Angiocentric glioma in refractory epilepsy: when to suspect?
Angelo Dante de Carvalho Corrêa, Sérgio Ferreira Alves Júnior, Luis Alcides Quevedo Canete, Nina Ventura

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
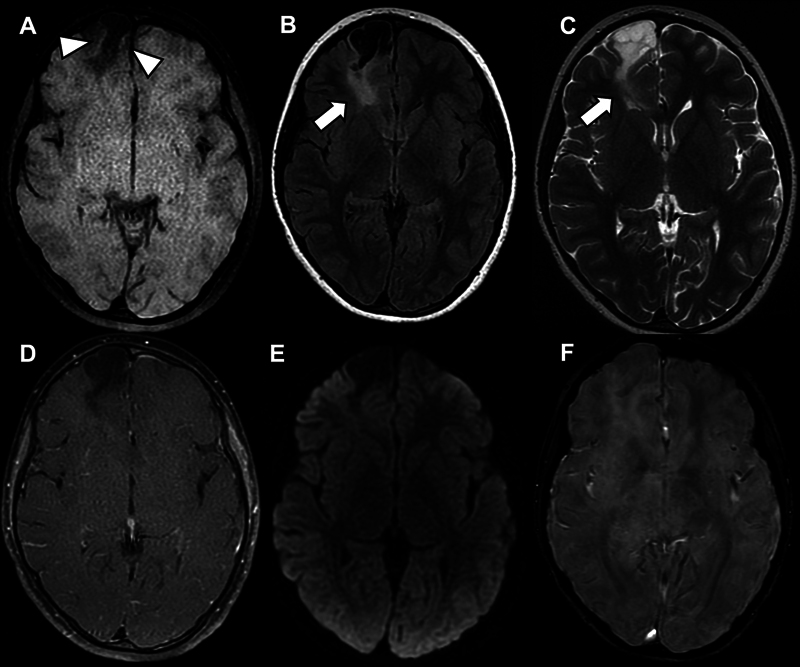 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlioma Diagnosis and Treatment · Epilepsy research and treatment · Meningioma and schwannoma management
A 9-year-old boy presented with partial seizures that had progressively worsened throughout the previous 4 months; the patient was refractory to oral medication. Magnetic resonance imaging (MRI) scans ( Figure 1 ) were performed, which demonstrated an expansive right frontal lesion, suggesting a tumor from the group of long-term epilepsy associated tumors (LEATs), with some findings suggestive of angiocentric glioma (AG), 1 2 confirmed after surgical resection.
Non-contrast T1-weighted imaging (T1-WI) ( A ) showing an expansive right frontal lesion with faint areas of hyperintense signal in its periphery (white arrowheads), a feature commonly observed in angiocentric glioma (AG). Fluid-attenuated inversion recovery (FLAIR) ( B ) and T2-weighted imaging (T2-WI) ( C ) showing a band of hyperintense signal extending from the lesion to the right lateral ventricle (Stalk-like sign; white arrows), which may represent tumor growth along the vessels. These two findings, within the clinical context, favored the diagnosis of AG. Moreover, the lesion did not present contrast enhancement on postcontrast T1-WI ( D ), neither foci of restricted diffusion ( E ) nor foci of bleeding or calcification in the susceptibility-weighted imaging (SWI) ( F ), findings that are usually absent in AG.
A rare World Health Organization (WHO) grade 1. pediatric-type. diffuse low-grade glioma, 3 AG is an epileptogenic lesion often observed in young patients. 4 The imaging findings ( Figure 1 ) may be characteristic and lead to radiological suspicion before surgery, 1 2 which can be essential for correct patient management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chen J Qi X Zhang M Zhang J Han T Wang C Cai C Review on neuroimaging in pediatric-type diffuse low-grade gliomas Front Pediatr 2023111.149646 E 610.3389/fped.2023.114964610.3389/fped.2023.1149646 PMC 1061914837920791 · doi ↗ · pubmed ↗
- 2Kurokawa R Baba A Emile P Kurokawa M Ota Y Kim J Neuroimaging features of angiocentric glioma: A case series and systematic review J Neuroimaging 2022320338939910.1111/jon.1298335201652 10.1111/jon.12983 PMC 9306893 · doi ↗ · pubmed ↗
- 3Louis D N Perry A Wesseling P Brat D J Cree I A Figarella-Branger D The 2021 WHO classification of tumors of the central nervous system: A summary Neuro-oncol 202123081231125110.1093/neuonc/noab 10634185076 10.1093/neuonc/noab 106PMC 8328013 · doi ↗ · pubmed ↗
- 4Bale T A Rosenblum M K The 2021 WHO Classification of Tumors of the Central Nervous System: An update on pediatric low-grade gliomas and glioneuronal tumors Brain Pathol 20223204 e 1306010.1111/bpa.1306035218102 10.1111/bpa.13060 PMC 9245930 · doi ↗ · pubmed ↗