A new method of endoscopic ultrasound and cholangioscopy-guided gastroenterostomy
Cancan Zhou, Zheng Wang, Zheng Wu, Hao Sun, Jie Hao

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
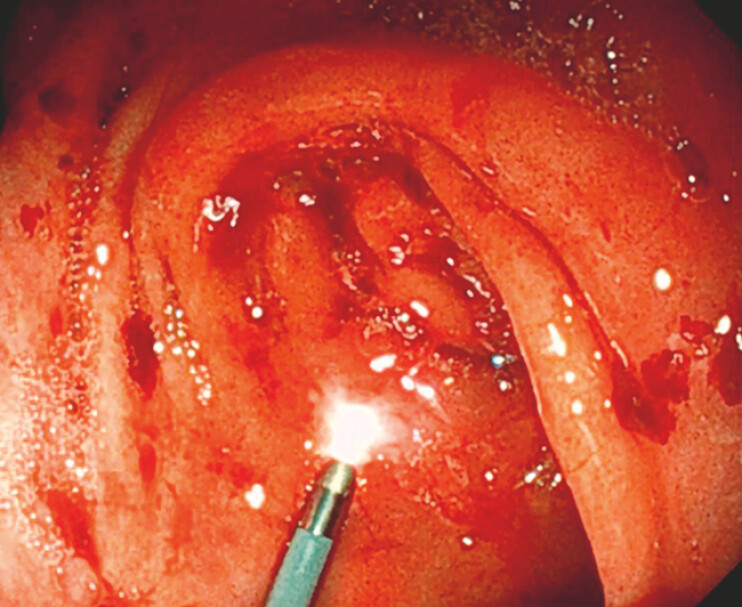 Fig. 1
Fig. 1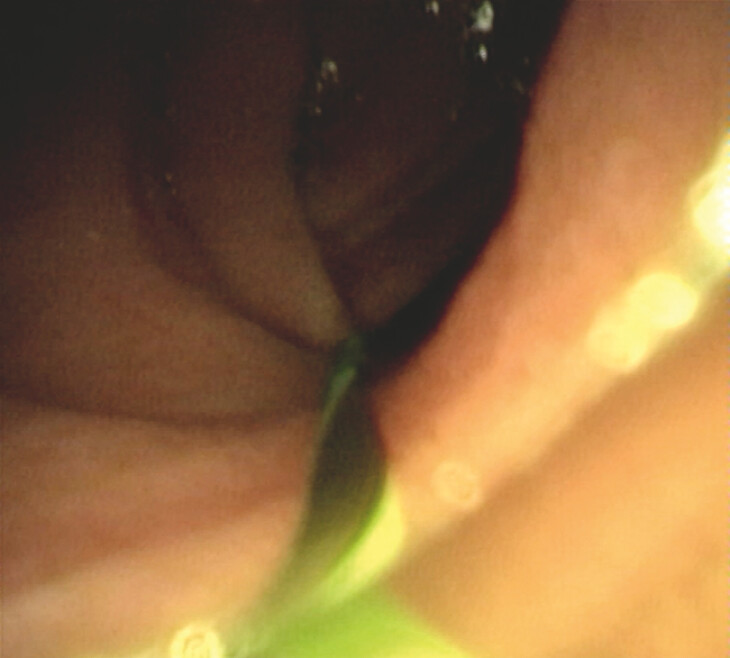 Fig. 2
Fig. 2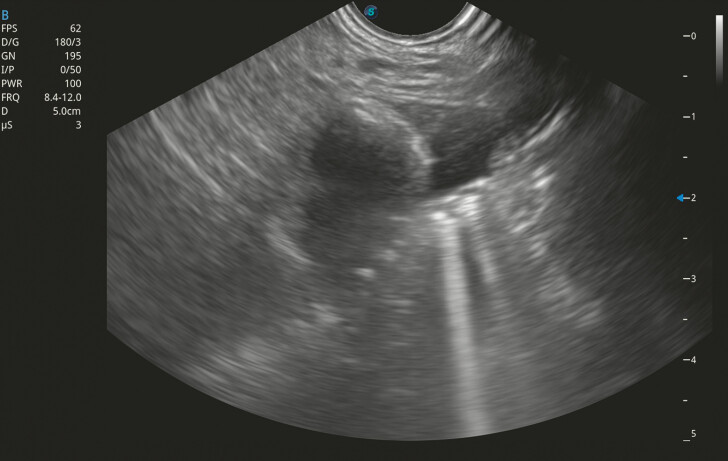 Fig. 3
Fig. 3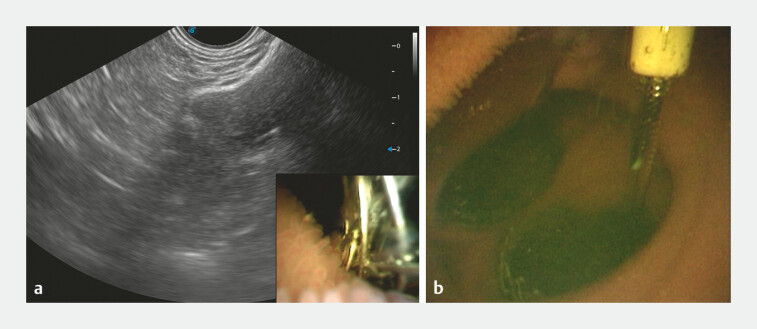 Fig. 4
Fig. 4 Fig. 5
Fig. 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Biliary and Gastrointestinal Fistulas · Gastrointestinal disorders and treatments
Endoscopic ultrasound (EUS)-guided gastroenterostomy (EUS-GE) using lumen-apposing metal stents (LAMS) has emerged as a promising minimally invasive approach for managing malignant gastric outlet obstruction 1 .
A 67-year-old man with pancreatic carcinoma presented with symptoms of gastric outlet obstruction. He was scheduled for EUS-GE under direct cholangioscopic guidance without X-ray. A 9-Fr cholangioscope (Micro-Tech, Nanjing, China) was advanced transnasally into the stomach and traversed the pylorus ( Fig. 1 ). Under the guidance of a 0.035-inch guidewire, the cholangioscope navigated through the stenotic duodenal bulb and distally to the jejunum ( Fig. 2 ). Simultaneous EUS imaging confirmed the location of the cholangioscope and dilated jejunum by water injection ( Fig. 3 ). A 20-mm LAMS (Hot AXIOS stent; Boston Scientific, Marlborough, Massachusetts, USA) was deployed through the gastric wall into the jejunum. Expansion of the distal flange was visualized in the cholangioscopic and EUS views. The electrocautery tip and the correct positioning and expansion of the distal flange in the jejunum were confirmed ( Fig. 4 ). Following deployment of the proximal flange, cholangioscopic methylene blue injection confirmed unimpeded stent patency with dye passage into the gastric lumen. After dilation of the LAMS, EUS-GE was completed without X-ray ( Video 1 ).
The cholangioscope was passed transnasally into the stomach and traversed the pylorus.
The cholangioscope passed through the obstruction into the jejunum under wire guidance.
Endoscopic ultrasound visualization showed the dilated jejunum and the scope sign.
Confirmation of the position of the distal flange and electrocautery tip. a Expansion of the distal flange was visualized both in cholangioscopic and endoscopic ultrasound views. b The electrocautery tip was seen in the jejunum.
The cholangioscope was advanced to the distal jejunum and expansion of the distal flange was confirmed by both cholangioscope and endoscopic ultrasound. Then, the gastroenterostomy was performed using a lumen-apposing metal stent without X-ray.Video 1
An upper gastrointestinal contrast study confirmed the patency of the stent ( Fig. 5 ). The patient tolerated a liquid diet and was discharged on postoperative day 4, with sustained clinical improvement.
Postoperative upper gastrointestinal radiography confirmed the patency of the stent.
Currently, EUS-GE techniques such as the balloon-occluded method and wire-guided electrocautery-enhanced stent placement (WEST) method aim to simplify the procedure, but the risks of misdeployment or inadvertent colonic anastomosis remain 2 3 . The WEST technique, despite its procedural streamlining, still reports adverse events including bleeding and perforation 4 . In contrast, our cholangioscopy-guided approach offers two key innovations. First, enhanced precision: cholangioscopic guidance allows immediate verification of LAMS deployment, reducing the risk of misplacement or collateral injury to adjacent organs. Second, real-time anatomic confirmation: direct cholangioscopic visualization eliminates reliance on fluoroscopy, mitigating radiation exposure for both patients and operators. This is particularly critical in minimizing cumulative radiation risks in recurrent procedural settings.
Endoscopy_UCTN_Code_TTT_1AS_2AG
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Van der Merwe S Wvan Wanrooij RLJ Bronswijk M Therapeutic endoscopic ultrasound: European Society of Gastrointestinal Endoscopy (ESGE) Guideline Endoscopy 20225418520510.1055/a-1717-139134937098 · doi ↗ · pubmed ↗
- 2Bronswijk Mvan Malenstein H Laleman WEUS-guided gastroenterostomy: less is more! The wireless EUS-guided gastroenterostomy simplified technique Video GIE 2020544210.1016/j.vgie.2020.06.012PMC 748241432954112 · doi ↗ · pubmed ↗
- 3Irani S Itoi T Baron THEUS-guided gastroenterostomy: techniques from East to West Video GIE 20195485032051906 10.1016/j.vgie.2019.10.007PMC 7004893 · doi ↗ · pubmed ↗
- 4Chen YI Kunda R Storm ACEUS-guided gastroenterostomy: a multicenter study comparing the direct and balloon-assisted techniques Gastrointest Endosc 2018871215122110.1016/j.gie.2017.07.03028750837 · doi ↗ · pubmed ↗