Intraductal papillary mucinous neoplasm with gastric penetration diagnosed using endoscopic imaging and aspiration cytology
Koichi Soga, Fuki Hayakawa, Mayumi Yamaguchi, Yo Fujimoto, Ryosaku Shirahashi, Ikuhiro Kobori, Masaya Tamano

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
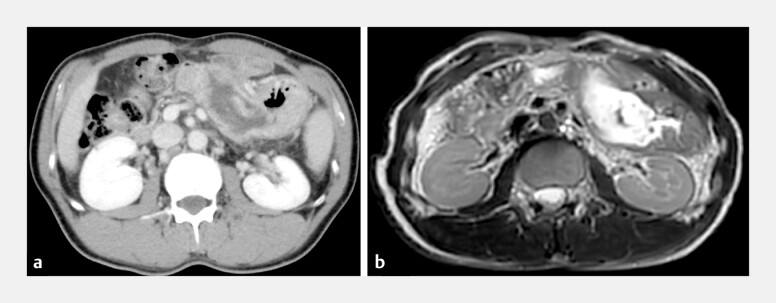 Fig. 1
Fig. 1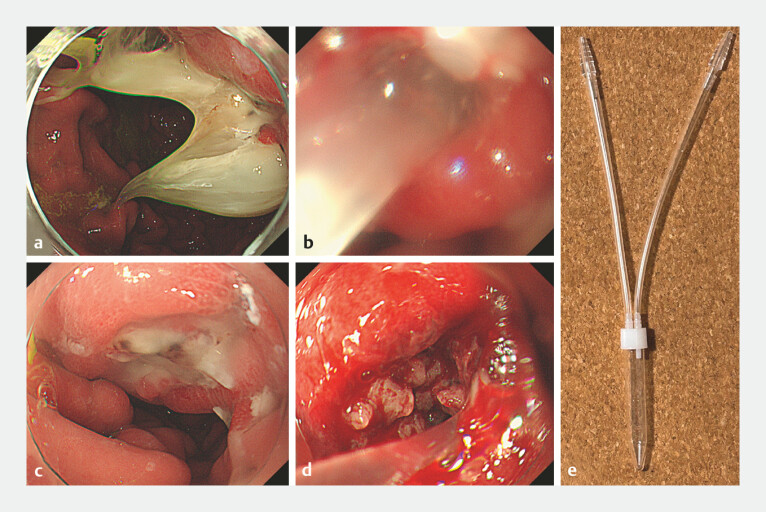 Fig. 2
Fig. 2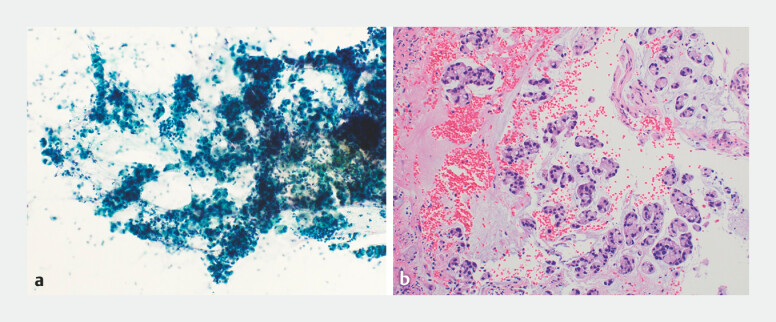 Fig. 3
Fig. 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatic and Hepatic Oncology Research · Gastrointestinal disorders and treatments · Gastrointestinal Tumor Research and Treatment
Intraductal papillary mucinous neoplasms (IPMNs) are cystic epithelial tumors arising in the pancreatic ductal system and characterized by intraductal papillary proliferation of mucin-producing neoplastic cells 1 . One rare complication of IPMNs is the formation of fistulas in adjacent organs, including the gastrointestinal tract. Cytological examination plays a pivotal role in the differential diagnosis of pancreatic cystic lesions, guiding clinical decision making and therapeutic strategies 2 .
A 48-year-old man with a history of chronic pancreatitis underwent pancreaticoduodenectomy 4 years before presentation. Follow-up abdominal imaging confirmed dilation of the remnant pancreatic duct suspected to be associated with malignant IPMN (mIPMN) and intragastric penetration of the IPMN through the pancreatic duct ( Fig. 1 ). We decided to perform an endoscopic procedure to examine the worsening IPMN.
Computed tomography (CT) and magnetic resonance imaging (MRI) of gastric penetration by intraductal papillary mucinous neoplasms (IPMNs). Contrast-enhanced CT (CE-CT) revealed a markedly dilated main pancreatic duct (MPD) and thin pancreatic tissue. a The tumor in the tail extended outside the pancreas, suggesting invasion of the stomach. b MRI confirmed the dilation of the MPD initially observed on CE-CT, with intraductal tumors with low signal intensity on T2-weighted images (T2-WI). The wall of the MPD and fistula showed high signal intensity on T2-WI.
Esophagogastroduodenoscopy revealed abundant mucus discharge from the stomach penetration site. We performed cytological analysis using endoscopic aspiration to collect the secreted mucus. Aspiration was performed using a material collection tube connected to an endoscope ( Fig. 2 ). After sufficient aspiration of a large amount of mucus, the papillary structure of the mIPMN was observed endoscopically.
Endoscopic imaging of intraductal papillary mucinous neoplasms (IPMNs) with gastric penetration and mucus discharge. a Esophagogastroduodenoscopy revealed gastropancreatic fistulas on the posterior wall of the gastric upper body and mucus discharged from the fistulas. b For cytological analysis, mucus was collected by endoscopic aspiration. c After sufficient aspiration and mucus removal using an endoscope, the stomach and pancreatic fistulas were observed endoscopically. d Insertion of the endoscope into the fistula revealed a papillary raised tumor. e The collection tube was connected to the endoscope under suction (SB-KAWASUMI, Kanagawa, Japan).
Approximately 30 mL of aspirated sample was subjected to cytological examination, revealing atypical glandular cells and abundant mucus adhesions (Papanicolaou stain, ×200). Biopsy of the papillary tumor performed after adequate mucus aspiration also showed cells with enlarged chromatin-dense nuclei. These findings were consistent with adenocarcinoma (hematoxylin and eosin stain, ×200). Based on these findings, mIPMN of the pancreas with a fistula penetrating the stomach was confirmed ( Fig. 3 , Video 1 ).
Cytological findings from aspirated mucus collected using endoscopy. a Collection of aspirated mucus revealed atypical mucus-covered glandular cells (Papanicolaou stain, ×200). b Biopsies of the papillary tumor performed after adequate mucus aspiration showed large and small clusters of tumor cells with enlarged chromatin-rich nuclei and pale acidophilic or foamy cytoplasm, accompanied by extracellular mucus; these findings were consistent with adenocarcinoma (hematoxylin and eosin stain, ×200).
Intraductal papillary mucinous neoplasm with gastric penetration diagnosed using endoscopic imaging and aspiration cytology.Video 1
In the present case, mIPMN penetrating the stomach was successfully diagnosed using aspiration cytology and endoscopy. Endoscopic imaging clearly depicted penetration of the IPMN into the gastric cavity, associated with significant mucus discharge. This case provides valuable insights into the diagnostic approach for this rare complication of IPMN and enhances our understanding of these neoplasms.
Endoscopy_UCTN_Code_CCL_1AZ_2AB
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tanaka M International consensus on the management of intraductal papillary mucinous neoplasm of the pancreas Ann Transl Med 2015328610.3978/j.issn.2305-5839.2015.11.0926697446 PMC 4671873 · doi ↗ · pubmed ↗
- 2Tacelli M Celsa C Magro B Diagnostic performance of endoscopic ultrasound through-the-needle microforceps biopsy of pancreatic cystic lesions: systematic review with meta-analysis Dig Endosc 2020321018103031912580 10.1111/den.13626 · doi ↗ · pubmed ↗