Impostor phenomenon and psychological outcomes among family medicine residents: a cross-sectional study in Croatia
Sunčana Vlah Tomičević, Valerija Bralić Lang

TL;DR
This study found that many family medicine residents in Croatia experience impostor feelings, which are strongly linked to depression, anxiety, and stress.
Contribution
The study is one of the first to explore the impostor phenomenon in Croatian family medicine residents and its association with mental health outcomes.
Findings
59 out of 79 residents reported impostor feelings, which were significantly linked to higher depression, anxiety, and stress scores.
All participants with high impostor feelings also had clinically relevant symptoms of depression, anxiety, and stress.
The study suggests early interventions like peer support and self-compassion could help mitigate these negative outcomes.
Abstract
The aim of this cross-sectional study was to determine the prevalence of the impostor phenomenon among family medicine residents (FMRs) and its connection with sociodemographic factors and clinically relevant symptoms of depression, anxiety, and stress. During July 2023, 158 first-year FMRs were invited to fill out an anonymous online questionnaire containing sociodemographic data, history of psychiatric disorders, Clance Impostor Phenomenon Scale (CIPS), and the 21-item Depression Anxiety Stress Scale (DASS-21). Seventynine participants responded (50 % response rate) and 59 reported some level of impostor feelings. Clinically relevant symptoms of depression were reported by 17, anxiety by 23, and stress by 20 participants. All 59 participants whose responses indicated impostor feelings above normal also had higher scores for depression, anxiety, and stress (p<0.001 in Mann-Whitney U…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
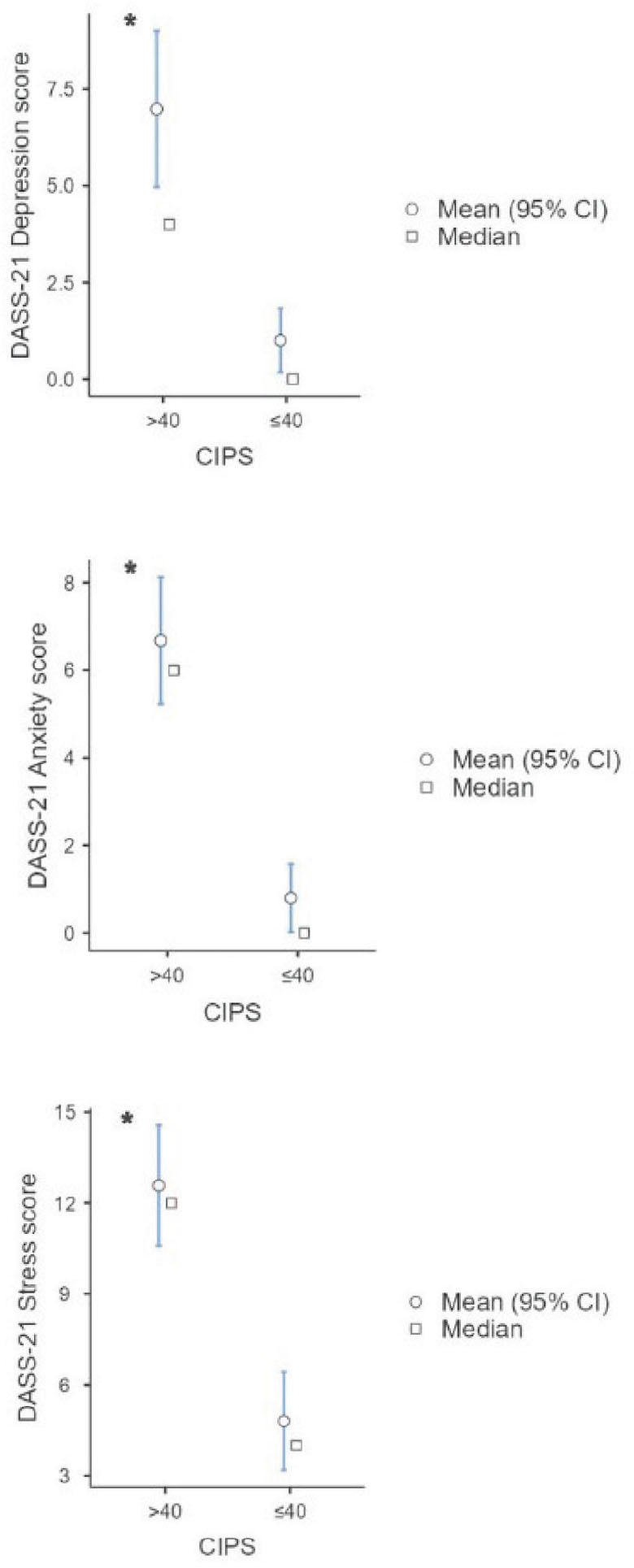 Figure 1
Figure 1|
| ||
|---|---|---|
| Partner | ||
| Yes | 5 | 36 |
| No | 9 | 29 |
|
| ||
| Children | ||
| Yes | 1 | 21 |
| No | 13 | 44 |
|
| ||
| Mental illness | ||
| Yes | 2 | 4 |
| No | 12 | 61 |
|
| ||
| School of medicine as first choice | ||
| Yes | 14 | 60 |
| No | 0 | 5 |
|
| ||
| Family medicine residency as first choice | ||
| Yes | 13 | 59 |
| No | 1 | 6 |
|
|
|
|
|
|---|---|---|---|
| Few ≤40 | 20 | 31.5 (21–40) | 28.1–33.3 |
| Moderate 41–60 | 33 | 48 (41–60) | 46.7–50.5 |
| Frequent 61–80 | 19 | 66 (62–80) | 66.0–72.0 |
| Intense >80 | 7 | 89 (81–99) | 81.9–93.8 |
|
|
|
|
|
|
|
|
|---|---|---|---|---|---|---|
| Depression | 62 | 5 | 9 | 1 | 2 | 2 (0–34) |
| Anxiety | 56 | 5 | 14 | 2 | 2 | 4 (0–24) |
| Stress | 59 | 6 | 12 | 1 | 1 | 10 (0–38) |
|
|
|
| |
|---|---|---|---|
|
| |||
| Gender | |||
| Male/Female | 0.54 | 0.16–1.86 | 0.329 |
| Partner | |||
| Yes/No | 0.36 | 0.12–1.07 | 0.066 |
| Children | |||
| Yes/No | 0.34 | 0.12–1.01 | 0.053 |
| Mental illness | |||
| Yes/No | 1.76 | 0.19–16.03 | 0.616 |
|
| |||
| Gender | |||
| Male/Female | 0.99 | 0.24–4.05 | 0.993 |
| Partner | |||
| Yes/No | 0.42 | 0.14–1.28 | 0.128 |
| Children | |||
| Yes/No | 0.75 | 0.22–2.62 | 0.655 |
| Mental illness | |||
| Yes/No | 4.21 | 0.77–23.14 | 0.098 |
|
| |||
| Gender | |||
| Male/Female | 0.35 | 0.07–1.70 | 0.193 |
| Partner | |||
| Yes/No | 1.02 | 0.38–2.68 | 0.975 |
| Children | |||
| Yes/No | 0.88 | 0.29–2.64 | 0.823 |
| Mental illness | |||
| Yes/No | 1.24 | 0.21–7.28 | 0.813 |
|
| |||
| Gender | |||
| Male/Female | 1.22 | 0.34–4.45 | 0.758 |
| Partner | |||
| Yes/No | 0.89 | 0.25–1.91 | 0.476 |
| Children | |||
| Yes/No | 0.57 | 0.17–1.94 | 0.369 |
| Mental illness | |||
| Yes/No | 0.57 | 0.06–5.18 | 0.616 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPerfectionism, Procrastination, Anxiety Studies · Anxiety, Depression, Psychometrics, Treatment, Cognitive Processes · Healthcare professionals’ stress and burnout
Mental health difficulties are common among doctors, especially women and young doctors (1). Some conditions like impostor phenomenon or syndrome (IP) can affect mental health, and physicians seem to be more susceptible to it, especially during residency (2,3,4). IP was first described by Clance and Imes (5) in 1978 as a feeling that one’s own success is owed to luck or a mistake or other reason rather than one’s own merit. Hence the feeling of being a fraud. IP is not considered a mental illness but a set of personality characteristics that can heighten during schooling and lead to over-preparedness or procrastination by working overtime to meet the last-minute deadline (4, 6). It starts at a young age, increases during schooling, especially if problems or difficulties are not addressed properly, and is considered prominent among young people, highly successful individuals, women, and minority groups (7, 8).
In Croatia, family medicine residents (FMRs) often work as the sole responsible physicians in family medicine for several years, even before beginning their residency. Since they start working in general practice immediately after completing medical school, they lack necessary education and skills to function as independent family medicine doctors. Administrative burden and high patient load they face pose a risk of poor mental outcomes as they exact high mental strain and a feeling of displacement, which favours the occurrence of IP (9, 10). Since young doctors have a higher prevalence of burnout, anxiety, and depression, a pre-existing condition like IP should be considered as a possible contributor to these negative mental states (11).
The aim of our cross-sectional study was to test this hypothesis by determining the prevalence of IP among first-year FMRs and its association with clinically relevant symptoms of depression, anxiety, and stress.
PARTICIPANTS AND METHODS
For this anonymous survey we invited 158 first-year FMRs in Zagreb, Croatia in July 2023. Only the first-year FMRs were included, because IP is more prominent in younger doctors, and they all attended the theoretical part of the specialisation and were available for this study (2).
The participants were recruited via email with a link to the web version of the questionnaire. All the invited participants were instructed to fill the survey only once. After three reminders, we closed the survey, having received completed questionnaire from 79 respondents (50 % response rate).
The survey was approved by the University of Zagreb School of Medicine Ethics Committee (approval No. 251-59-10106-24-111/150 of 9 October 2023).
Questionnaire
The questionnaire we developed specifically for this study is in Croatian and designed to collect sociodemographic data (age, gender, years of work, partner status, having children or not), history of psychiatric disorders, and whether the study of medicine and specialisation in family medicine were the participants’ first career choice.
Additionally, the questionnaire incorporated two instruments: the 20-item Clance Impostor Phenomenon Scale (CIPS) and the 21-item Depression Anxiety Stress Scale (DASS-21). We used the Croatian version of CIPS (12) to determine the level of IP in respondents as described by Clance (13). Each item is answered on the Likert scale from 1 (not true at all) to 5 (very true) and each score added. If the total score is 40 or less, the respondent seldom has impostor feelings; a score between 41 and 60 corresponds to a moderate frequency of IP experience; a score between 61 and 80 indicates that the respondent often has impostor feelings; and a score higher than 80 means the respondent often has intense impostor feelings. DASS-21 quantifies symptoms of depression (severity cut-off score >9), anxiety (cut-off score >7), and stress (cut-off score >14) (14, 15).
Statistical analysis
Before we started analysing data, we ran a power analysis with an independent sample t-test. Our sample of 79 participants is above the requirement of 70 for the minimum desired power of 0.9, moderate effect size of 0.5, and α of 0.05.
We analysed the obtained data using the jamovi^®^ version 2.6 computer software (open source). As the Kolmogorov-Smirnov test showed that data distribution was not normal (tested for each variable), we used the Mann-Whitney U test to compare two groups and the Kruskal-Wallis test to compare three or more groups. Quantitative data are presented as medians and ranges (interquartile where appropriate). The p-value of <0.05 was considered significant. To see how independent predictors like gender, partner status, having children, and having a history of psychiatric disorders affected DASS-21 and CIPS scores, we ran univariate logistic regression.
RESULTS
There were 65 women in the sample. The median age for both genders is 30, ranging from 26 to 50 years for women and from 27 to 43 years for men. Forty-nine respondents had worked for less than five years. Seventy-four claimed the study of medicine was their first choice and 72 picked family medicine as their first choice for specialisation. Forty-one had a partner, and 22 had at least one child. Six participants reported a history of psychiatric disorders (Table 1).
Table 2 shows the distribution of participants of both genders by the frequency and severity of experienced impostor feelings. Moderate to intense IP (CIPS>40) was reported by 59 participants (Cronbach’s alpha 0.95).
Mild to extremely severe symptoms of depression were reported by 17 participants, anxiety by 23, and stress by 20 participants (Cronbach’s alpha 0.91 for depression, 0.79 for anxiety, and 0. 87 for stress) (Table 3).
There were no significant differences in CIPS, depression, anxiety, or stress scores between men and women (p=0.059, p=0.905, p=0.228, and p=0.792, respectively). With the median CIPS score of 44 (IQR 43.1–50.4) participants with a partner also did not significantly differ from those without a partner (p=0.052). The same is true for participants who had children (p=0.053). History of psychiatric disorders also did not affect CIPS, depression, anxiety, or stress scores (p=0.556, p=0.200, p=0.962, p=0.340, respectively) (Table 4). The same is true for participants whose first choice was the study of medicine and specialisation in family medicine (p=0.724, p=0.724, p=0.246, and p=0.571, respectively).
Participants with higher CIPS scores also scored higher on all three subscales of DASS-21 (p<0.001) (Figure 1).
Plots showing higher mean (95 % CI) and median values of DASS-21 depression, anxiety, and stress scores in participants with CIPS scores higher than 40. * p<0.001 (Mann-Whitney U test). CI – confidence interval; CIPS – Clance Impostor Phenomenon Scale; DASS-21 – Depression Anxiety Stress Scale 21
DISCUSSION
This cross-sectional study in a sample of 79 first-year FMRs shows that most participants had some level of impostor feelings and that all participants with frequent or intense impostor feelings (more than one third) had significantly higher DASS-21 scores, which suggests that the impostor phenomenon increases the risk of stress, anxiety, and depression.
Our finding that more than one-third of participants had frequent or intense impostor feeling is consistent with the reported prevalence in medical students, residents, and physicians, ranging from 22.5 % to 46.6 % in different studies (16,17,18).
In contrast, DASS-21 scores in our sample are lower than the worldwide prevalence among resident physicians (19) but are still higher than in the general population (20). Some studies argue that the cause for poor psychological outcomes and impostor feelings is not working in a specific medical field but workplace-related risk factors like job demands, work-job imbalance, working overtime, administrative work, and, in the case of medical residents, inadequate training and the pressure that comes with studying and exams (8, 18). However, family medicine doctors in Croatia fit the bill: they often work overtime, they are burdened with administrative work, and receive a large number of patients in everyday practice. The reason for lower prevalence of depression, anxiety, and stress symptoms in our study sample could be that most of them had worked for less than five years in their profession. Also, they were surveyed at the beginning of their residency, when the workload and study/exam stress had not reached the peak.
The impostor syndrome had long been more common in women, but recent research confirms our findings, however limited, that this is no longer the fact (7, 18). The reason could be a shift in the gender paradigm, as more and more women work as physicians, breaking thus the stereotype of women as dominantly nurses (7). In fact, it is more common for a family doctor in Croatia to be a woman (21, 22), which is perhaps why our women FMRs do not feel like impostors based on their gender.
Other factors were not significantly associated with the CIPS scores, which is supported by various studies that found years of work, peer support, regular feedback, and good mentorship to have more impact on the result (11, 23).
The key finding of our research – the significant association between higher CIPS and DASS-21 scores – however, has confirmed our assumption that impostor feelings are associated with depression, anxiety, and stress. It also confirms earlier reports of IP being linked with increased burnout, anxiety, depression, suicide, and lower professional fulfilment (23, 24). More impostor feelings mean more psychological distress, as pointed out in a study among medical students (25) and among nursing students in Egypt (26). Another study on university students in the Netherlands suggests that higher levels of IP lead to mental exhaustion, anxiety, and fear of failure (27).
Considering that the impostor feeling is often heightened during medical schooling, addressing this issue should start at schools (28). Most studies show the impostor feelings can be alleviated with positive feedback and affirmation, safe environment to discuss medical errors, preparation for patient complaints, institutional support, and by avoiding delayed gratification (4, 7, 29). Changes should be made on institutional and personal levels to improve doctors’ mental health, with the emphasis on good family relationships and work-life balance as an essential part of medical school and residency curriculum.
Limitations of the study
The first limitation of this study is its cross-sectional design, which does not allow conclusions about causality. This is also the first study of this kind in FMRs in Croatia, and no comparison with earlier findings is possible. The third limitation is that both CIPS and DASS-21 rely on self-reported data and may be prone to response bias (withholding information on the history of psychiatric issues) or selection bias, considering that the response rate was 50 % (suggesting that only intrinsically motivated participants responded). Finally, the major limitation of our study is the possible sample bias owed to the small sample and the uneven distribution of participants by gender. It may have affected the findings of associations between specific parameters (such as gender, history of psychiatric issues, parenting, or having a partner) and the CIPS and DASS-21 scores. However, we find this sample representative of FMRs in Croatia, as generally 30–40 medical doctors enrol for this specialisation per year, and they are mostly women.
CONCLUSION
Despite the above limitations, our study has confirmed the association between impostor feelings and depression, anxiety, and stress in Croatian first-year FMRs. To our knowledge, this is the first study conducted among FMRs in Croatia to examine the association between the impostor phenomenon and mental health outcomes. Future research should aim to further investigate the prevalence, predictors, and consequences of the impostor phenomenon in this population, as well as its impact on residents’ well-being, clinical performance, and professional development. Strategies to alleviate IP among FMRs may include encouraging help-seeking, constructive feedback, recognising achievements, fostering peer support, promoting cognitive approaches such as reframing negative thoughts, practicing self-compassion, and implementing interventions such as small group discussions, workshops, and mentoring programmes. Follow up on the effectiveness of such strategies and interventions should also be part of future research to identify best practices in reducing impostor feelings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pascoe A Johnson D Putland M Willis K Smallwood N Differential impacts of the COVID-19 pandemic on mental health symptoms and working conditions for senior and junior doctors in Australian hospitals J Occup Environ Med 2022645 e 291910.1097/JOM.000000000000250535121691 · doi ↗ · pubmed ↗
- 2Gisselbaek M Hontoir S Pesonen AE Seidel L Geniets B Steen E Barreto Chang OL Saxena S Impostor syndrome in anaesthesiology primarily affects female and junior physicians Br J Anaesth 202413240910.1016/j.bja.2023.09.02537884406 · doi ↗ · pubmed ↗
- 3Villwock JA Sobin LB Koester LA Harris TM Impostor syndrome and burnout among American medical students: a pilot study Int J Med Educ 20167364910.5116/ijme.5801.eac 427802178 PMC 5116369 · doi ↗ · pubmed ↗
- 4Thomas M Bigatti S Perfectionism, impostor phenomenon, and mental health in medicine: a literature review Int J Med Educ 2020112011310.5116/ijme.5f 54.c 8f 832996466 PMC 7882132 · doi ↗ · pubmed ↗
- 5Clance PR Imes SA The impostor phenomenon in high achieving women: dynamics and therapeutic interventions Psychother Theory Res Pract 197815241710.1037/h 0086006 · doi ↗
- 6Thompson T Davis H Davidson J Attributional and affective responses of impostors to academic success and failure outcomes Pers Indiv Differ 1998253819610.1016/S 0191-8869(98)00065-8 · doi ↗
- 7Gottlieb M Chung A Battaglioli N Sebok-Syer SS Kalantari A Impostor syndrome among physicians and physicians in training: A scoping review Med Educ 2020541162410.1111/medu.1395631692028 · doi ↗ · pubmed ↗
- 8Harvey SB Epstein RM Glozier N Petrie K Strudwick J Gayed A Dean K Henderson M Mental illness and suicide among physicians Lancet 20213989203010.1016/S 0140-6736(21)01596-834481571 PMC 9618683 · doi ↗ · pubmed ↗