Comparison of the Outcomes of Double-Bar and Non-Double-Bar Techniques in the Minimally Invasive Repair of Pectus Excavatum: A Focus on Bar Removal and Complications
Duk Hwan Moon, Doyun Heo, Sungsoo Lee

TL;DR
This study compares two minimally invasive techniques for correcting pectus excavatum, finding that the double-bar method leads to shorter hospital stays and fewer complications.
Contribution
The study introduces a comparative analysis of double-bar versus non-double-bar MIRPE techniques, highlighting differences in bar removal time and complications.
Findings
The double-bar group had shorter hospital stays and reduced bar removal operation times.
The double-bar technique was associated with fewer chest X-ray bony spurs.
Non-double-bar use and bony spurs were significant risk factors for prolonged bar removal.
Abstract
Background/Objectives: Minimally invasive repair of pectus excavatum (MIRPE) techniques are classified into non-double-bar methods, which elevate the chest wall only, and double-bar methods, which involve both elevation and compression. Our objective was to compare the clinical outcomes of MIRPE procedures between the double-bar and non-double-bar techniques, with a particular focus on bar removal operation time and its associated complications. Methods: This retrospective study included 103 patients who were diagnosed with pectus excavatum and underwent MIRPE between January 2015 and July 2022. Propensity score matching was performed to adjust for confounding variables between patients who underwent the double-bar procedure and those who underwent the non-double-bar procedure. Comparative analyses between the groups were conducted using t-tests and chi-square tests, and linear…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
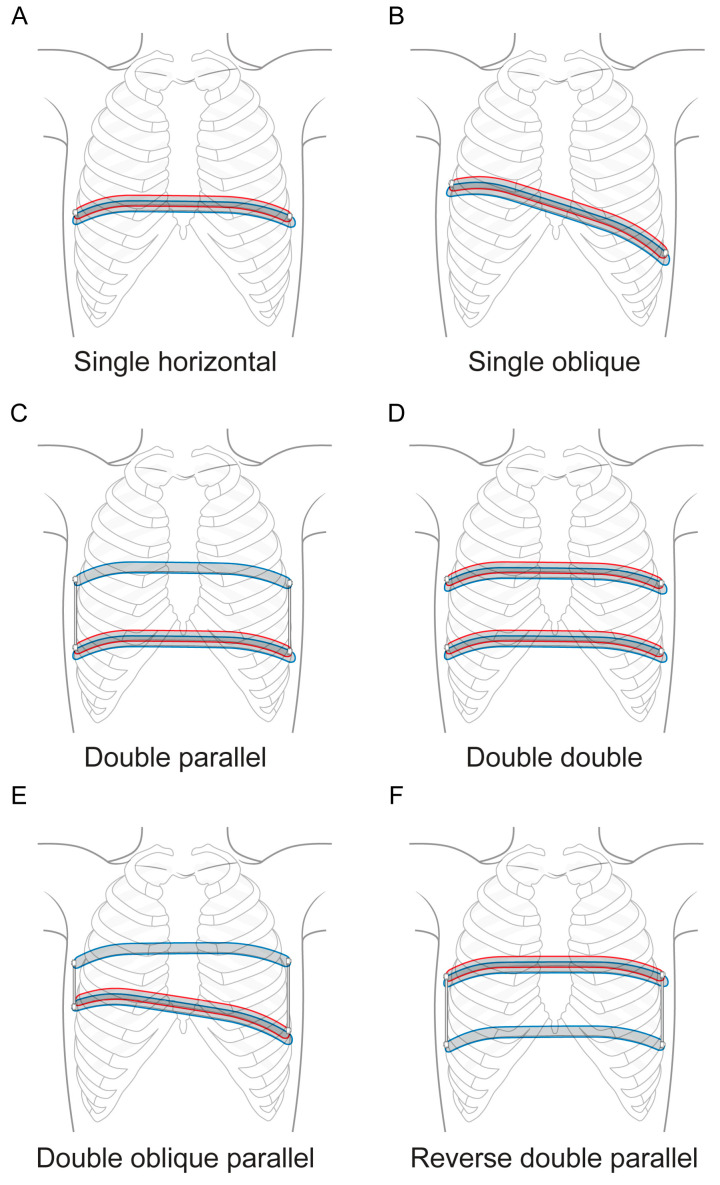 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPectus Deformity Diagnosis and Treatment
1. Introduction
Pectus excavatum (PE) is a congenital deformity of the chest wall characterized by posterior displacement of the sternum and costal cartilages [1]. Patients with PE often grapple with psychological issues, such as low self-esteem and body image dissatisfaction [2]. Additionally, these patients may experience dyspnea during exertion, non-specific chest pain, and reduced exercise tolerance, with the possibility of experiencing pulmonary complications [3,4].
Since the advent of conventional minimally invasive repair of pectus excavatum (MIRPE), surgical methods for treating PE have advanced significantly [5]. These advancements have led to an increased surgical correction rate; a reduction in complications, including pectus bar dislocation; and improved patient prognoses [6,7]. Initially, methods involving the use of two or more bars, such as the cross-bar and parallel bar techniques, were introduced to enhance the stability and efficiency of the pectus bar [8]. However, in non-double-bar techniques, sternal elevation alone is often insufficient to achieve complete correction of asymmetric PE due to the limited distribution of corrective force [9]. Moreover, excessive mechanical stress at hinge points can lead to the formation of bony spurs around the bar, making bar removal technically difficult [10].
Recent suggestions indicate that the double-bar technique, which involves the insertion of two bars—one into the retrosternal region and one into the presternal region, with the aim of simultaneously elevating and compressing the chest wall—may significantly reduce operation times, the postoperative hospital admission period, and complication rates for PE patients [11]. The double-bar technique is continually being refined and improved, while other methods, such as the oblique double-bar technique, are being developed [9].
Despite these advancements, there is limited evidence directly comparing the clinical outcomes of the double-bar (DB) and non-double-bar (NDB) techniques, particularly in terms of the operation time for bar removal and associated complications. This study aims to compare the clinical outcomes between DB and NDB patients, with a specific focus on bar removal operation time, complications, and the incidence of chest X-ray bony spurs. By evaluating these facets, our goal is to provide insights into which technique offers superior outcomes, leading to better patient management and surgical decision-making in PE treatment.
2. Materials and Methods
2.1. Patients
Among patients with past medical records from the thoracic surgery department of a tertiary university hospital, 103 patients who were diagnosed with PE and had undergone an MIRPE operation between January 2015 and July 2022 were retrospectively selected. In this study, chest X-ray (CXR) bony spurs are defined as the presence of small, bilateral, extra pieces of bone that have grown on the surface of the rib bones, as observed on chest X-ray following bar removal operation. This study received approval from the local institutional review board of Gangnam severance Hospital in Korea (IRB No. 3-2025-0034), and the requirement for informed consent was waived due to its retrospective nature.
2.2. Operative Techniques
For patients in the DB group, the double-bar correction technique was employed to stabilize the chest wall. First, a primary bar was inserted below the chest wall along a path created by a passer, which was guided through chest tubes and then rotated into position [9]. Next, a second bar was placed subcutaneously and submuscularly above the chest wall using a second passer [9]. Once both bars were properly aligned, they were fixed together with two screws, ensuring stability during the postoperative period [9]. The configuration of the DB varied based on the patient’s chest shape, ranging from a single horizontal placement to a single oblique one, with some cases involving double-bar insertion at the lower part and a parallel single bar connection at the upper part or even double-bar insertion at both the upper and lower parts to create a parallel structure (Figure 1).
For patients in the NDB group, two bar correction techniques were employed: the cross type and the parallel type. In the case of the cross type, the crossing point of the two bars elevated both the deepest portion of the lesion and the entire chest wall [8]. In contrast, the parallel type involved placing the first bar transversely at the deepest point of the chest and the second bar transversely 1 to 2 intercostal spaces above the first [8]. In both techniques, the ends of the bar were secured using bridge plates [8].
2.3. Statistical Analysis
Descriptive statistics were used to summarize the following variables: age, gender, height, weight, body mass index (BMI), Haller index (HI), bar insertion operation variables, and bar removal operation variables. Independent sample t-tests were used to assess the differences between groups, and chi-square tests were used for categorical variables. Univariate and multivariate regression analyses were used to identify risk factors leading to prolonged removal operation time.
To adjust for confounding factors, propensity score matching was employed. Six confounding variables (age, gender, height, weight, BMI, and Haller index) were used to estimate the propensity score, which is the predicted probability of undergoing DB insertion. A logistic regression model was fitted to these six variables to predict the probability of undergoing DB insertion versus NDB insertion. Patients were then matched using the nearest-neighbor matching algorithm with a caliper of 0.2 standard deviations of the logit of the propensity scores. Each DB patient was matched 1:1 with an NDB patient with a similar propensity score.
All statistical analyses were performed using R software (version 4.4.0; R Foundation for Statistical Computing, Vienna, Austria).
3. Results
3.1. Before Propensity Score Matching
A total of 103 PE patients were divided into two groups: a double-bar (DB) group (n = 59) and a non-double-bar (NDB) group (n = 44). In terms of baseline characteristics, the DB group had significantly lower mean values for age, weight, height, and BMI (p < 0.001) compared to the NDB group. Additionally, the Haller index (HI) was significantly lower in the DB group than in the NDB group (p = 0.045). Among the variables related to bar insertion, hospital stay duration was significantly shorter (p < 0.001), and the complication rate was lower (p = 0.012), in the DB group compared to the NDB group. Bar removal operation time (p < 0.001) and the incidence of CXR bony spurs upon bar removal (p < 0.001) were both significantly lower in the DB group than in the NDB group (Table 1).
3.2. After Propensity Score Matching
A total of 48 PE patients were selected, with each group consisting of 24 patients after propensity score matching. There were no significant differences between the two groups in terms of age, gender, height, weight, BMI, HI, bar insertion operation time, complication rate, or bar removal hospital stay. However, the DB group had significantly shorter bar insertion hospital stay (p < 0.001) and bar removal operation time (p < 0.001) and a lower incidence of CXR bony spurs upon bar removal (p = 0.018) compared to the NDB group, even after propensity score matching (Table 2).
3.3. Risk Factors for Prolonged Bar Removal Time
Univariate and multivariate linear regression analyses were conducted to identify the potential risk factors associated with prolonged bar removal time. Univariate analysis revealed significant associations for several factors. NDB was significantly associated with a prolonged bar removal time (p < 0.001). Additionally, height (p = 0.035), weight (p = 0.041), and the presence of a CXR bony spur (p < 0.001) were identified as significant factors for prolonged bar removal time. A multivariate linear regression model indicated that NDB was a significant predictor of prolonged bar removal time (p < 0.001). The presence of a CXR bony spur also remained significantly associated with prolonged bar removal time (p < 0.001). Height and weight were not significant in the multivariate analysis. (Table 3)
4. Discussion
This study compared the clinical outcomes of MIRPE procedures between DB and NDB among PE patients. After propensity matching for baseline characteristics, the DB group exhibited shorter bar insertion hospital stays (in days), shorter bar removal operation times, and fewer incidences of CXR bony spurs compared to the NDB group. Multivariate analysis identified NDB use and the presence of CXR bony spurs as significant risk factors for prolonged bar removal operation time.
The fewer days spent in the hospital after bar insertion in DB the group could be attributed to more stable chest wall support through better force distribution, potentially reducing postoperative complications such as pain or displacement. Although MIRPE is widely recognized as an effective procedure, bar removal carries a risk of postoperative complications, including wound infection, pneumothorax, pleural effusion, cardiac perforation, and, in rare cases, even death [12]. While uncommon, these complications can prolong recovery, diminish patient satisfaction, and negatively impact overall quality of life [13]. The likelihood of such adverse events increases when technical challenges arise during removal, often occurring due to anatomical alterations, such as bony spurs forming around the implanted bar.
Bony spurs on a CXR appear as radiopaque structures, formed through granulation tissue development and subsequent osteocalcification, a process driven by inflammatory responses. The higher incidence of CXR bony spurs in the NDB group suggests that the NDB technique may exert unevenly distributed pressure on the chest wall, causing localized shear stress on the lateral stabilizers (hinge points), leading to bony spur formation. In contrast, the DB technique ensures better force distribution across the chest wall, as shown in our graphical abstract, thereby reducing the incidence of CXR bony spurs. Specifically, in addition to the two hinge points, the force acting on the chest wall (chest wall restoring force) is dispersed over multiple other points.
These bony spurs make bar removal surgeries more technically challenging. Surgeons often need to use orthopedic instruments, such as an osteotome or rongeur, to forcibly remove the bar, which increases operation time and the risk of wound complications that could result in greater postoperative pain [14]. Our findings are consistent with this observation, as the presence of CXR bony spurs was identified as a significant risk factor for prolonged removal operation time. In this study, postoperative complications following bar removal were observed in two patients, with both complications likely related to the excessive use of these orthopedic instruments during surgery causing tissue damage. To address these issues, we propose the DB technique as a strategy for possibly reducing the incidence of CXR bony spurs, shortening bar removal operation time, and consequently minimizing wound complications as well as perioperative pain and complications. Given that the primary patient population for this procedure consists of growing adolescents, minimizing surgical complications is critical [15]. In addition to improving patient outcomes, the DB procedure can also reduce the technical burden on surgeons during bar removal.
This study has a few limitations. First, as a retrospective study, there was potential for selection bias between the DB and NDB groups. To mitigate this, we conducted propensity score matching and performed analyses on the matched patients. Second, the final sample size was relatively small (n = 48), which may limit the generalizability of our findings. Third, while the DB technique appears to provide clinical benefits during both PE repair and bar removal, its long-term efficacy in maintaining chest wall correction post-removal remains uncertain. Lastly, bar maintenance time was consistent across patients, and it was not found to significantly influence the clinical outcomes of this study. Therefore, further prospective studies with larger sample sizes and long-term follow-ups are needed to validate these findings and further explore the clinical advantages of the DB technique.
While the MIRPE procedure offers significant advantages, including shorter recovery times and fewer complications, it may not be suitable for all patients. In particular, for patients with upper chest wall deformities, such as pectus arcuatum with complex deformity, open repair (a modified Ravitch operation) may provide a more effective correction [16]. However, for most younger patients with pliable chest walls, MIRPE remains a highly effective and minimally invasive option [17].
Given these considerations, our study provides valuable insights into the pros and cons of the DB and NDB techniques in MIRPE procedures gained through comparing their outcomes. By directly comparing both groups, we found that the DB technique offers significant advantages, including shorter bar removal operation times and fewer complications, making it the preferable option.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Croitoru D. Nuss D. Chest wall anomalies: Pectus excavatum and pectus carinatum Adolesc. Med.20041545547110.1016/j.admecli.2004.06.00215625987 · doi ↗ · pubmed ↗
- 2Steinmann C. Krille S. Mueller A. Weber P. Reingruber B. Martin A. Pectus excavatum and pectus carinatum patients suffer from lower quality of life and impaired body image: A control group comparison of psychological characteristics prior to surgical correction Eur. J. Cardiothorac. Surg.2011401138114510.1016/j.ejcts.2011.02.01921440452 · doi ↗ · pubmed ↗
- 3Hebra A. Calder B.W. Lesher A. Minimally invasive repair of pectus excavatum J. Vis. Surg.201627310.21037/jovs.2016.03.2129078501 PMC 5637818 · doi ↗ · pubmed ↗
- 4Kelly R.E.Jr. Obermeyer R.J. Nuss D. Diminished pulmonary function in pectus excavatum: From denying the problem to finding the mechanism Ann. Cardiothorac. Surg.2016546647510.21037/acs.2016.09.0927747180 PMC 5056935 · doi ↗ · pubmed ↗
- 5Park H.J. Rim G. Yoon S.K. Recent Advancements in Pectus Surgery: Crane Lifting, Multiple-Bar Approach, Bridge Stabilization, and Sandwich Technique J. Pediatr. Surg.20245964064710.1016/j.jpedsurg.2023.12.01238185539 · doi ↗ · pubmed ↗
- 6Park H.J. Rim G. Development of a Screw-Crane System for Pre-Lifting the Sternal Depression in Pectus Excavatum Repair: A Test of Mechanical Properties for the Feasibility of a New Concept J. Chest Surg.20215418619010.5090/jcs.21.00833975982 PMC 8181698 · doi ↗ · pubmed ↗
- 7Kim H. Rim G. Park H.J. Technical Advances in Pectus Bar Stabilization in Chest Wall Deformity Surgery: 10-Year Trends and an Appraisal with 1500 Patients J. Chest Surg.20235622923710.5090/jcs.22.13637096252 PMC 10345656 · doi ↗ · pubmed ↗
- 8Moon D.H. Park C.H. Moon M.H. Park H.J. Lee S. The effectiveness of double-bar correction for pectus excavatum: A comparison between the parallel bar and cross-bar techniques P Lo S ONE 202015 e 023853910.1371/journal.pone.023853932941460 PMC 7498055 · doi ↗ · pubmed ↗