Myocardial Performance Improvement After Iron Replacement in Heart Failure Patients: The IRON-PATH II Echo-Substudy
Raúl Ramos-Polo, Maria del Mar Ras-Jiménez, María del Carmen Basalo Carbajales, Sílvia Jovells-Vaqué, José Manuel Garcia-Pinilla, Marta Cobo-Marcos, Javier de Juan-Bagudá, Cândida Fonseca, Josep Francesch Manzano, Andreea Eunice Cosa, Sergi Yun-Viladomat, Cristina Enjuanes

TL;DR
This study shows that heart failure patients with iron deficiency have worse heart function, but this improves after iron treatment.
Contribution
Demonstrates reversibility of myocardial dysfunction in heart failure patients after iron repletion using advanced echocardiographic parameters.
Findings
Iron-deficient heart failure patients had worse LV and RV myocardial performance compared to non-deficient patients.
Iron repletion improved LV and RV function, aligning with non-deficient patients.
Echocardiographic parameters like GLS, MW, and WE showed significant improvement after iron treatment.
Abstract
Background: Iron deficiency (ID) is a commonly seen comorbidity in heart failure (HF) patients. It is often associated with a poor prognosis and impaired physical capacity. The functional limitations linked to ID may lead to cardiac function abnormalities. The functional limitations linked to ID may lead to cardiac function abnormalities, that can be reversible after iron repletion. Some echocardiographic parameters, such as global longitudinal strain (GLS), myocardial work (MW) and its derivatives constructive work (CW), wasted work (WW) and work efficiency (WE), may be of added value in advanced cardiac performance assessment. Methods: IRON-PATH II was a multicenter, prospective and observational study designed to describe the pathophysiological pathways associated with ID. The echo-substudy included 100 HF patients that had undergone a specific pilot echocardiographic evaluation.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
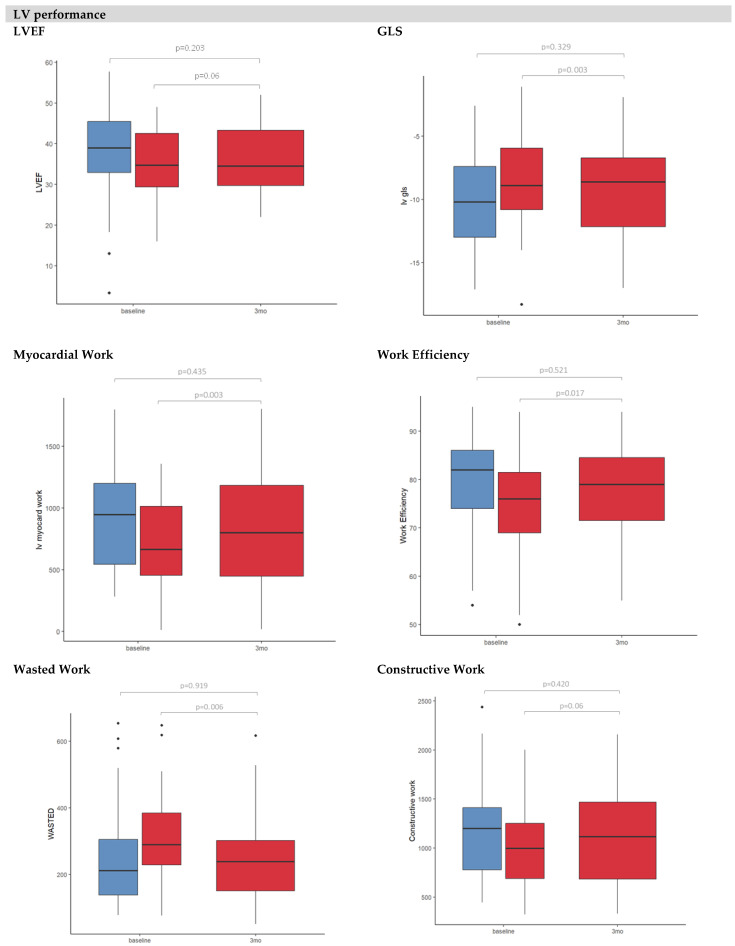 Figure 1
Figure 1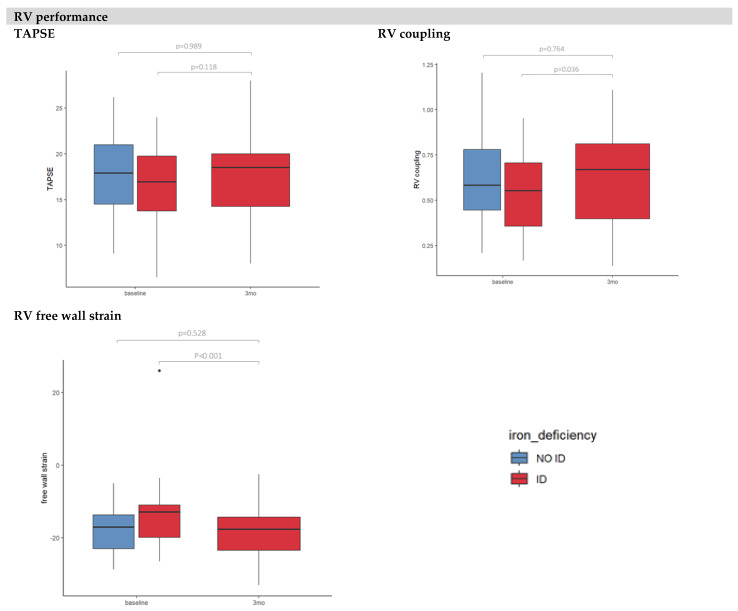 Figure 2
Figure 2- —CSL Vifor
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsErythropoietin and Anemia Treatment · Heart Failure Treatment and Management · Cardiac pacing and defibrillation studies
1. Introduction
Iron deficiency (ID) is highly prevalent among heart failure (HF) patients [1]. Regardless of the presence of anemia, ID reduces the energy efficiency of non-hematopoietic tissues with high energy demands [2]. Thus, ID affects the function of the cardiomyocytes by impairing the mitochondrial respiration chain, ATP production and contractility [3]. The decline in myocardial function due to ID has a pathophysiological basis, which has been explored in both human and animal models [4]. Therefore, anemia and ID directly affect cardiac function since they lead to a decrease in preload and the size of the left ventricular cavity [5].
Iron repletion in patients with HF and a left ventricular ejection fraction (LVEF) of less than 50% is associated with improvements in functional capacity and the quality of life and a reduction in rehospitalization [6,7,8,9,10]. However, the mechanisms by which iron replenishment improves exercise capacity and the quality of life remain unclear.
Although previous studies have shown that iron therapy may be linked to enhancements in cardiac function [5,11], the surrogate parameters of myocardial function used in these studies have several limitations. The first one, LVEF, is a volume-derived index that relies on geometric assumptions and is load-dependent [12]. Second, the conditions of elevated pre- or after-load directly affect GLS despite speckle-tracking-derived longitudinal strain offering lower inter-and intra-observer variability [13].
Regarding the limitations, the development of new echocardiography software has provided access to non-invasive assessments of highly valuable and more accurate information on cardiac physiology via the myocardial work (MW) index directly obtained by measuring the area of the pressure–strain loop. This is also the case for its derivatives constructive work (CW) and wasted work (WW) [14]. Finally, the non-invasive assessment of ventricular–arterial coupling (VAC) may be useful for a more complete cardiovascular performance profiling in this setting.
Interestingly, none of the previous studies that have attempted to assess the impact of iron status on cardiac function parameters have explored the impact of iron deficiency on myocardial performance parameters. This information is crucial to explaining the mechanisms that produce the worse exercise capacity observed in patients with ID [15]. Finally, the reversibility of the potential myocardial performance alterations associated with ID after iron replacement is undetermined.
Given the knowledge gap in this field and the limitations of previous studies, the IRON-PATH II echo-substudy was designed to define cardiac remodeling and myocardial deformation associated with systemic and tissue ID in patients with HF and reduced LVEF when compared to patients with HF without ID. Secondly, we aim to explore changes in myocardial function after iron replacement by using echocardiography.
2. Materials and Methods
Study design. IRON-PATH II (New pathophysiological pathways involved in iron metabolism disorder in hear failure: The IRON PATH II investigator-initiated Study, NCT05000853) was a multicenter, prospective, observational and investigator-initiated study aimed at characterizing the biological pathways involved in ID in HF patients and its association with laboratory biomarkers and clinical outcomes. The IRON-PATH II echo-substudy was designed to describe the echocardiographic features of HF patients according to ID and the effects of intravenous ferric carboxymaltose repletion on echocardiographic parameters.
The IRON PATH II study included a total of 210 HF patients (80 patients without ID and 130 patients with ID) recruited in 7 centers across Spain and Portugal between August 2021 and May 2023 and followed for a fixed period of 12 months. The echo-substudy included a subset of 100 patients on whom a specific echocardiographic evaluation was performed. All of them were recruited in the coordinating center.
The IRON-PATH II study was sponsored by CSL Vifor with coordination by Bellvitge Biomedical Research Institute (IDIBELL). The sponsor did not participate in the design of this study nor data analysis. An independent data and safety monitoring committee reviewed the data every 6 months. This study was approved by the local ethics committees for clinical research at each participating center and was conducted in accordance with the principles of the Declaration of Helsinki. All the patients gave written informed consent before entering this study.
The echo-substudy was included as a specific analysis within the IRON-PATH II project for the patients included at Bellvitge University Hospital. Safety was reported by local investigators in accordance with the current legislation that regulates pharmacovigilance in Spain and Portugal. Endpoint adjudication for the primary outcome components of this study was conducted on an ongoing basis by an independent endpoint committee blinded to the allocation of patient groups according to reports of serious events (death, readmission) by local investigators.
Patients. Patients with HF and an LVEF ≤50% according to the European Society of Cardiology (ESC) diagnostic criteria [16], receiving oral medication for chronic HF according to GDMT and without signs of fluid overload or low cardiac output were included. Reasons for ineligibility included significant anemia (Hb <11 g/dL), utilizing erythropoiesis stimulation agents or having used oral iron supplementation or intravenous iron treatment within the last 3 months. Individuals with a planned resynchronization therapy, coronary revascularization, heart transplant or left ventricular assistance device implantation or with less than one year of life expectancy were also excluded.
Study procedures. Patients were classified according to the current ESC guideline definition of ID (serum ferritin <100 ug/L or ferritin 100–299 ug/L with TSAT <20%) [16]. ID patents were treated following clinical recommendations; the dosage was calculated according to their weight and hemoglobin levels. Ferric carboxymaltose (FCM, Ferinject, CSL Vifor) was administered as an intravenous perfusion diluted in a sterile solution administered over 30–60 min. The patients received a maximum of 1000 mg of iron all at once. In patients for whom more iron was needed, a second dose was administered, at least fifteen days after the first one.
Study data. A detailed baseline evaluation was performed for all participants at study entry. Demographic characteristics, clinical and disease-related factors, comorbidities, laboratory tests and medical treatments were collected. Patients with ID were re-assessed after 3 months of iron replenishment (a clinical evaluation, a blood test and an echocardiography were performed). Clinical events were evaluated on an ongoing basis in all patients and finally ascertained after 12 months of follow-up.
Echocardiographic evaluation. Echocardiographic assessment was performed at baseline. In the ID group, echocardiography was repeated 3 months after intravenous iron replacement. Echocardiographic examinations were performed by two experienced research sonographers blinded to the iron status of the patient and the therapeutic interventions conducted in terms of iron repletion. Standard commercial Vivid E97 equipment and an MC5 active-matrix transducer (GE Medical Systems, Chicago, IL, USA) were used. All the images were digitally stored online and measured with specific offline software (EchoPAC Version 202, GE Medical Systems). All images were acquired throughout a complete cycle at a frame rate that represents 80% of the heart rate without exceeding 90 Hz or falling below 40 Hz. The data were transferred for further analysis in specific software. Measurements were made in three cycles (five cycles in patients that received atrial fibrillation during the examination), and the average value was calculated.
The echocardiographic features included the bidimensional and diastolic parameters (septal wall, posterior wall, LV end-diastolic diameter, LV end-diastolic volume, LA indexed volume, E/A ratio, E/e′ ratio), left and right ventricle function parameters (LVEF, GLS, LV indexed stroke volume, LV indexed stroke work, cardiac output, TAPSE, systolic pulmonary artery pressure, FAC, RV coupling ratio, RV free wall strain) and vascular function parameters (systemic arterial compliance, systemic arterial resistance index, LV end-systolic elastance (Ees), arterial elastance (Ea), ventricular–arterial coupling) (Table S1).
MW was assessed via the combination of LV strain data, the non-invasively estimated LV pressure curve (brachial cuff blood pressure) and the valvular event timing [14]. Strain and pressure data were synchronized using the onset of the R-wave in EKG, and the area of the pressure strain loop was used to derive the segmental and global MW. The global work index (GWI) was calculated as the average of segmental values. The CW was defined as work during segmental shortening in systole and during lengthening in isovolumic relaxation. WW (energy loss) is the work performed during lengthening in systole and shortening in isovolumic relaxation. Work efficacy (WE) was automatically calculated as the ratio of CW/(CW + WW).
Study outcomes. The main endpoint was the change in cardiac performance, including LVEF and LV deformation parameters (GLS and its derivates MW, WW, CW and WE) after iron replenishment. Secondary endpoints included the change in RV function parameters (TAPSE, FAC, RV free wall strain and RV coupling ratio). Finally, exploratory endpoints included cardiovascular function explored by means of Ea, Ees and VAC.
Statistical analysis. Variables are expressed as the mean and standard deviations (in the case of normal distribution) or median and interquartile ranges (in the case of non-normal distribution). Boxplots were used to graphically describe the distribution of the variables. A comparison was performed using the chi-squared test (for qualitative variables), the t-test (for quantitative variables with normal distribution) or the Mann–Whitney-U–Wilcoxon (for quantitative variables with non-normal distribution). The t-test was used for the variables that met the assumptions of independence, normality (using the Kolmogorov–Smirnov test) and homoscedasticity or equality of variances (using the Levene test).
The comparison between the baseline echocardiographic parameters (before iron replenishment) and those 3 months after iron replenishment was performed using a t-test for paired data. The 3-month variables of the iron-deficient group (after iron replenishment) were compared with the baseline variables of the non-iron-deficient group. Bar graphs were used to graphically describe the evolution of the variables. No multivariate statistical model was used.
All statistical tests and confidence intervals (CIs) were constructed with a Type I error, alpha level of 5%, with no adjustments for multiplicity. p-values below 0.05 were considered statistically significant. All analyses were performed using SPSS software (version 22.0; IBM, Armonk, NY, USA) and R software packages (version 4.2.1; R Foundation for Statistical Computing, Vienna, Austria).
3. Results
The IRON-PATH II echo-substudy included a subset of 100 patients undergoing a specific echocardiographic evaluation. Two patients were excluded due to a poor sonographic window. Thus, 98 patients were finally analyzed (Figure S1).
3.1. Baseline Characteristics
The baseline characteristics of the whole IRON-PATH II study cohort are presented in Table S2. The patients included in the echo-substudy cohort were slightly older (72 vs. 68 years, p = 0.027) and had worse renal function (eGFR 55 vs. 60 mL/min/1.73 m^2^, p = 0.044). Ferritin levels were lower in patients not included in the echo-substudy cohort (ferritin 244 vs. 138 ng/mL, p < 0.001) even though no differences in TSAT were observed (22 vs. 21%, p = 0.351).
The baseline characteristics of the echo-substudy sample, both overall and according to ID status, are listed in Table 1. ID was present in 44 patients (45%). Considering the clinical profile, ID patients were older (74 ± 8 vs. 70 ± 11 years; p-value = 0.03), more frequently male (78%), NYHA class II (71%) and had a slightly higher heart rate (72 vs. 67 bpm, p = 0.043). They also covered shorter distances in the 6 min walking distance (206 vs. 314 m, p < 0.001). Comorbidities appeared to be similar in the two groups, with the exception of atrial fibrillation (28 vs. 22%, p-value = 0.042).
The mean hemoglobin levels were lower among ID patients (13.2 vs. 14.2, p = 0.001), and the NTproBNP levels were higher (2180 vs. 997 pg/mL, p-value = 0.015). The ID group showed marked iron depletion evidenced by lower transferrin saturation (TSAT) (16 vs. 28%), ferritin (116 vs. 349 ng/mL) and iron (9 vs. 15 µmol/L) (all p-values < 0.001). Both groups were similarly treated (Table 1) with beta-blockers, angiotensin receptor neprilysin inhibitors (ARNIs), sodium–glucose cotransporter-2 (SGLT2i) and mineralocorticoid receptor antagonist (MRA) (94%, 76%, 71% and 76%, respectively), all p-values > 0.05. Anticoagulation therapy was more frequent among the ID patients (46% vs. 73%, p-value = 0.021).
3.2. Echocardiographic Features at Baseline
The groups according to ID status showed no differences relative to LV thickness, LV volumes, E/A ratio or E/e’ ratio (all p-values > 0.05) (Table 2). No differences were observed in the LVEF (38 ± 10% vs. 35 ± 9%, p-value = 0.210), TAPSE (18 mm vs. 17 mm, p-value = 0.118) or sPAP (29 mmHg vs. 30 mmHg, p-value = 0.150). The ID group displayed worse LV function expressed by lower GLS (−8.5 ± 9% vs. −10 ± 10%, p-value = 0.024), lower work efficiency (74 ± 10% vs. 80 ± 10%, p-value = 0.017), lower myocardial work (665 [453–1013] mmHg% vs. 947 [542–1199] mmHg%, p-value = 0.025) and higher wasted work (290 [228–384] mmHg% vs. 212 [138–305] mmHg%, p-value = 0.034) (Table 3 and Figure S2, panel A). The RV function was also worse, as shown by a lower RV free wall strain (−13 [−20–(−11)] % vs. −17 [−23–(−14)]%, p-value = 0.022) (Table 3 and Figure S2, panel B). However, no differences were observed regarding TAPSE (18 vs. 17 mm, p-value = 0.118) or sPAP (29 [24–35] vs. 30 [26–42] mmHg, p-value = 0.15). Finally, the ID group obtained worse end-diastolic elastance values (3.0 vs. 2.1 mmHg/mL, p-value = 0.03) and a worse ventricle–arterial coupling ratio (0.95 vs. 1.4 mmHg/mL, p-value = 0.04) (Table 3 and Figure S2, panel C).
3.3. Echocardiographic Features After Iron Repletion
After intravenous iron replacement (Table 3), improvements in GLS (−8.5 ± 9% vs. −9.3 ± 3%), work efficiency (74 ± 10% vs. 79 ± 10%), myocardial work (665 [453–1013] mmHg% vs. 801 [447–1183] mmHg%) and wasted work (290 [228–384] mmHg% vs. 239 [151–302] mmHg%) were observed (all p-values <0.05). Regarding the RV function, patients had an improved RV coupling ratio (0.54 ± 2 vs. 0.61 ± 0.3 mm/mmHg, p-value = 0.036) and RV free wall strain (−13 [−20 to −11]% vs. −18 [−24 to −14]%, p-value <0.001). Iron replacement had no impact on LV end-diastolic elastance or ventricle–arterial coupling (Ees/Ea). No differences were observed in any echocardiographic parameter of myocardial function between non-ID patients in comparison with ID-patients after iron replenishment (Figure 1 and Table 3).
4. Discussion
Our study provides relevant information regarding the pathophysiology of ID in the HF and LVEF <50% scenario. Firstly, patients with HF and ID displayed worse myocardial performance than non-ID patients, for both LV (GLS, myocardial work, wasted work and work efficiency) and RV (RV free wall strain and RV coupling), with no differences in LVEF or TAPSE. Secondly, iron repletion significantly improved myocardial performance in ID patients, resulting in a myocardial performance phenotype similar to that in non-ID patients.
There is accumulating evidence that ID is not only a consequence but also a contributor to the pathophysiology of systolic HF that potentially exacerbates disease progression through the mitochondrial dysfunction caused by intracellular iron depletion [17,18,19]. Previous studies showed that correcting anemia and ID results in an improvement in echocardiographic parameters, suggesting the role of these conditions in myocardial mechanics [5]. Toblli et al. demonstrated an enhancement in the LVEF (6.6 ± 3.8%) and a reduction in LV diameters (LVESD 10.5 ± 1.6 mm, LVEDD 9 ± 13 mm) with iron sucrose therapy among HF with reduced LVEF patients [20]. The IRON-CRT study [21] included 75 patients with HF, ID criteria and an LVEF of 45% or less. After CRT therapy, a greater increase in LVEF in response to CRT was observed in the group in which FCM was replaced when compared to placebo. The response was analyzed 3 months after iron replacement. The improvement was due to LV end-systolic volume (LVESV) reduction, with no differences in the LV end-diastolic volume (LVEDV).
Little evidence exists regarding the effects of iron repletion on strain parameters [11]. To our knowledge, only the Myocardial-IRON substudy [22] has explored the effects of iron repletion on myocardial function expressed through strain parameters. Improvement in the global longitudinal, circumferential and radial strain of both the LV and RV was observed 30 days after iron repletion. In COPD patients without anemia, ID was associated with a moderate increase in systolic pulmonary artery pressure [23]. However, no work to date has assessed the right ventricular remodeling associated with iron deficiency. Thus, in patients with HF, the impact of iron replacement on RV has not been adequately explored.
Myocardial work as a surrogate of cardiac function, back to the pressure–volume loop. Our cohorts showed no differences in the LVEF, LV stroke volume, LV stroke work, TAPSE or sPAP (all p-values >0.05). Nevertheless, in the IRON-PATH II echo-substudy, we employed speckle-tracking echocardiography (GLS, myocardial work index and its derivates) and VAC assessment as myocardial performance subrogates. These tools offer significant advantages over traditional measures like the LVEF as they offer a more accurate assessment of myocardial function by integrating both cardiac and arterial components [13,24,25]. The analysis of pressure–volume loops allows for the measurement of the energy imparted to the blood, with the area of the loop representing stroke work (SW) [26]. New echocardiography software creates arterial pressure–LV longitudinal myocardial strain curves by speckle-tracking [14]. This software calculates myocardial work, constructive work (work during segmental shortening in systole and during lengthening in isovolumic relaxation) and waste work (lengthening in systole and shortening in isovolumic relaxation).
Non-invasive methods for assessing myocardial work have shown good agreement with invasive pressure–volume loop measurements [27]. Thus, the myocardial work index allows for a comprehensive assessment of the energy dynamics within the heart while considering the loading conditions. In addition to the myocardial work index (work evaluated from mitral valve closure valve opening), waste work is calculated as the myocardial work consumed during segmental lengthening (negative work) that does not turn into segmental contraction (positive work) [14,27].
These parameters have been previously explored in the HF scenario. Sacubitril–Valsartan treatment has been shown to improve constructive work and work efficiency [28]; likewise, these two parameters have been proposed as a predictor of events in advanced HF [29] and as a predictor index of CRT response [30]. To the best of our knowledge, this is the first study demonstrating myocardial work improvement after iron repletion, due to a decrease in waste work and an improvement in work efficiency. The RV functional parameters like the RV coupling ratio and RV free wall strain also improved. Interestingly, these functional parameters were similar to those seen in the non-ID group after iron repletion.
Beyond myocardial performance, VAC makes it possible to study the relationship between the myocardium and the arterial tree. VAC is evaluated by non-invasively measuring the ratio of arterial (Ea) to ventricular end-systolic elastance (Ees) [31,32]. Ea is an integrative measure of arterial system properties [33], while Ees defines the ventricle’s contractile state and is relatively insensitive to loading conditions. Thus, VAC evaluation together with the interpretation of its components (Ea and Ees) allows for a more complete myocardial performance profile in patients with heart failure (HF) and iron deficiency (ID).
Ventricle–arterial uncoupling in HFrEF is characterized by a decrease in Ees together with an increase in Ea (derived from neurohormonal activation), which leads to higher VAC values [31]. Either CRT implantation [34] or pharmacological treatment with a β-blocker [35] may improve VAC. Patients with ID showed worse VAC at the expense of a lower Ees. However, no differences in Ees, Ea or VAC were observed after iron replacement.
The role of iron in myocardial performance. Myocardial activity is closely linked to oxidative metabolism [36]. Notably, not all the energy generated by oxidative metabolism is utilized and converted into effective work. Therefore, our data suggests that ID may contribute to HF progression based on the lower myocardial work (likely related to the higher waste work displayed by ID patients) and reversibility seen after iron replacement.
Clinically, the iron-deficient group was probably composed of patients with a true iron-deficient state, as reflected by a mean TSAT of 16%. The significant improvements observed in our study can be explained by the restoration of mitochondrial function and energy production in cardiomyocytes due to iron repletion [37]. Notably, ID repletion had a positive effect on cardiac performance even though AF was more frequent and the mean left atria was larger in patients in the ID group. Finally, the positive changes in RV function and ventricular–arterial coupling suggest that iron therapy may also improve pulmonary hemodynamics and right ventricular performance, thereby contributing to better overall heart function.
The ID group showed significantly higher NTproBNP levels (997 vs. 2180 ng/L, p = 0.015). The improvement in myocardial performance was not linked to a change in clinical congestion, since NTproBNP levels did not decrease in the control at 3 months (2180 vs. 2260 ng/L, p = 0.34). All patients included were in a clinically stable situation with no signs or symptoms of hypervolemia. The elevated NTproBNP values were probably related to subclinical congestion and worse iron absorption.
Our study highlights the significant improvements in myocardial performance following intravenous iron repletion in patients with HF and ID. These findings underscore the potential of iron therapy to enhance cardiac function beyond traditional measures such as the LVEF or TAPSE. Future research should include mechanistic studies to shed light on the pathways through which medical therapies, in general, and iron repletion, in particular, benefit myocardial function. These insights will pave the way for more targeted and effective therapeutic strategies.
Limitations. Our study has some limitations that should be mentioned. First, our study is based on echocardiography. Therefore, the performance of cMRI in the study of myocardial work after iron replacement is uncertain. However, echocardiography is an accessible technique, and myocardial work calculation is an easy-to-use and reproducible tool as it has been included in echocardiographic software. Second, speckle-tracking requires experience and depends on image quality. Non-invasive arterial pressure is included in the calculation of myocardial work, which can be variable throughout the cardiac cycle. Third, both groups were well balanced. However, ID patients were slightly older and had a higher incidence of AF and lower mean hemoglobin levels. Although this may partially explain the baseline differences, the improvement in myocardial performance after iron replacement was clear. The echocardiographic evaluation was performed 3 months after iron replenishment. However, the duration of the potential beneficial effect on myocardial performance is unknown. Finally, both groups underwent baseline echocardiography, but only the ID group received control echocardiography (3 months after replacement). Thus, direct comparison between the two groups is limited.
5. Conclusions
The IRON-PATH II echo-substudy demonstrates that HF patients with a reduced LVEF and ID have worse myocardial performance in both the LV and RV. Specifically, ID patients had impaired GLS, work efficiency, myocardial work, waste work, RV free wall strain and RV coupling. No differences were observed in terms of the LVEF or TAPSE. These alterations in myocardial function were measurable via echocardiography and were reversible with the intravenous repletion of ferric carboxymaltose. This underscores the significant role of iron therapy in enhancing cardiac function. Future research should explore the underlying mechanisms and further validate these findings to optimize therapeutic strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Melenovsky V. Petrak J. Mracek T. Benes J. Borlaug B.A. NuskováH. Pluhacek T. Spatenka J. Kovalcikova J. Drahota Z. Myocardial iron content and mitochondrial function in human heart failure: A direct tissue analysis Eur. J. Heart Fail.20171952253010.1002/ejhf.64027647766 · doi ↗ · pubmed ↗
- 2Rocha B.M.L. Cunha G.J.L. Falcão L.F. The Burden of Iron Deficiency in Heart Failure J. Am. Coll. Cardiol.20187178279310.1016/j.jacc.2017.12.02729447741 · doi ↗ · pubmed ↗
- 3Hoes M.F. Grote Beverborg N. Kijlstra J.D. Kuipers J. Swinkels D.W. Giepmans B.N.G. Rodenburg R.J. Van Veldhuisen D.J. De Boer R.A. Van Der Meer P. Iron deficiency impairs contractility of human cardiomyocytes through decreased mitochondrial function Eur. J. Heart Fail.20182091091910.1002/ejhf.115429484788 PMC 5993224 · doi ↗ · pubmed ↗
- 4Zhang H. Jamieson K.L. Grenier J. Nikhanj A. Tang Z. Wang F. Wang S. Seidman J.G. Seidman C.E. Thompson R. Myocardial Iron Deficiency and Mitochondrial Dysfunction in Advanced Heart Failure in Humans J. Am. Heart Assoc.202211 e 02285310.1161/JAHA.121.02285335656974 PMC 9238720 · doi ↗ · pubmed ↗
- 5Sutil-Vega M. Rizzo M. Martínez-Rubio A. Anemia and iron deficiency in heart failure: A review of echocardiographic features Echocardiography 20193658559410.1111/echo.1427130693550 · doi ↗ · pubmed ↗
- 6Graham F.J. Pellicori P. Kalra P.R. Ford I. Bruzzese D. Cleland J.G.F. Intravenous iron in patients with heart failure and iron deficiency: An updated meta-analysis Eur. J. Heart Fail.20232552853710.1002/ejhf.281036823953 PMC 10946839 · doi ↗ · pubmed ↗
- 7Anker S.D. Comin Colet J. Filippatos G. Willenheimer R. Dickstein K. Drexler H. Lüscher T.F. Bart B. Banasiak W. Niegowska J. Ferric Carboxymaltose in Patients with Heart Failure and Iron Deficiency N. Engl. J. Med.20093612436244810.1056/NEJ Moa 090835519920054 · doi ↗ · pubmed ↗
- 8Ponikowski P. Kirwan B.-A. Anker S.D. Mc Donagh T. Dorobantu M. Drozdz J. Fabien V. Filippatos G. Göhring U.M. Keren A. Ferric carboxymaltose for iron deficiency at discharge after acute heart failure: A multicentre, double-blind, randomised, controlled trial Lancet 20203961895190410.1016/S 0140-6736(20)32339-433197395 · doi ↗ · pubmed ↗