Effects of Hypopressive Techniques on the CORE Complex: A Systematic Review
Pablo Hernandez-Lucas, Isabel Escobio-Prieto, Paloma Moro López-Menchero

TL;DR
This review examines how hypopressive techniques affect core muscles, finding some benefits but noting poor study quality.
Contribution
The study systematically evaluates the effects of hypopressive techniques on the CORE complex using randomized controlled trials.
Findings
Abdominal hypopressive techniques may improve pelvic floor and transverse abdominis muscle function.
Positive effects on the lumbar region and diaphragm were observed in some studies.
Most studies had high risk of bias and low methodological quality.
Abstract
The CORE complex refers to the muscles of the core region of the body, including the abdominal muscles, lower back muscles, and diaphragm. Among the various techniques aimed at improving CORE strength and functionality, abdominal hypopressive techniques have gained popularity. Objectives: To evaluate the available scientific literature on the effects of AHT on the CORE complex. Methods: A systematic search was conducted in January 2025 in PubMed, Web of Science, PEDro, Cochrane, ClinicalTrials.gov and Scopus. Only randomized controlled trials (RCTs) involving adults were included. Two reviewers independently selected studies and extracted data. The review was registered in PROSPERO (CRD-42023424933) and followed PRISMA guidelines. Results: Of 258 studies identified, 13 of them met the eligibility criteria for the final review. Showing the application of abdominal hypopressive techniques…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
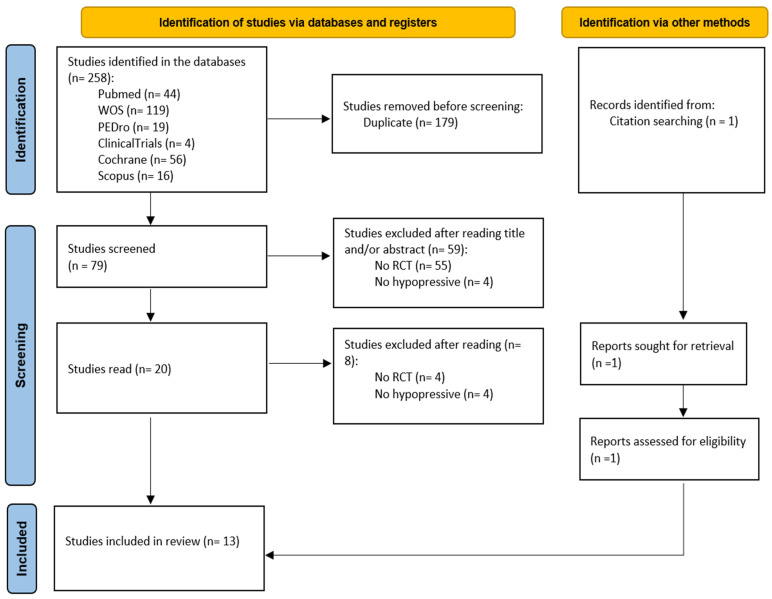 Figure 1
Figure 1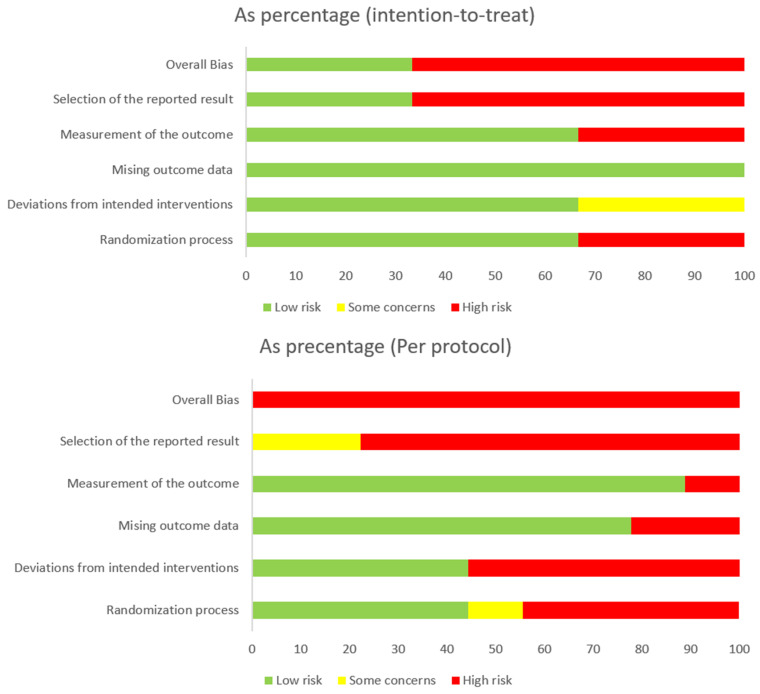 Figure 2
Figure 2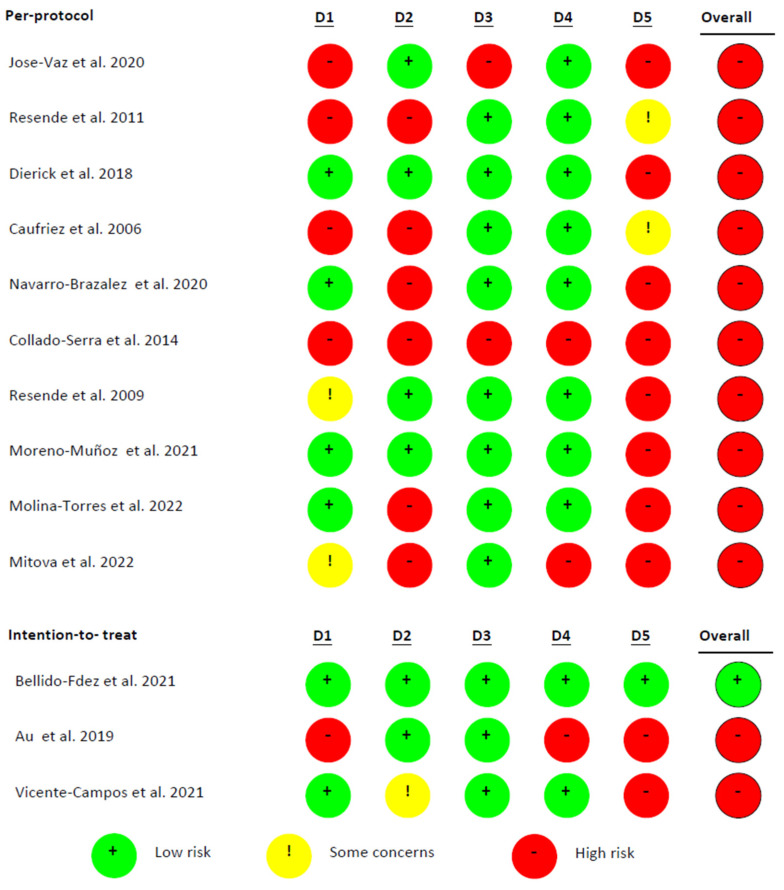 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMusculoskeletal pain and rehabilitation · Anesthesia and Pain Management · Hernia repair and management
1. Introduction
The lumbo-pelvic coxal complex, known as “CORE”, is a three-dimensional region of the body delimited by the diaphragm above, the abdominal muscles on the sides, the paravertebral and glutes behind, and the pelvic floor (PF) muscles below [1]. These structures work synergistically to stabilize the spine and regulate intra-abdominal pressure [1,2]. According to Panjabi’s model [3,4], core stabilization involves three interconnected subsystems: the passive system (comprising vertebrae, intervertebral discs, ligaments, and the passive components of muscles), the active system (consisting of core muscles providing dynamic support), and the neural system (responsible for processing and coordinating motor responses). These subsystems interact continuously to ensure postural control and efficient movement.
Beyond spinal stabilization, the CORE complex also plays a vital role in postural control, force transmission between the upper and lower limbs, motor control, and injury prevention. As such, optimizing the CORE function is crucial for both athletic performance and rehabilitation.
Among the techniques used to target deep musculature and reduce intra-abdominal pressure, the abdominal hypopressive technique (AHT) has gained in popularity. The AHT is a series of postural and respiratory exercises originally developed to improve pelvic floor function and abdominal tonicity. These exercises involve specific body positions combined with expiratory apnea and diaphragmatic aspiration, aiming to generate a reflex activation of deep stabilizing muscles, such as the PF and transversus abdominis (TrA) [5,6,7,8,9,10]. However, despite its growing use in clinical practice, scientific evidence on the physiological effects and functional impact of the AHT remains limited and methodologically inconsistent, particularly regarding its influence on the CORE complex as a whole.
Previous systematic reviews have mainly focused on women with pelvic floor dysfunction [11,12], without comprehensively addressing the effects of the AHT on all CORE-related regions or including male participants. Given that muscle activation patterns during AHT exercises have also been demonstrated in men [10], and that the AHT has shown potential benefits beyond the pelvic floor, such as in the lumbar spine and diaphragm [13], a broader evaluation is warranted.
Therefore, this systematic review aims to analyze the effects of abdominal hypopressive techniques on the CORE complex, considering evidence from randomized controlled trials in both men and women, and examining outcomes across the pelvic floor, abdominal wall, lumbar region, and diaphragm. This broader scope distinguishes the present review from prior literature and seeks to provide a more comprehensive understanding of the AHT’s potential clinical applications.
2. Materials and Methods
2.1. Design
This research was prospectively registered in PROSPERO (code: CRD-42023424933), following the guidelines established by PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) [14], as well as the reporting standards in PRISMA in Exercise, Rehabilitation, Medicine and Sports Sciences (PERSIST) [15] and the recommendations of the Cochrane Collaboration [16].
In January 2025, a comprehensive search for publications was conducted in the following databases: Web of Science, PubMed, PEDro, Cochrane, ClinicalTrials.gov, and Scopus. A variety of combinations were used with the following Medical Subject Headings (MeSH): “pelvic floor”, “pelvic floor disorders”, “abdominal muscles”, “abdominal CORE”, “low back pain”, “back pain”, and “diaphragm.” Additionally, the following free-text terms were included: “hypopressive”, “hypopressive exercise”, and “hypopressive abdominals.”. Appendix A: Table A1 presents the search equations used in each database, which were based on a specific PICO question. P (Population) comprises adults (≥18 years) with symptoms associated with CORE complex dysfunctions, such as pelvic floor disorders, urinary incontinence, low back pain, postural alterations, or post-surgical conditions. I (Intervention) involves the application of the AHT, either as a standalone treatment or within a multimodal approach. C (Comparison) is defined as no intervention, placebo, or other active treatments, such as pelvic floor muscle exercises, massage therapy, biofeedback, or electrostimulation. O (Outcomes) include pelvic floor strength, symptom reduction (e.g., incontinence, pain), postural control, respiratory function, and quality of life. S (Study Design) selected randomised controlled trials and controlled clinical trials published in peer-reviewed journals. Studies were included if they applied the AHT as a central or complementary intervention, assessed at least one predefined outcome, and were available in full text in English or Spanish. Exclusion criteria comprised case reports, reviews, editorials, conference abstracts, studies involving minors or animals, or lacking detailed information on AHT implementation. The search included studies in English and Spanish, with no restrictions on publication status; no filters were applied during the search, and grey literature was not included.
2.2. Study Selection
After eliminating duplicates, two authors (P.M.L.-M.; P.H.-L.) continued reading the titles and abstracts, eliminating the studies that did not agree with the objective of the systematic review. The Kappa coefficient between the first and second reviewers was 0.9, indicating almost perfect agreement. After completing this process, each of them was analyzed applying the following inclusion criteria for the selection studies: (i) men and women, (ii) between 18 and 60 years of age, (iii) randomized controlled studies, and (iv) intervention with the AHT. The following exclusion criteria were also applied: (i) variables related to the CORE were not analyzed, and (ii) the study was not published. After screening the results based on the inclusion criteria using a personalized Microsoft Excel table, the articles for this review were obtained.
2.3. Data Extraction
Two reviewers (P.M.L.-M.; P.H.-L.) extracted the following data for analysis: demographic information (title, authors, journal and publication year), sample characteristics (age, sex and number of participants), specific parameters of the study (duration of the intervention, adverse events and exercise methods), and the results obtained (variables analyzed, instruments used and follow-up time). Tables were used to describe both study characteristics and extracted data.
2.4. Quality Assessment
The PEDro scale [17] was used to evaluate the quality of these studies and the RoB scale (Risk of Bias) [18] tool was applied to evaluate the risk of bias. Two reviewers (P.M.L.-M.; P.H.-L.) applied the PEDro and RoB scales. In cases where the reviewers disagreed, a third reviewer (I.E.-P.) was consulted to make the final decision regarding the inclusion or exclusion of a study from the analysis.
3. Results
Out of 258 search results, 79 studies were considered eligible for inclusion after removing duplicates and reviews. Among the 79 articles screened, 59 were excluded after abstract and title screening. Of the 20 full-text articles assessed for eligibility, eight were excluded. Thirteen articles were ultimately included in the synthesis [19,20,21,22,23,24,25,26,27,28,29,30] and a new article was added in the author search [31] (Figure 1).
3.1. Methodological Quality of the Studies and Risk of Bias
The average score of all articles included in this review was 6.6 points, which indicated a moderate methodological quality (Table 1) [17]. The articles with the lowest score obtained five points [23,29] and those with the highest score attained eight points [22,27].
According to the Cochrane Collaboration Tool to assess the RoB, of the 13 studies, three are intention-to-treat [22,25,28] and nine are per protocol [19,20,21,23,24,27,29,30,31]. One of them presents a low RoB [22] and the rest show a high RoB [19,20,21,23,24,25,26,27,28,29,30,31] (Figure 2 and Figure 3).
3.2. Participants
A total of 992 people participated in the 13 studies [19,20,21,22,23,24,25,26,27,28,29,30,31], and the mean age was 42.4 years, with a range from 23 to 63 years. It is worth mentioning that three articles do not describe the age or the participants [23,29,31] (Table 2).
3.3. Interventions
In the 13 articles included in this review, the AHT intervention group could be used as a single technique [19,22,24,26,27,28,29,30,31] or combined with PF exercises [20,21,23,24,25,29] or with massage therapy [22]. It is compared with a control group in which they have no intervention [20,23,24,26,27,28], a PF exercise group [19,20,24,25,29,30], an electro-biofeedback group [21], a massage therapy group [22], and a postural training group [31] (Table 3).
The AHT exercises were carried out according to these guidelines: self-elongation, neutral position of the pelvis, ankle dorsiflexion, knee flexion, activation of the shoulder girdle muscle, three respiratory cycles with lateral costal breathing and slow deep exhalation (inspiration, maximum exhalation), and maintaining breathing after expansion of the rib cage (diaphragmatic aspiration), with a learning respiratory pattern of complete expiration and diaphragmatic aspiration [20,21,24,30]. In two articles, prior learning is not indicated [22,23]. In one of the articles, diaphragmatic aspiration was not performed, but abdominal contraction was performed during expiratory apnea [29] (Table 3).
The AHT exercises were static with different positions of the limbs in the supine, sitting and biding positions [19,20,24], and with quadrupedy [21]. In others, a dynamic progression was made from the standing to supine positions [26,27,30,31]. In the remaining studies, the type of technique is not specified [22,23,25,28,29]. The duration of the treatment varied between 3 weeks [21] and 25 weeks [25], with an average of 14 weeks. On average, three sessions were conducted per week, with each session lasting approximately 38 min. Treatment intensities ranged from brief interventions of 20 min twice per week to an intensive regimen of up to 45 min, five times per week over several months.
3.4. Effects
Regarding the articles that assess PF strength [19,20,21,24,27,30], it is observed that the AHT group does not increase the strength variables compared to the PF exercise group [19,21] or that there is no significant difference between both groups [20,24,30]. However, the AHT group significantly increases the strength variables compared to the control group [20,27] and compared to baseline levels [19,20,21,24,27,30].
In five articles, urinary incontinence (UI) is assessed [19,23,25,27,29] and a significant decrease in symptoms is observed in the AHT group compared to baseline values [19,23,25,27,29] and compared to the control group [23,27]. But regarding the PF muscle exercise (PFMX), one article shows improvement in UI compared to the AHT [19] and in another, there are no significant differences between groups [25]. Finally, Mitova et al., 2022, obtained significant changes in UI in favor of the AHT group in combination with Kegel exercise, compared to AHT and Kegel exercise groups used alone [29]. In the articles that assess the abdominal region [24,26,29], it is observed that the AHT group improves the variable of postural control [26,29] and abdominis transversus (TrA) strength compared to baseline levels [24,26,29] and the control group [24,26,29].
Two articles assess lumbar flexibility [22,31], and it is observed that the AHT group improves the mobility variable compared to baseline levels [22,31] and compared to the postural training group [31]. Furthermore, the AHT group in combination with massage therapy significantly improves disability compared to only using massage therapy or only performing AHT exercises [22].
Finally, only one article assesses the effect on the diaphragm [28], in which they observed that the AHT group improves the variables of diaphragmatic thickness and forced inspiration compared to basal levels and the control group.
4. Discussion
The main objective of this review was to analyze the available scientific literature on the effects of the AHT on CORE. The results of the articles included in this systematic review suggest that the AHT could have positive effects at the level of the PF, TrA, lumbar region and diaphragm.
In this systematic review, six studies assessed the strength of the pelvic floor (PF) [19,20,21,24,27,30]. Although the AHT group showed significant improvements compared to baseline levels in most studies [19,20,21,24,27,30], the true between-group differences were more limited. Specifically, the AHT group did not show superior improvements compared to the pelvic floor muscle exercise (PFMX) group in several studies [19,21], and no significant differences were found between these two interventions in others [20,24,30]. For example, Resende et al. (2012) reported no significant advantage in adding the AHT to PFMX compared to performing PFMX alone. Similarly, Jose-Vaz et al. (2020) found greater improvements in PF strength variables in the PFMX group compared to the AHT group. However, the AHT group did demonstrate significantly better outcomes when compared to control groups [20,24,27], which suggests a potential benefit of the AHT in the absence of active intervention. This may be due to the reflexive activation of the musculature during AHT exercises, promoted by postural guidelines such as axial self-elongation, shoulder girdle activation, and a neutral pelvis [32,33]. These elements, combined with expiratory apnea and rib cage expansion, generate negative pressure in the abdominal cavity that may involuntarily activate type I slow-twitch fibers of the PF and abdominal muscles, enhancing muscle tone and endurance [30]. In contrast, PFMX involves voluntary contractions that mainly recruit type II fast-twitch fibers, which are associated with greater force generation [30].
In this work, five articles evaluate UI [19,23,25,27,29]. They show significant improvements in the AHT group compared to baseline values [19,23,25,27,29] and compared to the control group [23,27]. Nevertheless, regarding the PFMX group, the results are ambiguous; one article shows improvement in stress urinary incontinence (SUI) compared to the AHT [19] and, in another article, there are no significant differences between groups [25]. Furthermore, Mitova et al., 2022, obtained significant improvements in UI in the AHT group in combination with Kegel compared to groups using only AHT or Kegel exercises [29]. Similarly, leading clinical guidelines suggest conservative treatment using therapeutic exercises and lifestyle modifications as the first-line intervention [34].
Only three articles that assess the strength of the TrA [24,26,29] obtained significant improvements in all of them [24,26,29]. This may be due to the fact that the activation of the shoulder girdle and the neutral pelvis position are related to the activation of the CORE [35]. Furthermore, axial self-elongation and abdominal activation are strongly related due to optimal spinal alignment, activation of deep CORE muscles, balanced distribution of intra-abdominal pressure, muscle synergy, improved body awareness and reflex activation [36]. Other authors pointed out a decrease in waist circumference measurement after the intervention with the AHT, associating this effect with an activation of TrA [37,38,39].
Two articles [22,31] assessed lumbar flexibility, obtaining a significant increase in the mobility of this posterior region of the CORE in both studies [22,31]. Furthermore, the AHT group in combination with massage therapy significantly improved disability compared to only using massage therapy or only performing AHT exercises [22]. Along the same lines, the mobility of the lumbar region was evaluated by Ria et al., 2014, showing improvement after an AHT session [37]. On the other hand, the mobility of the lumbar region and TrA strength are important to address low back pain [40]. Previous research also relates AHT to improvements in pain and disability associated with low back pain [13,41].
Only one of the articles in our review [28] assessed the diaphragm of subjects performing AHT exercises and both diaphragmatic thickness and forced inspiration [28]. The benefits of these parameters could be explained by the sustained eccentric contraction of the diaphragm during AHT performance. In a different investigation, another respiratory parameter significantly increased in participants who performed AHT exercises—peak expiratory flow [39]. This means that the abdominal muscles contracted more to expel air more quickly [42]. This is related to the three articles that assessed the increase in TrA strength after performing AHT exercises [24,26,29].
The results obtained in the articles included in this systematic review must be interpreted with caution due to the following reasons: the high heterogeneity of the protocols; the insufficient methodological quality according to the PEDro scale, and 12 of the 13 articles present a high risk of bias [19,20,21,23,24,25,26,27,28,29,30,31]. Furthermore, it should be noted that the duration of the AHT interventions varied substantially across the included studies (ranging from 3 to 26 weeks), which may influence the magnitude of the reported effects. In addition, there were methodological differences regarding the use of static versus dynamic techniques, as well as the application of complementary therapies (such as pelvic floor muscle training, massage therapy, or electrostimulation). Several studies also lacked key participant data (e.g., age or baseline characteristics), which weakens the interpretability and comparability of the results. This variability limits the generalizability of the findings and hinders the identification of the specific component responsible for the observed effects. Moreover, due to the clinical and methodological heterogeneity of the included studies, it was not possible to conduct a meta-analysis, which restricts the statistical strength and precision of the overall conclusions.
Therefore, further research is needed to analyze the effects of the AHT in the CORE region, with larger samples and long-term follow-ups that help confirm these initial findings. Given the generally high risk of bias and methodological limitations in the included studies, the current evidence should be considered preliminary. The findings regarding the effectiveness of the AHT remain mixed, with some trials showing improvements and others reporting no significant differences compared to established interventions, such as pelvic floor muscle training. To advance this area of research, future studies should adopt standardized AHT protocols with clearly defined parameters, include larger and more diverse populations, and incorporate extended follow-up periods. High-quality randomized controlled trials with blinded assessments and rigorous methodological designs are essential before any firm clinical recommendations can be made.
Given the overall high risk of bias and methodological limitations identified in most of the included trials, the current evidence should be interpreted as preliminary. While some studies report positive effects of the AHT on PF strength, TrA activation, lumbar mobility, and diaphragm function, the findings are mixed and often inconsistent between studies. Notably, several trials failed to demonstrate superiority of the AHT over conventional pelvic floor muscle training. Therefore, the heterogeneity of protocols and the conflicting outcomes across studies highlight the urgent need for well-designed, high-quality randomized controlled trials before clinical recommendations can be made with confidence.
5. Conclusions
The results of the articles included in this systematic review suggest that the AHT could have positive effects at the level of the PF, TrA, lumbar region and diaphragm. However, the methodological quality of the scientific literature is preliminary and presents high risk of bias. Therefore, further research is necessary to confirm these findings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Akuthota V. Nadler S.F. Core strengthening Arch. Phys. Med. Rehabil.200485869210.1053/j.apmr.2003.12.00515034861 · doi ↗ · pubmed ↗
- 2Smith C.E. Nyland J. Caudill P. Brosky J. Caborn D.N. Dynamic trunk stabilization: A conceptual back injury prevention program for volleyball athletes J. Orthop. Sports Phys. Ther.20083870372010.2519/jospt.2008.281418978452 · doi ↗ · pubmed ↗
- 3Panjabi M.M. The stabilizing system of the spine. Part I. Function, dysfunction, adaptation, and enhancement J. Spinal Disord.1992538339710.1097/00002517-199212000-000011490034 · doi ↗ · pubmed ↗
- 4Panjabi M.M. The stabilizing system of the spine. Part II. Neutral zone and instability hypothesis J. Spinal Disord.1992539039710.1097/00002517-199212000-000021490035 · doi ↗ · pubmed ↗
- 5Rami-Colás C. Martín-Nogueras A.M. Physiotherapy treatment of idiopathic scoliosis: Schroth versus hypopressive gymnastics Fisioterapia 201638283710.1016/j.ft.2015.01.002 · doi ↗
- 6Soto González M. Da Cuña Carrera I. Gutiérrez Nieto M. López García S. Ojea Calvo A. Lantarón Caeiro E.M. Early 3-month treatment with comprehensive physical therapy program restores continence in urinary incontinence patients after radical prostatectomy: A randomized controlled trial Neurourol. Urodyn.2020391529153710.1002/nau.2438932442334 · doi ↗ · pubmed ↗
- 7Caufriez M. Fernández J.C. Guignel G. Heimann A. Comparación de las variaciones de presión abdominal en medio acuático y aéreo durante la realización de cuatro ejercicios abdominales hipopresivos Rev. Iberoam. Fisioter. Kinesiol.200710122310.1016/S 1138-6045(07)73661-4 · doi ↗
- 8Navarro Brazález B. Sánchez Sánchez B. Prieto Gómez V. De La Villa Polo P. Mc Lean L. Torres Lacomba M. Pelvic floor and abdominal muscle responses during hypopressive exercises in women with pelvic floor dysfunction Neurourol. Urodyn.20203979380310.1002/nau.2428431985114 · doi ↗ · pubmed ↗