ultrasound-guided hepaticogastrostomy with fine-gauge dilation catheter.Video 1
A 56-year-old man with advanced pancreatic cancer presented with obstructive jaundice and underwent EUS-HGS using a 7 Fr PS ( Fig. 1 ). Two weeks later, he developed cholangitis due to stent dysfunction, requiring reintervention via the HGS route. To access the incomplete fistula, a side hole was created in the PS, and a guidewire (GW) was advanced into the IBD 2 ( Fig. 2 ). Subsequently, we attempted PS removal using alligator forceps, although the stent ruptured, leading to complete migration ( Fig. 3 ). Thus, a fine-gauge biliary dilation catheter (4-mm REN; Kaneka) was inserted into the migrated stent, and intraluminal balloon inflation allowed it to be firmly grasped. The PS was easily removed, and a new metallic stent was successfully placed ( Fig. 4 ). Postoperatively, cholangitis improved rapidly, and the patient was discharged without any adverse events.
Fluoroscopic images. a Endoscopic ultrasound-guided hepaticogastrostomy was performed for obstructive jaundice secondary to pancreatic head cancer. b We punctured the B3 site and inserted a 7 Fr plastic stent.
Endoscopic and fluoroscopic images. a Two weeks later, acute cholangitis occurred due to stent dysfunction. We attempted a stent exchange. b–d We cut through half of the plastic stent using a loop cutter to create a new side hole, and a guidewire was inserted.
Stent migration. a We attempted to remove the plastic stent using alligator forceps, which was difficult due to the large fluctuations in the endoscopic field of view caused by the patientʼs deep breathing. b, c Finally, the plastic stent migrated into the intrahepatic bile duct via the EUS-HGS. Abbreviation: EUS-HGS, endoscopic ultrasound-guided hepaticogastrostomy.
Migrated stent retrieval using a fine-gauge biliary dilation catheter. a–c We inserted a biliary dilation catheter into the migrated stent via EUS-HGS, dilated inside, and successfully removed the stent-balloon complex. d Biliary dilation catheter (4-mm, REN; KANEKA), with 2.7 Fr well-tapered distal ends for easy insertion into the plastic stent. Abbreviation: EUS-HGS, endoscopic ultrasound-guided hepaticogastrostomy.
Several methods have been reported for stent retrieval, including grasping with forceps, snares, and balloon dilation near the stent 3 4 5 . In this report, we used a biliary dilation catheter with a tapering tip, thin enough (2.7 Fr) for smooth insertion into a 7 Fr PS. The PS was removed as a complex with the catheter over the GW and through the endoscope, to minimize strain on the fistula and reduce the risk of GW deviation.
This is the first report of successful and safe retrieval of a migrated stent from the EUS-HGS route using this technique.
Endoscopy_UCTN_Code_TTT_1AS_2AH
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wang K Zhu J Xing L Assessment of efficacy and safety of EUS-guided biliary drainage: a systematic review Gastrointest Endosc 2016831218122710.1016/j.gie.2015.10.03326542374 · doi ↗ · pubmed ↗
- 2Hijioka S Sakamoto Y Nagashio Y Novel and safe plastic stent exchange method after endoscopic ultrasound-guided hepaticogastrostomy with incomplete fistula (side hole method)Endoscopy 202255 E 24E 2536113486 10.1055/a-1930-6319 PMC 9812677 · doi ↗ · pubmed ↗
- 3Saito T Hamada T Kogure H Digital cholangioscopy-guided retrieval of a migrated hepaticogastrostomy stent through a created hepaticogastrostomy route Endoscopy 202052 E 320E 32132106317 10.1055/a-1119-0987 · doi ↗ · pubmed ↗
- 4Miwa H Sugimori K Ozeki Y Biliary stent removal through a transgastric fistula created with endoscopic ultrasound-guided hepaticogastrostomy Clin J Gastroenterol 20211430430832710384 10.1007/s 12328-020-01184-7 · doi ↗ · pubmed ↗
- 5Ohno A Kaku T Fujimori N Spy basket retrieval method of an embedded hepaticogastrostomy stent (with videos)Endosc Ultrasound 20231216716810.4103/EUS-D-21-0021335899901 PMC 10134930 · doi ↗ · pubmed ↗