Endoscopic management of recurrent sump syndrome after surgical choledochoduodenostomy: a stent through two orifices
Jonathan Rozenberg, Reid D. Wasserman, William F. Abel, Paul Yeaton, Patrick Okolo, Vivek Kesar, Varun Kesar

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Fig. 1
Fig. 1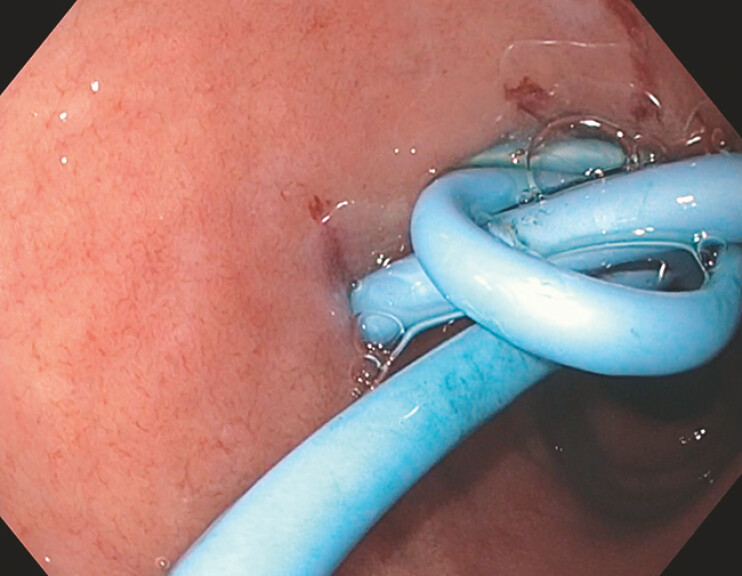 Fig. 2
Fig. 2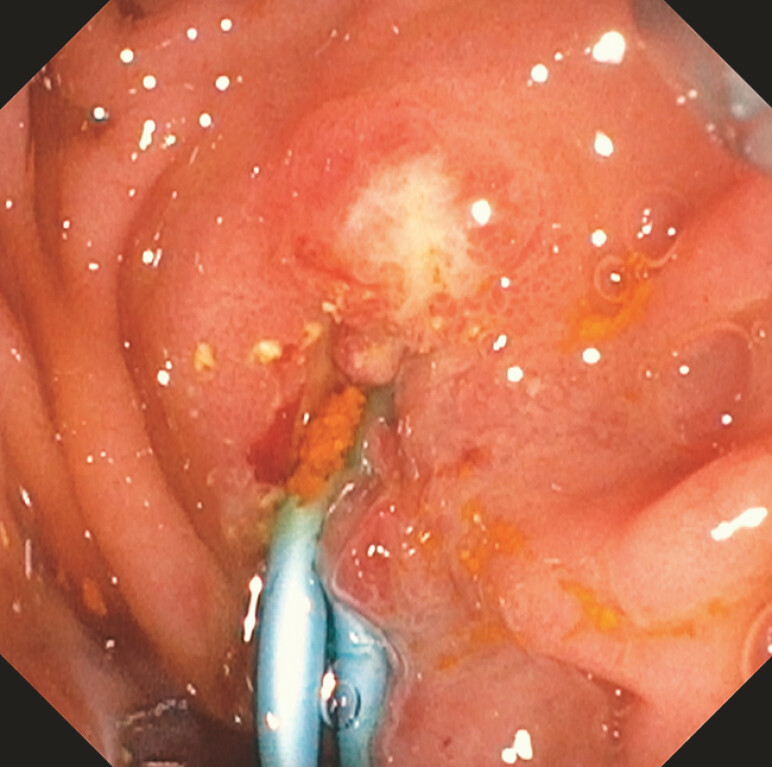 Fig. 3
Fig. 3 Fig. 4
Fig. 4 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Diaphragmatic Hernia Studies · Gastrointestinal disorders and treatments · Gastroesophageal reflux and treatments
A 78-year-old woman presented with recurrent choledocholithiasis. Her medical history included cholecystectomy and surgical choledochoduodenostomy (CDS), and choledocholithiasis consistent with sump syndrome (SS) status post endoscopic retrograde cholangiopancreatography (ERCP) with sphincterotomy, balloon sweep, and placement of a 10 mm × 10 cm fully covered self-expandable metal stent (fcSEMS) into the common bile duct (CBD). She underwent repeat ERCP with removal of the fcSEMs due to stent migration ( Fig. 1 ). Two plastic double-pigtail stents (PDPS; 10 Fr × 6 cm and 7 Fr × 7 cm, respectively) ( Fig. 2 , Fig. 3 ) were placed via a guidewire from the CDS across the papilla ( Fig. 4 ), effectively occluding both sites to prevent further recurrence of sump syndrome. In the 8 months since the procedure, she has remained asymptomatic.
Fluoroscopic image of a fully covered self-expandable metal stent, which migrated from the common bile duct into the choledochoduodenostomy.
Endoscopic image of a plastic double-pigtail stent placed into the choledochoduodenostomy site.
Endoscopic image of a plastic double-pigtail stent placed into the ampulla via the choledochoduodenostomy site.
Fluoroscopic image of successful guidewire passage from the choledochoduodenostomy site across the major papilla.
CDS refers to creation of a biliary-enteric anastomosis for the management of biliary stone pathologies and/or malignant biliary obstructions 1 . Consequently, the CBD limb distal to the CDS that extends to the ampulla of Vater, known as the “sump,” can amass stagnant debris, bile, and/or food ( Fig. 5 ), which when in the setting of impaired biliary drainage of the CDS can result in conditions such as ascending cholangitis, otherwise known as sump syndrome 1 2 . ERCP with sphincterotomy and/or debris removal is the mainstay of treatment; however, this does not preclude recurrence of sump syndrome and can necessitate repeat ERCPs and/or further surgical intervention (e.g. Roux-en-Y hepaticojejunostomy with distal CBD resection) 1 2 . The use of PDPS in treating sump syndrome has been documented in case reports wherein choledocholithiasis required the use of lithotripsy followed by PDPS placement into the CDS alone 3 4 . This case depicts successful management and prevention of further recurrence of sump syndrome through placement of two PDPS from a CDS through the major papilla ( Video 1 ).
Endoscopic image of a prior fully covered self-expandable metal stent occluded with debris, food obstructing biliary drainage from the choledochoduodenostomy.
Management and further prevention of sump syndrome via the use of two double-pigtail plastic stents at both the choledochoduodenostomy (CDS) and papilla in a patient with a history of surgical CDS with recurrent sump syndrome.Video 1
Endoscopy_UCTN_Code_TTT_1AR_2AK
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Qadan M Clarke S Morrow E Sump syndrome as a complication of choledochoduodenostomy Dig Dis Sci 2012572011201510.1007/s 10620-011-2020-422167692 · doi ↗ · pubmed ↗
- 2Abraham H Thomas S Srivastava A Sump syndrome: a rare long-term complication of choledochoduodenostomy Case Rep Gastroenterol 20171142843310.1159/00047733529033759 PMC 5624249 · doi ↗ · pubmed ↗
- 3Nakshabandi A Nakshabendi R Berry A Sump syndrome: keeping the diagnosis relevant in the ERCP-laden world: 140Am J Gastroenterol 2015110 S 59S 60
- 4Duarte-Chavez R Matin A Martinez-Tapia A 1344 Sump syndrome with massive choledocholithiasis requiring electrohydraulic lithotripsy Am J Gastroenterol 2019114 S 744