Going beyond the fifth child: Exploring the determinants of desire for more children among high parity partnered women in Uganda
Godfrey Tumwizere, Yiga Joseph Douglas, Allen Kabagenyi, Betty Kwagala

TL;DR
This study explores why some women in Uganda who already have five or more children still want more, identifying factors like religion, education, and decision-making autonomy.
Contribution
The study is the first to focus on the desire for more children among high-parity women in Uganda, revealing novel insights into socio-religious and educational determinants.
Findings
21% of high-parity women in Uganda desire more children.
Catholic women and those without decision-making autonomy are more likely to desire more children.
Education and contraceptive use significantly reduce the desire for more children.
Abstract
Despite the extensive research on fertility desire among women worldwide, there is a dearth of literature on the desire for more children among high-parity women. This study aimed to identify the determinants of the desire for more children among high parity partnered women in Uganda. This study was based on nationally representative data from the 2016 Uganda Demographic and Health Survey. The study sample comprised of a weighted sample of 4502 women aged 15–49 years with five and more children. A complimentary log-log model was fit to identify factors associated with the desire for more children among high-parity women in Uganda at the 5% level of significance. The findings revealed that 21% of high parity partnered women desired more children. The odds of desire for more children were 26% higher among women without decision-making autonomy on the number of children (AOR = 1.262 95%…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
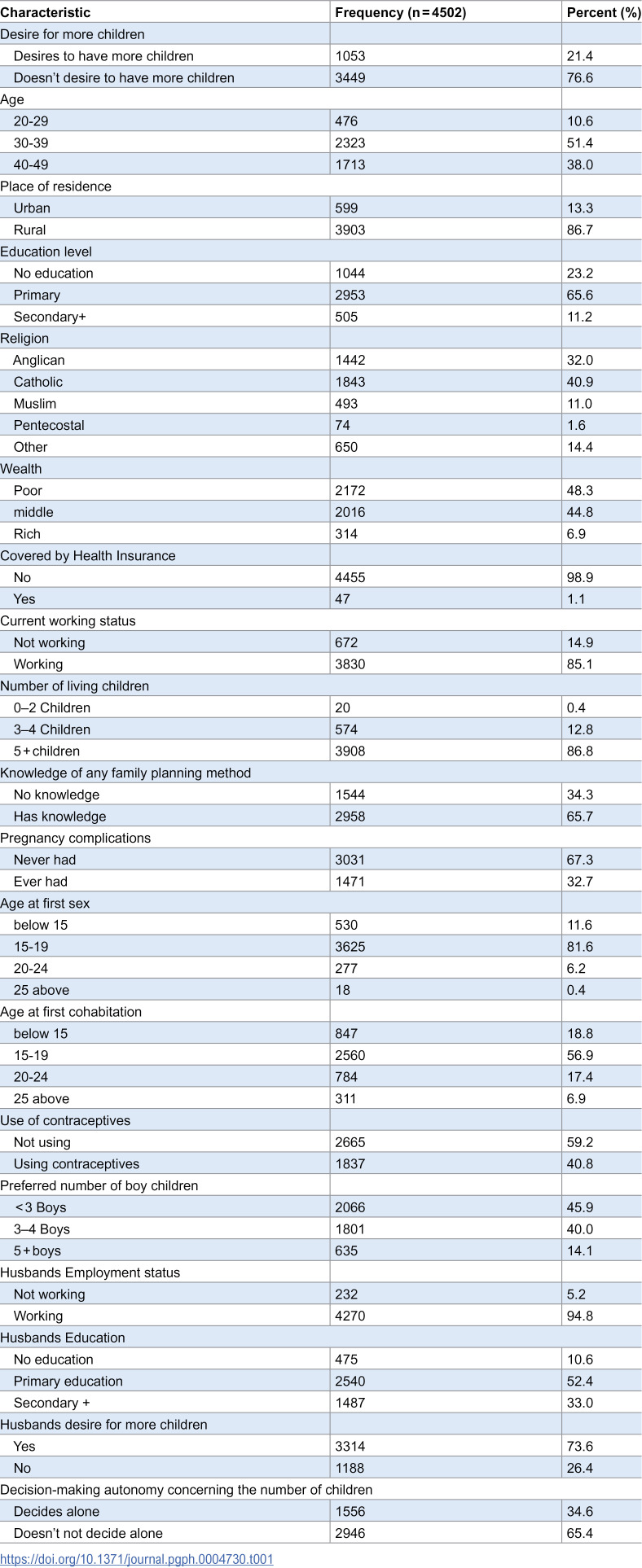 Figure 1
Figure 1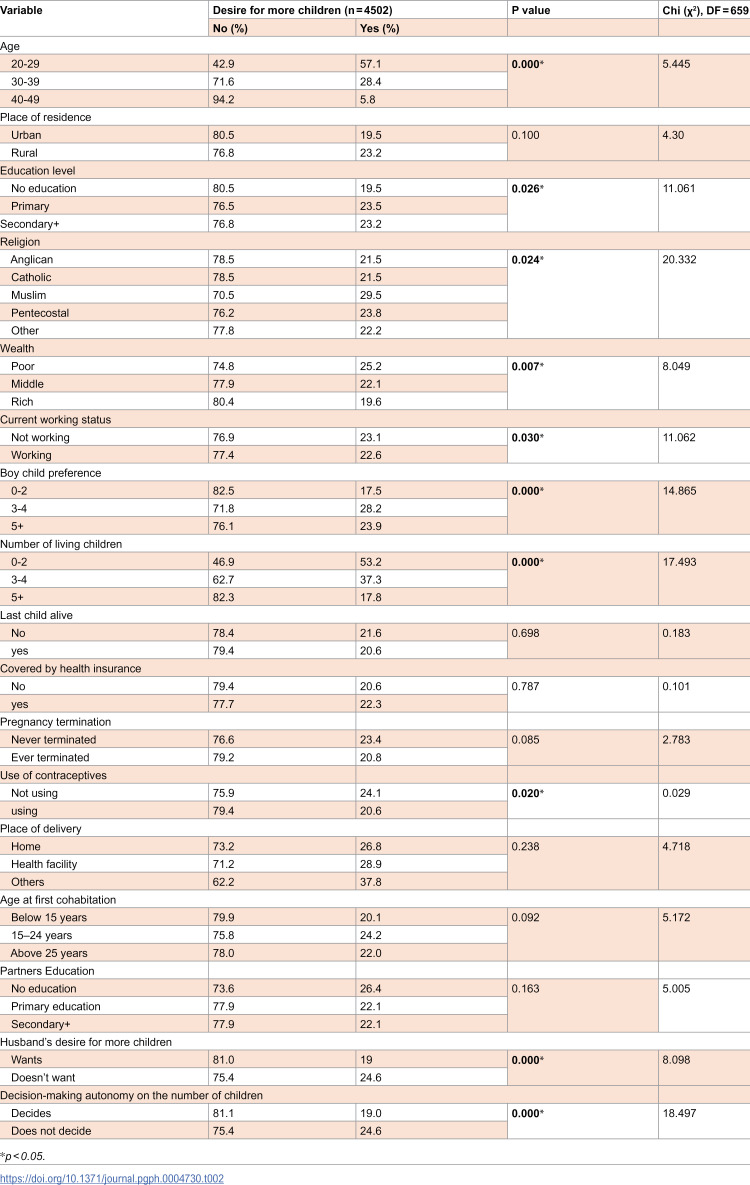 Figure 2
Figure 2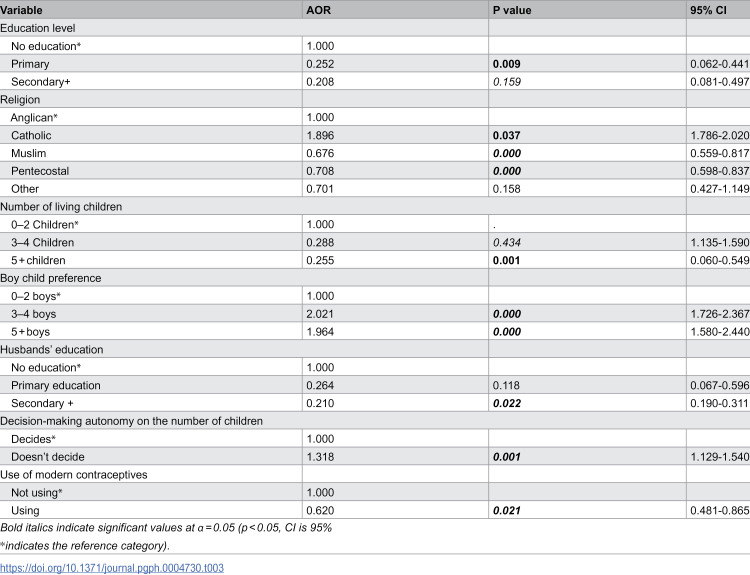 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Maternal and Child Health · Demographic Trends and Gender Preferences · Family Dynamics and Relationships
Introduction
The global population of over eight billion people is projected to reach nearly 9.6 billion by 2050 [1]. Africa’s population is expected to grow from 1.5 billion in 2024 to 2.4 billion in 2050, accounting for over 60% of the projected global population growth during this period [1,2]. While fertility rates have declined in many regions, some low- and middle-income countries still experience high levels of fertility [3]. Among the 78 million people added to the world population annually, approximately 97% originate from low- and middle-income countries [4]. Scientists predict that the continuous population growth will reach a level where there will not be enough resources to sustain life, and this raises concerns about whether the earth is facing overpopulation [5].
Sub-Saharan Africa with the lowest world economies have youngest population with 40% of the population younger than 15 years [6]. Studies reveal that in sub-Saharan Africa, women still produce more than four children [4,7], but more importantly, many women with as many as five children still want to produce more [4]. Uganda has the second youngest population in the world, with more than three-quarters (78%) aged below 35 years. Demographers project this youthful population to double in the next 25 years [8]. Despite the decline in Uganda’s fertility from 6.9 children to 5.2 children per woman [9] the current fertility level raises concerns about the potential impact on the country’s ability to achieve the desired fertility [10,11]. A significant proportion of high-parity women with five or more children who apparently should have attained the desired fertility, continue to express a desire for more children or are undecided whether to have more [4]. This not only defies conventional expectations but also perpetuates high fertility rates, exacerbates dependency ratio that strain already limited resources potentially hindering the realization of demographic dividend which is a critical component of sustainable development [12,13].
Research on fertility desires among high-parity women show several factors influencing their fertility preferences. A study by Atake and Gnakou Ali [7] in four high-fertility countries in sub-Saharan African countries found that women’s empowerment in economic and familial domains, is associated with a desire for fewer children. Elements such as education, decision-making power, and control over household resources are significant in shaping fertility preferences [7]. Similarly, Ahinkorah, Seidu [4] analyzed data from 32 Sub-Saharan African countries and identified that age, educational attainment, contraceptive use, and the number of living children significantly influence women’s desire for more children. Women with higher education levels and those using contraceptives were less likely to desire additional children [4]. In Ghana, research by Owoo [14] highlighted that internalized patriarchal norms and perceptions of male partner pronatalism are linked to women’s intentions to have more children, which emphasizes the role of socio-cultural factors in fertility decisions [14]. Furthermore, a synthesis of longitudinal studies across 28 countries in Africa and Asia demonstrated that while women’s desire to stop childbearing is a strong predictor of subsequent fertility, discrepancies often exist between fertility preferences and actual behavior [15].
In Uganda, a number of studies [16–21] have explored the factors affecting the desire for more children in different settings. Some studies have been conducted among HIV-positive individuals and HIV-discordant couples [20,22], whereas other studies have explored fertility desire from a general population perspective, including among married or cohabiting individuals [11]. These studies indicate that the desire for few children is still low [17,18,20]. The limited information on desire and intention to have more children among women with five or more children, leaves a noticeable gap in the literature that calls for an in-depth examination. This study aimed to determine factors associated with the desire for more children among high parity partnered women. The study attempted to answer the following research question; What are the determinants of the desire for more children among women with 5 + children? We hypothesized that age, level of education and decision-making autonomy on the number of children do not significantly affect the desire for more children among high parity partnered women in Uganda.
Methods
Data source
The study used secondary data from Uganda Demographic and Health Survey (UDHS). Data were accessed with permission from Measure DHS. UDHS is a cross-sectional survey that uses a stratified two-stage cluster sampling design. The 2016 UDHS interviewed 18506 women aged 15–49. We selected 4502 partnered women who reported five and more children during the survey.
Measure of the outcome variable
The outcome variable “desire for more children” was derived from the question, “Would you like to have a (another) child, or would you prefer not to have any more children?”. The question had five response options: “want another child,” “want no more,” “cannot become pregnant,” “undecided,” and “don’t know”. Women who responded that they wanted another child were considered to have a desire for more children, whereas others were considered not to have a desire for more children. Thus, the variable was recorded on a binary scale of 0 = does not desire more children and 1 = desires to have more children. Women who provided any other response (“cannot get pregnant,” “undecided,” or “don’t know”) were excluded because their responses were unclear about their fertility preference.
Measure of explanatory variables
The explanatory variables for this study included age, education, place of residence, wealth status, employment status, religion, knowledge of family planning, number of living children, mortality experiences, age at first sex, preference of boy child, use of contraceptives, history of pregnancy termination, ideal number of children, place of delivery, age at first cohabitation, partner employment status, partner education, husband desire for children and decision-making autonomy. There were only 8 women aged 15–24 with at least 5 children and were regrouped by 20–29 years. The selection of these explanatory variables was based on previous studies and their hypothetical relationship with the desire to have more children.
Statistical analysis
Statistical analysis was performed using STATA (Version 17) [23]. Data were weighted to ensure representativeness of the study population. The analyses were performed at three levels. At univariate analysis, the frequency and percent distribution of women according to the sociodemographic characteristics were determined. At the bivariate level, a cross tabulation of desire for more children and each explanatory variable was performed. The Pearson chi square test was used to measure the significance of associations of desire for more children with each explanatory variable at 5% level of significance. All variables with a ρ value less than or equal to 0.05 and with no autocorrelation (Vif < 10) were automatically considered for further analysis at the multivariate level. Age, wealth index and husband’s desire for more children showed autocorrelation with Variance inflation factor greater than 10 and were not considered for further analysis. At the multivariate level, since desire for more children was measured on a binary scale (1 = desires and 0 = does not desire), a complementary log-log regression model was used. Model building was done using stepwise selection to fit the factors associated with the desire for more children and results presented in the form of adjusted odds ratios (AORs) with 95% confidence intervals.
Results
Characteristics of high parity partnered women in Uganda
Table 1 presents the distribution of women’s sociodemographic characteristics. The results indicate that 21% of high-parity women desire to have more children. More than half (51%) of the high-parity women who desired more children were aged 30–39 years, the majority (87%) resided in rural areas, more than half (66%) had attained a primary level of education, 41% were affiliated with the Catholic religion, 85% were currently working, more than half (67%) had never experienced pregnancy complications, and 54% preferred at least 3 boys. In addition, more than half (66%) of the women were aware of a family planning method, and 93% had a history of child mortality. With respect to wealth, the findings show that almost half (48%) of the high-parity women were from poor wealth category households, 45% were from the middle quintile, and 7% were from the rich category. The results also indicate that the majority (85%) of the high-parity women were working and 87% had at least 5 living children. The results also revealed that 59% had never used contraceptives, more than half (57%) had their first cohabitation between 15 and 19 years, whereas approximately one quarter (19%) had their first cohabitation at before 15 years. Concerning age at first sex, more than half (82%) had their first sex between 15 and 19 years, and 12% had their first sex below 15 years. Seventy per cent of the women had no history of pregnancy termination. In terms of partner characteristics, 95% of women reported that their partners were working, 52% of women had partners with primary education, approximately 3 in 4 women (74%) had partners who desired more children, and 65% of women did not decide on matters regarding the number of children.
Table 1: Distribution of high parity partnered women by selected characteristics, UDHS 2016.
Bivariate analysis of the factors associated with the desire for more children
The findings in Table 2 reveal that the desire to have another child decreased with increasing age, and the association between the woman’s age and the desire for more children was significant (P = 0.000). More than half (approximately 57%) of the women who desired more children were aged 20–29 years, with 26% aged 30–39 years and 6% aged 40–49 years. The woman’s working status (ρ = 0.030) was significantly associated with the desire for more children. The desire for more children increased with increasing education levels. More than 1 in 5 women (23%) with secondary education and above had a desire for more children, with 19% of women without education having a desire for more children. The preferences of the boy child (ρ = 0.000), religion (ρ = 0.024), number of living children (ρ = 0.000), partner desire (ρ = 0.000) and decision-making autonomy (ρ = 0.000) were statistically significantly associated with the desire for more children.
Table 2: Desire for more children by selected characteristics.
Factors associated with the desire for more children among high parity partnered women
Table 3 shows the results of the multivariate complementary log-log of desire for more children. The desire for more children among high-parity women was associated with education level, religion, number of living children, preference for boy children, partner education, decision-making autonomy and use of contraceptives.
Table 3: Complementary log–log regression of factors associated with the desire for more children.
The likelihood of the desire for more children decreased with increasing education level. Women with primary education had 75% lower odds of desire for more children (AOR = 0.252, 95% CI = 0.062-0.441, whereas women with at least secondary education had 79% lower odds of desire for more children (AOR = 0.208, 95% CI = 0.081-0.497) than women with no education. Similarly, women whose partners had at least secondary education had 79% reduced odds of desire for more children (AOR = 0.210, 95% CI = 0.190-0.311) compared than women whose partners have no education. Compared with Anglican women, Catholic women had 89% increased odds of desire for more children (AOR = 1.896, 95% CI = 1.786 - 2.020), whereas Muslim women had 33% reduced odds (AOR = 0.676, 95% CI = 0.559-0.817) of desire for more children. In the same vein, the women who said that they were Pentecostals had 29% reduced odds (AOR = 0.708, 95% CI = 0.598-0.837) relative to their Anglican counterparts. Women with at least five living children had 75% reduced odds of desire for more children compared to those with less than three living children (AOR = 0.255, 95% CI = 0.060-0.549). Additionally, women who used contraceptives were 0.6 times less likely (AOR = 0.620, 95% CI = 0.481-0.865) to desire more children than women who did not use contraceptives. Compared with those with no education, the odds of desire for more children decreased with education level. On the hand On the other hand, decision-making autonomy concerning the number of children and the preference of boy children increased the odds of the desire for more children., Findings indicate that women who preferred 3–4 boys were 2 times more likely (AOR = 2.021, 95% CI = 0.1.726-2.367) and that those who preferred 5 + children were 1.9 times more likely (AOR = 1.964, 95% CI = 1.580-2.440) to desire more children than those who preferred 0–2 boys.
Discussion
Approximately one in five (21%) high-parity women desired to have more children. The study revealed that having no education was positively associated with the desire for more children. The odds of desire for more children among women with primary education and secondary education were lower than those among women with no education. This finding is similar to those of other studies in Uganda [20,24,25] and Ghana [26], Ethiopia [27] other countries in sub-Saharan Africa [11,28]. This finding suggests that educated women are exposure to health messages, understand the importance of small family size and more likely to make informed choices about the number of children they want to have and prioritize providing better opportunities for their existing children rather than having more. This finding, however, contrasts with Matovu, Makumbi [20] who found that in Uganda, women with primary education had greater desire for additional children compared to those with no education, a pattern attributed to cultural norms and limited socio-economic mobility despite minimal schooling [20]. Similarly, analysis across sub-Saharan Africa by Channon and Harper [29] revealed that education alone may not uniformly reduce fertility desires but its impact is mediated by factors like quality of schooling, exposure to reproductive health services, economic opportunities, and entrenched gender and cultural norms [29].
The findings indicated that catholic women had increased odds of desire for more children compared to Anglicans. This can be linked to the fact that Catholic Church promotes openness to life in marriage and discourages modern contraception. The catholic doctrine emphasizes that children are blessings, and procreation is a central purpose of marriage hence each marital act should remain open to the possibility of life. This finding is similar to other studies in Uganda [20,25]. Muslim and Pentecostal women were less likely to desire more children than Anglican women. Religion has immense significance in most societies and thus plays an important role in promoting acceptance or creating resistance to family planning. This finding is in line with a study performed in Nepal [30,31], which showed that Muslim and Pentecostal women were less likely to desire more children than Anglican women. This finding contradicts the findings of other studies in Ghana [26] Ethiopia [27], Kenya [32] and Tanzania [33], which have shown that Anglican women have less desire for more children than Muslim women.. This is explained by the fact that religious tradition strongly influences the uptake of family planning, with a wide range of interpretations of most religious traditions affecting the perceived acceptability of family planning programs.
The results showed that women with five or more living children were less likely to desire more children. This is because women with five or more living children may be satisfied with their ideal number of children. This finding is consistent the previous study conducted in Uganda comparing predictors across regions and revealed that women with more children are satisfied with their fertility and are more likely to use contraceptives to limit the fertility [34] and another study conducted in 33 countries on marital satisfaction, sex, age, marriage duration, religion and desire for more children which found that women with more than 4 children have less desire for more children [35]. This is partly because, these women may prioritize quality over quantity, focusing on providing the best care and opportunities for their existing children rather than expanding their family further.
Similarly, Women with three or more boys were less likely to desire more children than women with fewer boys. This finding agrees with the findings in Nigeria, Asia and India. In Asia women opt for sex selective abortion in favor of a producing a boy child [36]. Similarly women in India women desire for more child if the first child born is a girl [37]. This is explained by the fact that women with several boys might be contented with family dynamics and not feel the need for additional children. This, however, contrasts with the findings of a study in Taiwan on the value of children, sex preference and fertility desire among young Taiwanese women [38], which showed that the desire for children was associated with the balanced sex composition of children and Iran [39] that showed preference of sex had no significant effect on fertility.
Women who use contraceptives are less likely to desire more children. This is explained by the fact that women who are using contraceptives make informed decisions about family size and might not wish to give birth to additional children. Similar findings consistent with this was reported in Uganda where women who were most women (72%) using modern contraceptives did not intent to have more children in the future [40,41]. The study further revealed that women without decision-making autonomy were more likely to desire more children than their counterparts were. This finding is similar to findings of other studies [42,43] which showed that women with high decision-making autonomy were associated with the desire for no more children. This can be partly explained by the fact that women who lack decision-making autonomy may feel pressured to conform to family expectations or desires and ultimately have more children. Women with limited decision-making autonomy may also face barriers to accessing contraception and family planning services, and in such situations, they may continue to have children because they lack the means to prevent pregnancies.
Conclusions
The study assessed the critical research gap of desire for more children among high parity women who ideally should have attained the desired fertility. Findings indicate that one in five high-parity women desire to have more children. The desire for more children is significantly associated with education level, religion, number of living children, preference of boy child, decision making autonomy and use of modern contraceptives. The study found evidence to accept the hypothesis that age does not significantly affect the desire for more children. The study also found evidence to conclude that decision making autonomy and education level significantly affect the desire for more children. These findings have implications for future fertility thus recommend that policymakers and Programme implementers should work toward providing education and awareness programs on the benefits of family planning, small family size especially to women with no formal education or primary education. The study also recommends empowering women through increased autonomy and participation in household decisions can lead to more balanced fertility preferences, collaboration with religious leaders to promote health education sensitive to religious values while promoting informed decision making. The study further recommends promotion of gender equality to reduce the desire for more children based on gender preference.
This study examined the determinants of desire for more children using a nationally representative data from Uganda’s major regions. The data used is trustworthy because it was collected by a reputable national organization that conducts large surveys and censuses. However, this study, like other cross-sectional studies, cannot draw causal inferences about the desire for more children. The study only looked at relationships between the selected variables and the desire for more children Therefore, an in-depth analysis of the factors associated with the desire for more children through a qualitative approach and trend analysis between 2001 and 2022 is needed to fully understand the desire for more children among high-parity women in Uganda.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1PRB. World population datasheet; 2024 [cited 2025 Apr 8]; Available from: https://2024-wpds.prb.org/data-sheet-download/
- 2United Nations Department of Economic and Social Affairs (UN DESA). World population prospects 2024; 2024. Available from: https://population.un.org/wpp/
- 3Vollset SE, Goren E, Yuan C-W, Cao J, Smith AE, Hsiao T, et al. Fertility, mortality, migration, and population scenarios for 195 countries and territories from 2017 to 2100: a forecasting analysis for the Global Burden of Disease Study. Lancet. 2020;396(10258):1285–306. doi: 10.1016/S 0140-6736(20)30677-2 32679112 PMC 7561721 · doi ↗ · pubmed ↗
- 4Ahinkorah BO, Seidu A-A, Armah-Ansah EK, Budu E, Ameyaw EK, Agbaglo E, et al. Drivers of desire for more children among childbearing women in sub-Saharan Africa: implications for fertility control. BMC Pregnancy Childbirth. 2020;20(1):778. doi: 10.1186/s 12884-020-03470-1 33317476 PMC 7734747 · doi ↗ · pubmed ↗
- 5Ganivet E. Growth in human population and consumption both need to be addressed to reach an ecologically sustainable future. Environ Dev Sustain. 2020;22(6):4979–98.
- 6Atake E-H, Gnakou Ali P. Women’s empowerment and fertility preferences in high fertility countries in Sub-Saharan Africa. BMC Women’s Health. 2019;19(1):54. doi: 10.1186/s 12905-019-0747-9 30953494 PMC 6451210 · doi ↗ · pubmed ↗
- 7Walker RA, et al. Uganda economic update 16th edition: investing in Uganda’s youth. In: Uganda economic update, no. 16. Washington (DC): World Bank Group; 2020.
- 8UBOS. Uganda demographic and health survey. Uganda Bureau of Statistics; 2022.