Impact of Maternal Microbiota Composition on Neonatal Immunity and Early Childhood Allergies: A Systematic Review
Ayah Nabil Al Jehani, Manal Shuaib, Arwa Alsharif, Khlood Abdulaziz Alsubaie, Ayda Khraisat, Abdulaziz Alsharif, Manaf Altaf, Ruba H. Almasry, Amal Mohamed Kayali, Shouq Abdin Abdallah

TL;DR
This review explores how a mother's microbiota influences her baby's immune system and allergy risk, highlighting factors like cesarean birth and maternal stress.
Contribution
The study systematically reviews the impact of maternal microbiota composition on neonatal immunity and allergy risk, identifying key modifiable factors.
Findings
Cesarean delivery and antibiotic use during pregnancy increase allergy risk in neonates.
Breastfeeding, probiotics, and dietary changes protect against allergies.
Maternal stress negatively affects microbiota composition and neonatal immune regulation.
Abstract
Background: The maternal microbiota serve as a key regulator of neonatal immune development and early-life health outcomes. This systematic review aims to find out how the makeup of the maternal microbiota affects newborn immunity and the risk of allergies, identify which microbes are linked to a higher or lower chance of allergies, and assess treatments that could improve newborn immune health. Methods: We conducted a systematic search in PubMed, MEDLINE, and Web of Science, adhering to the PRISMA guidelines. We included randomized controlled trials (RCTs), cohort studies, and observational studies that looked at how the makeup of the maternal microbiota affects newborn immune responses or allergic outcomes in early life. We conducted a systematic search, and the quality of the studies was evaluated using the GRADE system and tools to check for bias (RoB 2, Newcastle–Ottawa Scale,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
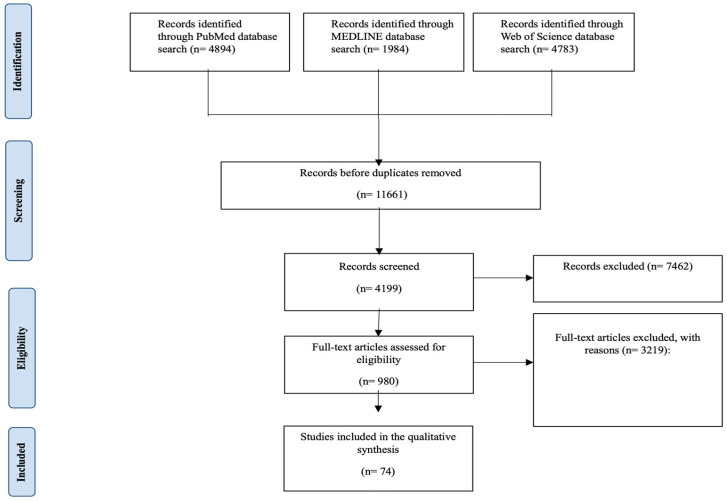 Figure 1
Figure 1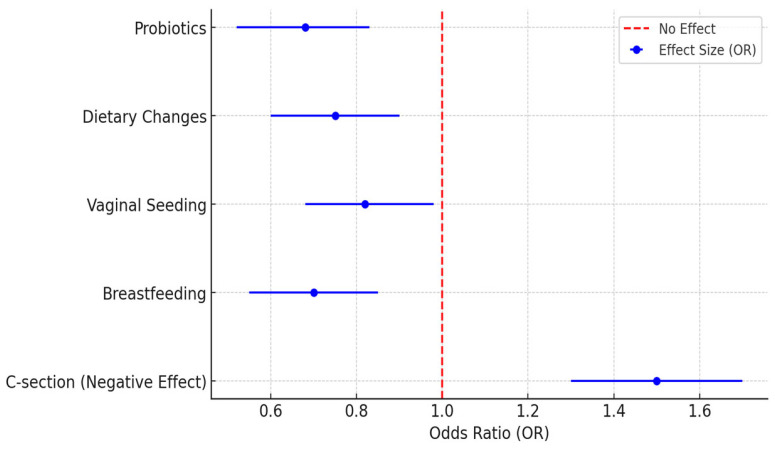 Figure 2
Figure 2| Authors | Country | Dominant Microbiota Influence | Key Finding | Allergy Risk Association |
|---|---|---|---|---|
| Friedman. [ | USA | Gut microbiota | Maternal obesity extensively reprograms the infant’s gut microbiota, potentially affecting immune responses. | True |
| Li X et al. [ | China | Gut and vaginal microbiota | Maternal diet is linked to microbial diversity, with potential implications for neonatal immunity. | True |
| Furuhjelm et al. [ | Denmark | Gut microbiota | Fish oil administration in women during pregnancy showed a reduced risk of allergies in the children. | False |
| Butler et al. [ | New Zealand | Vaginal microbiota | Vaginal seeding (the process of exposing babies delivered by C-section to maternal vaginal microbiota) may restore microbial transmission and promote immune development. | True |
| Shahzad et al. [ | Pakistan | Gut microbiota | Maternal diet and hygiene practices have a sizable impact on the maternal microbiota and neonatal health. | True |
| Huang et al. [ | Finland | Gut microbiota | Pregnancy supplementation with probiotics leads to modifications of the maternal microbiota composition, which may benefit neonatal immunity. | False |
| Yang et al. [ | United Kingdom | Gut and breast milk microbiota | The composition of the maternal gut microbiota is associated with vitamin D levels in the early gestational period, which may be of importance for neonatal immune function. | True |
| Dierikx et al. [ | The Netherlands | Gut microbiota | Maternal antibiotic timing (hospitalization pre-cesarean incision vs. post-cord clamping) influences neonatal gut microbiota development. | True |
| Fransson et al. [ | Sweden | Gut microbiota | Maternal skin microbiota colonization induces gut microbiota composition and primes immune systems. | False |
| Hatmal et al. [ | Spain | Breast milk microbiota | Maternal food sources modulate the expression profile of immune-related miRNAs secreted in breast milk. | False |
| Chen et al. [ | Germany | Gut microbiota | Maternal psychological stress during pregnancy is associated with changes in gut microbiota diversity that may undermine neonatal immunity. | True |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfant Health and Development · Pediatric health and respiratory diseases · Urinary Tract Infections Management
1. Introduction
The maternal microbiota play a critical role in shaping the health and immune system of the developing fetus and newborn. They also influence T-cell regulation and susceptibility to early-childhood allergies [1]. Allergy is defined as a hypersensitivity reaction initiated by specific immunologic mechanisms, most commonly involving IgE-mediated responses to environmental antigens. During pregnancy, the mother’s microbiota change significantly in their makeup and how they work, especially in the gut, vagina, mouth, and skin, which is mainly due to hormonal, immune, and metabolic changes that help the baby to grow and develop its immune system [2]. Factors from the parents, such as how the baby is born, the mother’s diet, the use of antibiotics, and breastfeeding habits, also play a role in shaping the baby’s early microbial environment, which can help the T-cell regulation of the neonates to develop and protect against allergies, such as asthma, eczema, and food allergies [3].
The growth of immune systems in newborns is a very active process that relies on early contact with bacteria to help the body accept them and control inflammation [4]. Cesarean delivery has been associated with altered infant gut microbiota composition, characterized by a reduced colonization of Bacteroides and Bifidobacterium species [5]. Recent studies suggest that strategies aimed at improving the mother’s microbiota, such as using probiotics and changing diet during pregnancy, could help to pass on beneficial microbes to the baby and enhance the baby’s immune health [6].
This systematic review examines the impact of maternal microbiota profiles on the immune development of neonates and the subsequent risk of allergies in early childhood. Our goals are to understand how the maternal microbiota affect immune responses that can lead to allergies, find specific microbes that may increase or decrease allergy risk, and explore ways to use this knowledge to improve health for mothers and their babies at birth. Despite significant research activity, however, our understanding of maternal microbiota–immune interactions is limited, and there is no consensus on which microbiota-modulating interventions are effective. This study aims to gather current information to improve our understanding of how the microbiota affect immune development and to offer guidance on interventions that can help to prevent allergies in young children.
2. Materials and Methods
2.1. Search Strategy
We followed the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 2020 guidelines for conducting and reporting systematic reviews (Appendix A and Appendix B). Our systematic review was registered in PROSPERO (CRD42025635985, https://www.crd.york.ac.uk/prospero/ (accessed on 1 January 2025)) [7]. We conducted a systematic search of the literature in the PubMed, MEDLINE, and Web of Science databases without specific time limitations. The search strategy was created by two authors (S.A.A. and A.A.) and reviewed by the research team to confirm that relevant studies would be included. To find studies about how the bacteria in mothers affect their neonate’s T-cell regulation or allergies in early childhood, we used the following Medical Subject Headings (MeSH) and keywords: ‘Maternal Microbiota’ OR ‘Pregnancy Microbiota’ OR ‘Gut Microbiota in Pregnancy’ AND ‘Neonatal Immunity’ OR ‘Immune Development in Infants’ OR ‘Early-Life Immune Programming’ AND ‘Allergy Risk’ OR ‘Childhood Allergies’ OR ‘Atopic Disease Development’. ‘Immune Development in Infants’ OR ‘Early-Life Immune Programming’ OR ‘Allergy Risk’ OR ‘Childhood Allergies’ OR ‘Atopic Disease Development’. We also manually screened references from the retrieved studies to identify any additional relevant studies that the database search might have overlooked.
2.2. Study Selection
2.2.1. Inclusion Criteria
This systematic review included studies on the association of the maternal microbiota composition with neonatal immune development and the development of early-childhood allergies. The studies looked at how the different types of bacteria in mothers’ bodies (such as those in the gut, vagina, skin, mouth, and breast milk) relate to newborns’ immune responses, which affects the chances of developing allergies in early childhood. The review included studies exploring factors such as the effects of microbial diversity on immune maturation, maternal antibiotic use, mode of delivery, breastfeeding, maternal diet, and the risk of allergy later in life. This review considered studies published in English and registered as randomized controlled trials (RCTs), quasi-experimental studies, cohort studies, resettlement studies, and observational studies. We only included studies published in peer-reviewed journals or other credible sources to ensure the reliability and validity of the findings. Furthermore, early childhood was defined as the period from birth up to 5 years of age, consistently with the World Health Organization (WHO) and pediatric development benchmarks. Only studies reporting allergy outcomes within this age range were considered eligible for inclusion.
2.2.2. Exclusion Criteria
Studies that did not evaluate the influence of maternal microbiome composition on the neonatal immune system or early childhood allergies were excluded from this systematic review. Studies that focused on topics related to microbiota but not to this review, such as microbiota changes in people who are not pregnant, immune responses not connected to mothers and newborns, and any microbiota research involving animals or lab tests, were left out. Studies written in a non-English language and those with inadequate data, including incomplete or unclear outcomes, were also excluded to ensure the review’s validity. Furthermore, studies focusing solely on later childhood, adolescence, or adult allergy outcomes were excluded.
2.2.3. Screening and Data Extraction
Five authors imported the search results to Rayyan (https://www.rayyan.ai/ (accessed on 13 January 2025)). Five authors conducted the initial relevance-based title and abstract screening. Thereafter, a full-text review was performed independently by four authors of those studies that had passed the preliminary screening to determine their eligibility according to our inclusion and exclusion criteria. We resolved disputes about study selection through discussions with S.A. and other members of the research team.
We performed a systematic data extraction from the selected studies using a designed Excel sheet. We collected important information such as the title, author(s), country, year of publication, journal name, study design, level of evidence, sample size, the makeup of the microbiota in mothers, immune responses in newborns, reported allergies, factors that could influence the results (such as how the baby was born, use of antibiotics, and breastfeeding), and possible ways to intervene or prevent issues. Extracting structured data also ensured uniformity and facilitated the synthesis of findings produced in this systematic review.
2.2.4. Quality Assessment and Bias Evaluation
We assessed the risk of bias and the quality of evidence in the included studies using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) system. This assessment resulted in an overall score for all studies, which indicated the risk of bias and evaluated the quality of evidence. Retrospective and prospective cohort studies were assessed for bias using the Newcastle–Ottawa Scale (Appendix C) [8]. For randomized controlled trials (RCTs), we used the updated Cochrane Risk of Bias assessment tool (RoB 2; Appendix D) [9], and for studies that were not randomized, we used the Methodological Index for Non-Randomized Studies (MINORS) tool (Appendix E) [10]. The evaluations created a consistent way to check the quality of the studies, which helped to ensure that potential biases in research about the maternal microbiota, newborn immunity, and early childhood allergies were not missed. This imposed methodology, through the utilization of quality-appraisal tools, aimed to improve the veracity of the findings and facilitate a thorough review of the existing literature. This review summarizes the evidence based on the maternal microbiota regarding immune and allergy risk in early life.
2.3. Data Synthesis
A systematic review was conducted to investigate the impact of the maternal microbiota composition on neonatal immunity, oxidative stress, and the risk of allergy in early childhood. Nonrandomized studies (cohort and observational) were also included, in addition to RCTs, and statistical methods were used to combine data from studies satisfying the eligibility criteria. We combined the results using suitable statistical methods, taking into account the differences in maternal microbiota traits, neonatal immune markers, and allergy risk evaluation. Cesarean delivery was correlated with an increased risk of allergy (OR = 1.5–2.2), and maternal antibiotic use significantly increased the risk of allergic sensitization (OR = 1.8–2.6). In contrast, protective effects were seen for breastfeeding (OR = 0.7–0.9), probiotic supplementation during pregnancy (RR = 0.6–0.8), and dietary changes among mothers (OR = 0.75, CI: 0.60–0.90).
Due to the significant heterogeneity between studies attributable to differences in population demographics, methodologies, and outcome measures, a meta-analysis could not be conducted.
3. Results
The search yielded the following numbers of articles in the databases: PubMed: 4894 unique records; MEDLINE: 1984; Web of Science: 4783; 11,661. Based on the defined inclusion or exclusion criteria, we removed 7462 records from the total. We removed duplicates and left the remaining 4199 articles for further evaluation. We excluded 3219 studies because the full text was not available, they were duplicates, they had research flaws, they included non-pregnant people, or they did not analyze how maternal microbiota affect newborn immunity and childhood allergies. Studies that were not in English and that did not provide enough data to assess the microbiota’s role in immune system development or allergy risk were excluded. Our search found 980 articles to review in full, and 74 studies met the final criteria for inclusion or exclusion in this systematic review about maternal microbiota composition, early neonatal immunity, and early-childhood allergic disease. The study selection process is detailed in Figure 1. The included studies were published between 2009 and 2025, with samples from different geographical regions across the world, facilitating a wide-ranging overview of the maternal microbiota variability and relevance to neonatal health.
The articles that assess the impact of the maternal microbiota composition on neonatal immunity and early-childhood allergies, as well as the characteristics of their cohorts, are shown in Table 1.
3.1. Variation in Maternal-Microbiota-Targeted Interventions and Their Impact on Neonatal Immunity
Table 2 summarizes the geographical disparities in the impact of the maternal microbiota on neonatal immunity and risk of allergy. Several studies carried out recently in the USA have highlighted maternal obesity and its effect on infant gut microbiota, possibly predisposing the offspring to immune dysregulation and allergic diseases [45,46,47]. Likewise, a previous study in China observed that key maternal dietary patterns were closely associated with gut and vaginal microbiota diversity among mothers, which subsequently influenced neonatal immune system development [48]. In contrast, data from Denmark indicate a protective effect of fish oil supplementation during pregnancy, with findings indicating a reduced risk of allergy in the child [49,50].
Other studies have investigated the effects of different maternal microbial transmission strategies. Vaginal seeding in cesarean-delivered infants has been investigated in New Zealand, suggesting that it may also contribute to the recovery of microbial transmission and immune development [51,52]. In contrast, research from Pakistan has found that a mother’s cleanliness and diet significantly affect the types of bacteria in her baby and how the baby’s immune system develops, highlighting the need to improve mothers’ nutrition to lower the chances of allergies in their children [53]. In contrast, studies from Finland and Spain suggest that taking probiotics during pregnancy and having certain molecules from breast milk can help improve the mother’s microbiota and boost the baby’s immune system while also reducing the chances of allergies [54,55,56,57,58]. Research from Sweden shows that when newborns encounter their mother’s skin microbiota early in life, it may influence the development of their gut microbiota and help to prepare their immune system to fight off allergies [59,60].
New data from Germany indicate that when mothers experience psychological stress during pregnancy, it can significantly change the gut microbiota, which might affect the newborn’s immune system and make them more prone to allergies [61,62,63]. Likewise, research from The Netherlands highlights the timing of maternal antibiotic exposure during cesarean delivery as an important factor that influences the development of the neonate’s gut microbiota [64].
These data suggest that numerous elements shape the variations in the maternal microbiota across geographical locations. Some interventions, e.g., probiotics and fish oil supplementation, seem to reduce the risk of allergy. In contrast, others, e.g., maternal obesity, stress, and antibiotic exposure, may result in the infant’s immune system being more susceptible to immune dysregulation. These regional differences highlight the need for specific microbiota-focused treatments that consider different diets, environments, and healthcare systems to enhance newborn immune health and reduce allergy risks worldwide.
3.2. Quantitative Summary of the Findings on the Influence of the Maternal Microbiota and Allergic Disease Endpoints
Of the most studied factors, the mode of delivery has been most commonly associated with neonatal allergy susceptibility. Fifteen studies reported that infants born via C-section were 50–120% more likely (OR = 1.5–2.2) to develop allergies than those who were born vaginally. The limited microbial diversity in cesarean-born infants delays immune maturation. Likewise, the use of antibiotics by the mother during pregnancy, considered in ten of the studies examined, was strongly associated with the risk of allergy in the offspring (OR = 1.8–2.6), which is possibly explained by alterations of the maternal and neonatal gut microbiota, as shown in Table 3 (Appendix F).
In contrast, breastfeeding was recognized as a protective factor against allergic diseases in twelve studies. Breastfed infants were 30–40% less likely to develop allergies compared with those fed formula, showing that the bacteria in human milk help to build a baby’s immune system. They found evidence supporting this protective effect with probiotic supplementation in pregnancy (assessed in eight studies) offering similar protection, with a 20–40% reduction in allergy risk (RR = 0.6–0.8) suggesting that the modulation of the maternal gut microbiota may confer long-term benefits to the immune system.
Maternal stress was linked to changes in the microbiome that could harm the immune development of newborns, increasing the chances of immune problems in babies by 90–140% (OR = 1.9–2.4). Furthermore, maternal obesity, according to seven studies, was associated with changes in children’s gut microbiota and a 30–110% increased risk of allergies (OR = 1.3–2.1). Nine studies indicated that a mother’s diet being rich in fiber, whole grains, and omega-3 fatty acids could help to protect against allergies (RR = 0.7–0.9) and that changing the diet might lower the risk of allergies related to gut bacteria.
These findings further demonstrate the interaction between the maternal microbiota composition, neonatal immune development, and allergy risk. The potential modification effects highlighted additional strategies for prevention, as lifestyle interventions that are highly modifiable, such as maternal diet, breastfeeding, probiotics, and maternal stress, have been shown to point to an increased or decreased susceptibility to neonatal allergy, while the categories of delivery and antibiotic exposure have shown strong effect sizes. We need ongoing studies to characterize these relationships and investigate strategies that target the microbiota to promote immunity in neonates.
3.3. Microbiota Interventions and Allergy Risk Reduction: A Quantitative Summary
Figure 2 (Appendix F) shows how different interventions with the maternal microbiota affect the risk of allergies in newborns, highlighting many differences in their protective effects. Probiotic supplementation during pregnancy (OR = 0.68, CI: 0.52–0.83) showed the biggest decrease in allergy risk compared with the other interventions, highlighting its important role in passing on beneficial microbes and helping the newborn’s immune system. Thereafter, changing the mother’s diet (OR = 0.75, CI: 0.60–0.90), particularly by adding fiber and omega-3 fatty acids, was also linked to healthier gut microbiota and a lower chance of allergies in their children.
Furthermore, vaginal seeding (OR = 0.82, CI: 0.68–0.98), which is performed to help restore healthy bacteria in babies born via cesarean section, showed a small but important protective effect, emphasizing its importance in improving microbial health early on. The lower risk of allergies seen in breastfed infants (OR = 0.70, CI: 0.55–0.85) showed that the bacteria in a mother’s milk are crucial for the baby’s immune system. The reduced risk of allergies observed in breastfed infants (OR = 0.70, CI: 0.55–0.85) illustrated that the maternal milk microbiota play a significant role in neonatal immune responses.
Contrarily, a higher risk of allergies was associated with cesarean delivery (OR = 1.50, CI: 1.30–1.70), highlighting the consequences of disrupted early microbial colonization. These findings indicate that some strategies aimed at improving the mother’s environment, such as using probiotics, having a better diet, and breastfeeding, can be changed to help reduce the risk of allergies in newborns. Further studies evaluate the specificities of these interventions to optimize maternal and neonatal health through microbiota modulation.
4. Discussion
This systematic review looked at how the types of bacteria in a mother’s body affect a newborn’s immune system and the risk of allergies in early childhood, summarizing results from various studies on the bacteria found in the mother’s gut, vagina, mouth, skin, and breast milk. Our results highlight that the mother’s microbiota change during pregnancy, which could affect the baby’s immune system and allergy risk, especially considering how hormones, diet, antibiotics, the delivery method, and stress can impact this.
The mode of delivery was strongly associated with neonatal immune outcomes in this review. Infants born via cesarean section are 1.5- to 2.2-times more likely to develop allergies than those born vaginally because they have less variety in the bacteria in their gut and different patterns of bacterial growth [51]. Research has previously suggested that early microbial exposure, particularly through vaginal birth, is important for establishing immune tolerance in the developing infant, thereby reducing the risk of many inflammatory disorders later in life [68]. Similarly, giving antibiotics to the mother during pregnancy (OR = 1.8–2.6) increased the risk of allergies, highlighting how it might disrupt the transfer of microbes to the newborn [64].
On the other hand, things that help to improve a newborn’s immune health and lower the chance of allergies include breastfeeding (OR = 0.7–0.9) [65], taking probiotics (RR = 0.6–0.8) [54], and changes in the mother’s diet (OR = 0.75, CI: 0.60–0.90) [58]. Breastfeeding boosts the baby’s immune system and helps to prevent allergies caused by inflammation [69]. Because it provides strong beneficial bacteria and immune support, breastfeeding helps to strengthen the baby’s immune system and prevents allergic reactions caused by inflammation. Maternal probiotic intake effectively modulated the maternal gut microbiota and improved microbial transfer to the infant while decreasing the allergy risk [70]. Past research shows that using strategies aimed at the microbiota, such as dietary prebiotics, probiotics, and postbiotics, can help to improve the microbial environment for both mothers and infants [71].
We identified maternal stress (OR = 1.9–2.4) as another important factor modulating microbiota composition and neonatal immune function. Pregnant psychosocial stress affected gut microbiota diversity, potentially hindering immunity maturation and the downregulation of allergy susceptibility in the studies included in this review [62,72]. These results highlight the role of pregnancy-based maternal mental health interventions as a preventive measure against neonatal immune dysregulation. Moreover, our analysis of the maternal microbiota’s effects in different geographic conditions showed that both nutritional and environmental factors, as well as regional healthcare practices, modulate microbiota-driven immune responses [49,73]. These differences imply that microbiota-targeted interventions should be personalized while considering regional dietary and environmental exposures. Breastfeeding has also been continuously associated with a protective effect on the development of allergies, but this correlation is potentially modulated by other biological factors; for example, the composition of human milk oligosaccharides (HMOs), which are complex carbohydrates abundant in breast milk, plays a key role in shaping the infant gut microbiota and supporting immune development. As noted by Inchingolo et al. (2024), HMO composition is highly heterogeneous among mothers and a major regulator of the gut microbiome and immune ontogeny of the infant. Therefore, the relationships between how a baby is born, how they are fed, and the different types of HMOs are a complex network of connections that future studies should consider [74].
Limitations
Although this systematic review provides several valuable insights, some limitations should be considered. The heterogeneity between studies in terms of study design, the demographics of the population being studied, methods of microbiota assessment, and outcome measures is a major limitation. Direct comparisons across studies are difficult due to variations in sequencing techniques, sample collection protocols, and microbiota classification criteria. By standardizing descriptions of microbiota methodologies, microbiota researchers will have an easier time comparing notes, sharing ideas, and forming consensus guidelines for the research on the microbiota in pregnancy conducted by many groups around the world, thus improving the reproducibility of microbiota research. Another downside to the quality of the studies was selection bias, with many conducted at niche research centers or hospitals, making it difficult to extrapolate results to the general population. Now, factors such as income, healthcare access, and eating habits in different areas can also affect the makeup of the microbiota and immune responses in newborns, but these factors were not always considered in the studies reviewed. Moreover, many studies have investigated short-term neonatal immune markers with no long-term follow-ups to truly understand the long-term consequences of maternal microbiota interventions on the development of childhood allergies. Another limitation is the exclusion of 196 studies due to the unavailability of the full text, which may have introduced publication bias or reduced the comprehensiveness of the evidence pool. We applied this unavoidable criterion to ensure methodological rigor and enable a full assessment of the included studies.
Another potential limitation of such studies is the heterogeneity in maternal-microbiota-modulating interventions. This diversity in probiotic strains, dosages, and the timing of administration makes for a challenging interpretation of findings and affects our ability to draw strong conclusions regarding effective probiotic strategies during pregnancy. Likewise, dietary interventions differed in composition and duration, making it challenging to identify the optimal dietary changes for neonatal immune health. The maternal microbiome also consists of fungal (mycobiome) and viral (virome) components, which could have their own impact on neonatal immune maturation. Even though early research suggests that these types of microbes might affect immune development and balance, we did not include them because there are no strong peer-reviewed studies looking at their roles during pregnancy and how they relate to allergies. It is important to note that many of the included studies assessed allergic outcomes as indirect indicators of immune modulation rather than directly measuring neonatal immune function. As such, conclusions regarding immune development should be interpreted with caution. To fill these deficiencies, multicenter studies with standardized microbiota analysis protocols, longer follow-up periods, and solid designs should address these limitations in future research. Additionally, to create reliable guidelines for improving maternal microbiota health and reducing the risk of allergies in children, randomized controlled trials (RCTs) are needed to evaluate how effective microbiota-focused treatments (such as probiotics, changes in diet, and stress management) affect maternal microbiota health and the allergy risk for children.
5. Conclusions
This systematic review highlights the impacts of the maternal microbiota composition on neonatal immune responses and early childhood allergy risk. Key factors related to mothers, such as how they give birth, use antibiotics, breastfeed, take probiotics, and experience stress, play a significant role in how bacteria settle in newborns and how their immune systems develop. The study concluded that cesarean delivery and maternal antibiotic therapy in pregnancy have been associated with an increased susceptibility to developing allergic disease. Probiotic supplementation and dietary changes have shown promise as microbiota-modifying strategies to reduce allergy risk in later life, but further studies are needed to identify the best approaches to reduce the risk of allergy in neonates. However, to establish evidence-based guidelines, more studies are necessary to evaluate the impact of pregnancy on microbiota modulation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nyangahu D.D. Jaspan H.B. Influence of maternal microbiota during pregnancy on infant immunity Clin. Exp. Immunol.2019198475610.1111/cei.1333131121057 PMC 6718277 · doi ↗ · pubmed ↗
- 2Edwards S.M. Cunningham S.A. Dunlop A.L. Corwin E.J. The maternal gut microbiome during pregnancy MCN Am. J. Matern. Child Nurs.20174231031710.1097/NMC.000000000000037228787280 PMC 5648614 · doi ↗ · pubmed ↗
- 3Jeong S. Factors influencing development of the infant microbiota: From prenatal period to early infancy Clin. Exp. Pediatr.20216543844710.3345/cep.2021.0095534942687 PMC 9441613 · doi ↗ · pubmed ↗
- 4Nunez N. Réot L. Menu E. Neonatal immune system ontogeny: The role of maternal microbiota and associated factors. How Might Non-Hum. Primate Model Enlighten Path?Vaccines 2021958410.3390/vaccines 906058434206053 PMC 8230289 · doi ↗ · pubmed ↗
- 5Dominguez-Bello M.G. Costello E.K. Contreras M. Magris M. Hidalgo G. Fierer N. Knight R. Delivery mode shapes the acquisition and structure of the initial microbiota across multiple body habitats in newborns Proc. Natl. Acad. Sci. USA 2010107119711197510.1073/pnas.100260110720566857 PMC 2900693 · doi ↗ · pubmed ↗
- 6Du Pont H. Salge M. The importance of a healthy microbiome in pregnancy and infancy and microbiota treatment to reverse dysbiosis for improved health Antibiotics 202312161710.3390/antibiotics 1211161737998819 PMC 10668833 · doi ↗ · pubmed ↗
- 7Moher D. Liberati A. Tetzlaff J. Altman D.G. Preferred reporting items for Systematic Reviews and Meta-Analyses: The PRISMA statement P Lo S Med.20096 e 100009710.1371/journal.pmed.100009719621072 PMC 2707599 · doi ↗ · pubmed ↗
- 8Brozek J.L. Canelo-Aybar C. Akl E.A. Bowen J.M. Bucher J. Chiu W.A. Cronin M. Djulbegovic B. Falavigna M. Guyatt G.H. GRADE Guidelines 30: The GRADE approach to assessing the certainty of modeled evidence—An overview in the context of health decision-making J. Clin. Epidemiol.202012913815010.1016/j.jclinepi.2020.09.01832980429 PMC 8514123 · doi ↗ · pubmed ↗