Successful resection of ampullary neuroendocrine tumors using clip traction-assisted hybrid endoscopic submucosal dissection
Ke Jiang, Justin Ryan Lay Tan, Weigang Gu, Qifeng Lou, Hangbin Jin, Jianfeng Yang, Xiaofeng Zhang

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
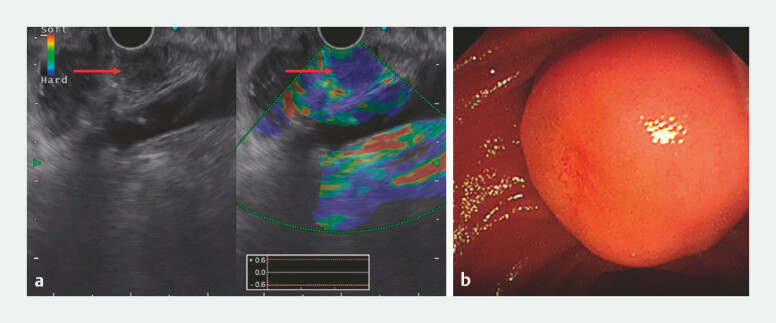 Fig. 1
Fig. 1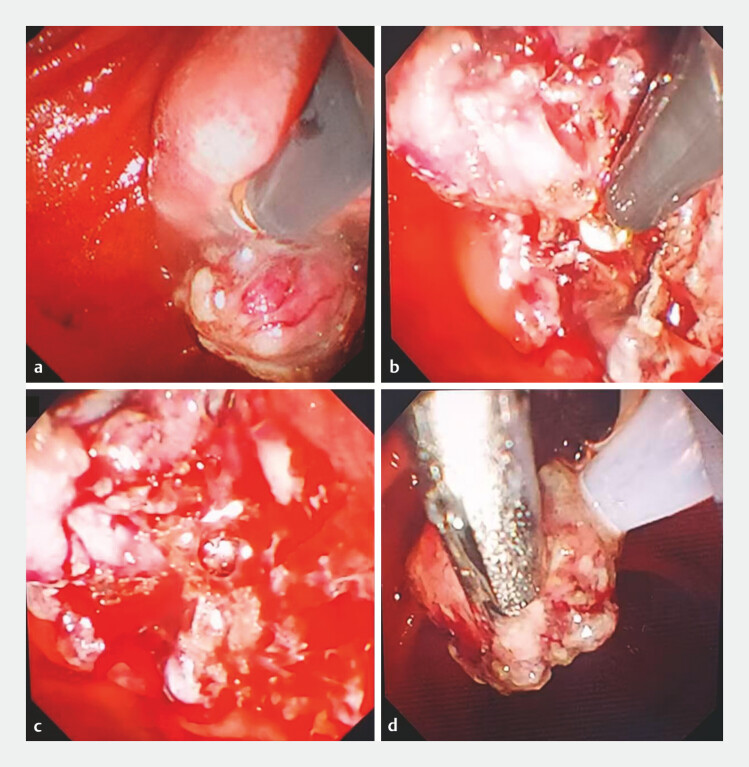 Fig. 2
Fig. 2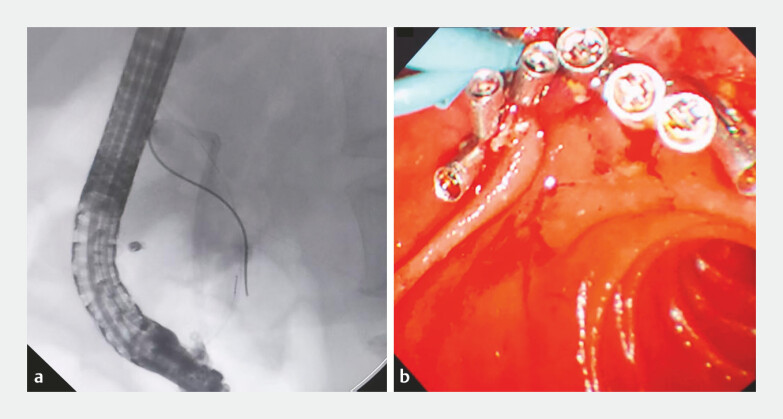 Fig. 3
Fig. 3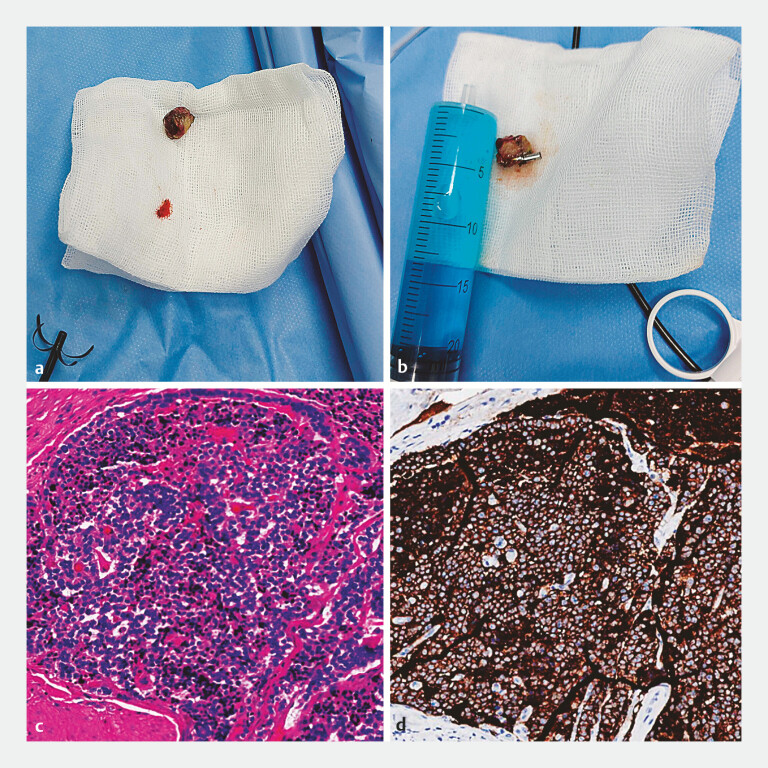 Fig. 4
Fig. 4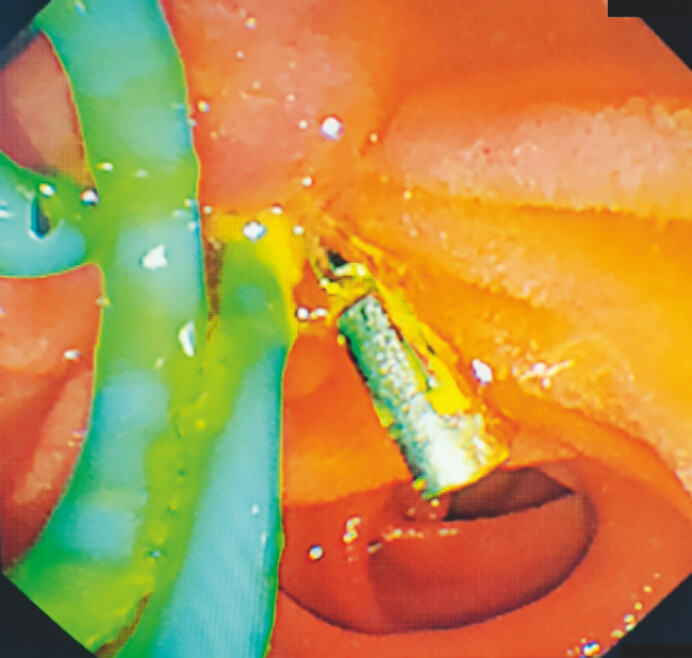 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeuroendocrine Tumor Research Advances · Metastasis and carcinoma case studies · Gastric Cancer Management and Outcomes
A 63-year-old man was referred due to a 1-month history of abdominal pain. Endoscopic ultrasound (EUS) and endoscopic retrograde cholangiopancreatography (ERCP) showed a 2.1 × 2.3 cm duodenal papilla submucosal tumor (SMT) with distinct borders ( Fig. 1 ). Endoscopic submucosal dissection (ESD) was initially planned. A submucosal injection of diluted methylene blue was performed, followed by a mucosal incision using a GoldKnife (Microtech Nanjing). This was followed by a layered multi-knife dissection (Gold Knife and IT Knife Nano) performed with clip traction assistance ( Fig. 2 a, b ). Due to anatomical challenges and bleeding, hybrid-ESD was adopted ( Fig. 2 c, d ). Placement of pancreatic and biliary stents for endoscopic retrograde pancreatic drainage (ERPD) and endoscopic retrograde biliary drainage (ERBD) and the post-resection defect were closed with a total of seven hemoclips. A nasobiliary tube was inserted to monitor the bleeding ( Fig. 3 , Video 1 ). The patient was discharged 7 days post-procedure.
EUS ( a ) and endoscopic image ( b ) showing the duodenal papilla submucosal tumor. Abbreviation: EUS, endoscopic ultrasound.
Surgical process images of hybrid ESD and EMR assisted by clip traction: a Using a Goldknife for submucosal dissection; b Using an IT Knife Nano for submucosal dissection; c Intraoperative bleeding resulted in blurred field of view, making it impossible to proceed with ESD for complete resection; d EMR of the partially dissected lesion. Abbreviations: ESD, Endoscopic submucosal dissection; EMR.
a ERCP was performed to insert a 7Fr single-pigtail biliary stent (3 cm) and a 7Fr single-pigtail pancreatic stent (7 cm) to prevent biliary stricture and pancreatitis, respectively; b A total of seven hemoclips (Micro-Tech) were deployed to close the post-ESD defect and a nasobiliary tube was inserted to monitor the bleeding. Abbreviation: ESD, endoscopic submucosal dissection.
Successfully resected neuroendocrine tumors in the ampulla using a combination of ESD and EMR with a clip-assisted traction.Video 1
The combined maximum diameter of the two specimens measured 1.9 cm ( Fig. 4 a, b ). Histopathology and immunohistochemistry showed a well-differentiated neuroendocrine tumor (NET), classified as G1 ( Fig. 4 c, d ), with tumor-free resection margins. Follow-up ERCP after 1 month demonstrated complete healing of the excision site, and random biopsy results were normal ( Fig. 5 , Video 1 ). The patient remained asymptomatic with no evidence of recurrence at the 12-month follow-up.
The combined widest diameter of the two specimens was 1.9 cm ( a, b ); Histopathology and immunohistochemistry showed a well-differentiated NET, classified as G1 ( c, d ). Abbreviation: NET, neuroendocrine tumor.
Image from follow-up duodenoscopy 1 month later showing complete healing of the resection site and no evidence of recurrence.
The unique anatomical features of the duodenum pose certain challenges to the implementation of ESD 1 2 3 4 . In this context, we highlight the utility of a single-clip-assisted traction technique combined with a novel hybrid-ESD approach for treating ampullary lesions. Our experience demonstrates that this technology effectively enhances surgical field exposure, thereby improving dissection efficiency and the overall resection rate. Additionally, it reduces risks such as bleeding and perforation.
Endoscopy_UCTN_Code_TTT_1AO_2AG_3AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kulkarni AS Karwat T Dubewar S Endoscopic resection of a large ampullary tumor using a hybrid endoscopic submucosal dissection and mucosal resection technique Endoscopy 20235501 E 1114 E 111510.1055/a-2173-722137802107 PMC 10558254 · doi ↗ · pubmed ↗
- 2Nabi Z Ramchandani M Asif S Outcomes of Endoscopic Submucosal Dissection in Duodenal Neuroendocrine Tumors J Gastrointest Surg 20222627527710.1007/s 11605-021-05133-834508292 · doi ↗ · pubmed ↗
- 3Nelsen EM Akhter A Benson MEEMR of large periampullary neuroendocrine tumor Video GIE 2017233610.1016/j.vgie.2017.08.00529916465 PMC 6003891 · doi ↗ · pubmed ↗
- 4Tashima T Nonaka K Kurumi H Successful traction-assisted endoscopic submucosal dissection using dental floss and a clip for a huge superficial nonampullary duodenal epithelial tumor with severe fibrosis (with video)JGH Open 2018317918131061895 10.1002/jgh 3.12118 PMC 6487824 · doi ↗ · pubmed ↗