Exploring a role for Chemerin in the cardiovascular and musculoskeletal benefits of intradialytic exercise in the hemodialysis population
Mingyue Deng, Daniel S. March, Darren R. Churchwood, Hannah M. L. Young, Patrick J. Highton, Matthew J. Denniff, Matthew P. M. Graham-Brown, James O. Burton, Luke A. Baker

TL;DR
This study explores whether chemerin, a protein linked to inflammation, is involved in the cardiovascular and musculoskeletal benefits of intradialytic cycling in hemodialysis patients.
Contribution
The study is the first to show that plasma chemerin levels increase with time on hemodialysis, but it does not support a role for chemerin in modifying cardiac structure or function.
Findings
Plasma chemerin concentrations increased significantly after 6 months in both the IDC and control groups.
Chemerin was positively associated with physical performance at baseline but not with cardiovascular or body composition markers.
No evidence was found to support a role for chemerin in modifying cardiac structure or function in response to intradialytic cycling.
Abstract
Cardiovascular disease is the leading cause of death for people receiving hemodialysis. Intradialytic cycling (IDC) has been shown to improve cardiovascular health in the hemodialysis population, but specific mechanisms require elucidation. Chemerin is an adipokine which contributes to the inflammatory process and may be associated with the cardiovascular benefits of IDC and physical function in hemodialysis population. Adults undertaking ≥3 months hemodialysis were randomized to either IDC (30 min each time, moderate intensity, thrice weekly) and usual care; or usual care only (control group). 88 blood samples were retrospectively analyzed for chemerin concentrations using ELISA. Unadjusted and adjusted linear regression was used to understand how changes in chemerin are associated with changes in cardiovascular and musculoskeletal health in response to IDC. There was a significant…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
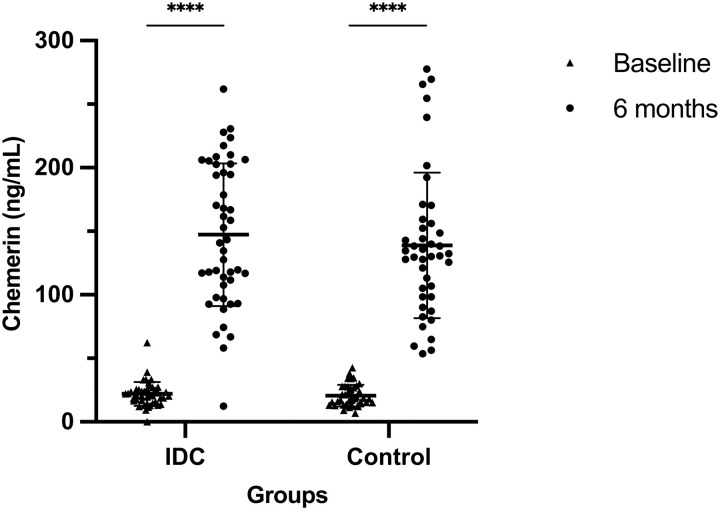 Fig 1
Fig 1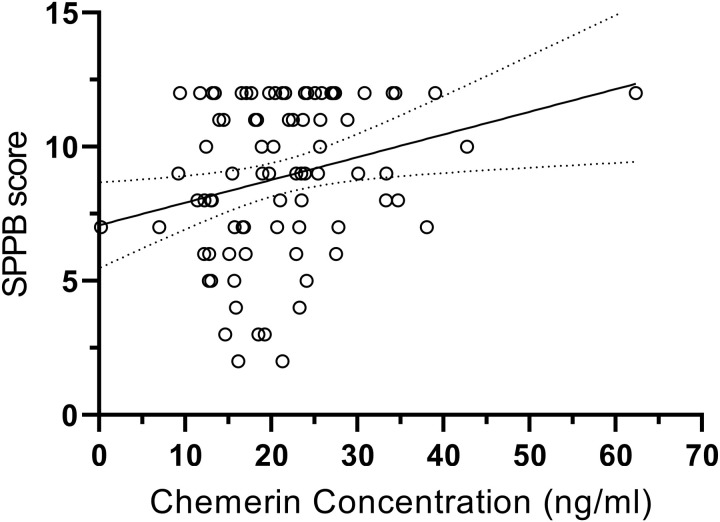 Fig 2
Fig 2- —National Institute of Health Research
- —Leicester Hospitals Charity Kidney Care Appeal
- —Stoneygate Trust
- —National Institute for Health and Care Research (NIHR) Leicester Biomedical Research Centre (BRC)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsExercise and Physiological Responses · Children's Physical and Motor Development · Adipokines, Inflammation, and Metabolic Diseases
Introduction
Cardiovascular disease (CVD) is the leading cause of death for people with end-stage kidney disease (ESKD) receiving hemodialysis [1–3]. Studies have concluded systemic inflammation, endothelial activation, vascular calcification, accumulation of gut microbiota-derived uremic toxins and anemia as non-traditional risk factors of CVDs in hemodialysis population [3,4]. As a result of the pro-inflammatory state within this population (through factors such as the dialysis process itself) and the additional stress to endotoxin exposure, the internal antioxidant system is impaired [3,5]. The chronic inflammatory environment is characterized by elevated levels of intracellular reactive oxygen species (ROS) and circulating inflammatory factors [5], which contribute to vascular and myocardial remodeling in this population. Recently, A 6-month intradialytic cycling (IDC) intervention has been shown to improve significant cardiovascular structure and function in the hemodialysis population [2], though the specific mechanisms that drove these adaptations are not known.
Chemerin, a novel adipokine predominantly secreted from the liver and white adipose tissue in its precursor form [6,7], is cleaved into different bio-active forms [8]. Research has shown it elicits its biological effects via 3 G-protein-coupled receptors, in which chemokine-like receptor 1 (CMKLR1/ChemR23) is suggested to be the main receptor of action [9–11]. Over-activated chemerin/ChemR23 axis has been shown to disturb the function of endothelial cells, vascular smooth muscle cells, and perivascular adipose tissue by inducing proliferation, lipid deposition and inflammation, contributing to the development of CVD risk factors in chronic kidney disease (CKD) [3,11,12]. However, a significant survival advantage brought by increased chemerin has been reported in dialysis population, which persisted after adjustment for inflammation [13]. This may be related with the vascular protective potential of chemerin/ChemR23 signaling [14], though further investigation is required to understand the relationship between chemerin and cardiovascular factors in the hemodialysis population. Previous work suggests circulatory chemerin concentrations are associated with physical inactivity in metabolic disorders, and a suppressive effect of exercise on circulating chemerin has been reported in patients with metabolic disorders including obesity and type 2 diabetes [15]. It may impair glucose uptake, induce insulin resistance, contribute to excessive levels of pro-inflammatory cytokines and mitochondrial ROS in skeletal muscle, all of which lead to exacerbation of muscle wasting [16,17]. However, we do not know the relationship between chemerin and physical function in the hemodialysis population.
Therefore, this retrospective analysis of the CYCLE-HD study aimed to investigate the association between chemerin and the CV benefits noted in response to IDC. As a secondary analysis, we investigated a role for chemerin in skeletal muscle mass, function and body composition in hemodialysis population.
Methods
Participants
Individuals receiving hemodialysis (>3 months) ≥18 years of age were eligible for inclusion. The CYCLE-HD trial was given ethical approval by the National Health Service (NHS) Research Ethics Committee East Midlands (Northampton, UK; Ref: 14/EM/1190) and was conducted according to the Declaration of Helsinki. All participants provided written informed consent and the trial recruitment period was from March 2015 until April 2018, demographic and clinical characteristics were collected at the point of recruitment to align with trial-specific outcome measures.
Study design
This study was a retrospective analysis of the 6-month CYCLE-HD trial (ISRCTN1129707). Detailed descriptions of the trial design, including randomization, specific inclusion and exclusion criteria and data collection procedures, are described previously [18]. Briefly, in an open-label, blinded endpoint, cluster randomized controlled trial, adults undergoing maintenance hemodialysis were received either a 6-month structured, progressive program of IDC and usual care (IDC group) or usual care only (control group). Participants in IDC group used specially adapted and calibrated cycle ergometers (Letto series; Motmed, Reck, Germany) 3 times a week, aiming for 30 minutes of continuous cycling at a Rating of Perceived Exertion of between 12–14. Resistance was adjusted by increasing the gears on the bike as required to progress training.
Quantification of plasma Chemerin
Blood samples were collected from the arterial dialysis needle before each dialysis (i.e., after the short interdialytic break) and centrifugated at 2500 × g for 15 min at 20°C. Plasma was stored at −80°C prior to analysis of chemerin. Plasma level of chemerin was quantified using the Colorimetric ELISA Kit (Human Chemerin Quantikine ELISA; R&D Systems, Minneapolis, MN, USA) according to the manufacturer’s instructions. All reagents, including diluted sample (1:100), were prepared. Wavelength of microplate reader was set to 450 nm first and then to 570 nm to get the first and second reading results for the correction of optical imperfections. The quantification was performed in February 2024 and the coefficient of variation between analysis plates was deemed to be within acceptable ranges.
Outcome acquisition
Bioimpedance spectroscopy (BIS) (BCM Fresenius Medical Care, Bad Homburg, Germany) was used to measure body composition before dialysis. The short physical performance battery (SPPB) (which includes gait speed along with the sit-to-stand 5 and balance test) and 60-s sit-to-stand (STS60) test were performed on a non-dialysis. Physical activity was measured using the SenseWear Pro3 Armband (BodyMedia, Pittsburgh, PA, USA), an accelerometer with physiological sensors. Participants were instructed to wear the accelerometer for 7 days on the upper arm (the opposite arm of their vascular access). Steps per day were calculated as the average for total days worn (i.e., the total number of steps divided by days worn). All participants underwent cardiac magnetic resonance imaging on a 3-T platform (Skyra; Siemens Medical Imaging, Erlangen, Germany). Prognostically important measures of cardiovascular structure and function were acquired, including: LV mass index (ratio of LV mass to body surface area); LV Mass/Left Ventricular End Diastolic Volume (LVM/LVEDV); LV Ejection Fraction (LVEF), Global Native T1 (measure of myocardial fibrosis and inflammation); and Pulse Wave Velocity (PWV) with methods for acquisistion as previously described [2,18–20].
Statistical analysis
The data were presented as mean ± standard deviation (SD) or number (percentage). The normality was checked by ‘p value’ from the Shapiro-Wilk test. The changes of plasma chemerin, measure of CVD, body composition and physical function markers following the 6-month intervention were obtained from data at 6 months minus baseline data. Difference of change value of chemerin between groups was measured by a linear regression with baseline value of chemerin and groups as independent variables. Unadjusted linear regression of chemerin with CV markers, body composition and physical function were performed at baseline and in the change of 6 months. Significant associations of chemerin were further explored using a multiple linear regression, adjusting for age, sex, body mass index (BMI), hemoglobin, dialysis vintage, ultrafiltration volume, history of diabetes and CVDs. All statistical analyses were performed using the Statistical Package for the Social Sciences program (SPSS for Windows, version 29; Chicago, IL, USA) and figures were produced on GraphPad Prism version 10 (GraphPad Software, San Diego, CA, USA). A p < 0.05 was considered statistically significant.
Results
The CYCLE-HD trial enrolled from March 2015 to April 2018. This retrospective analysis was undertaken on n = 88 participants for whom we had remaining pre and post-intervention plasma blood samples for (IDC group, n = 46; control group, n = 42) (there were n = 130 reported in the primary CYCLE-HD report [2]). Demographic data is presented in Table 1. The control group was older (p = 0.049), and there was a higher percentage of males than the IDC group (p = 0.111) (Table 1).
Table 1: Baseline demographic characteristics of participants.
Change in plasma chemerin following a 6-month intradialytic exercise program
The plasma concentration of chemerin was increased in both IDC and control groups after 6 months (p *< *0.0001) (Fig 1). There was no significant difference in the concentration change (p = 0.449) between groups in response to the 6-month program. There was no significant correlation between baseline chemerin level and its change value following 6-month program between groups (F = 0.529, p = 0.469) (Table 2).
Table 2: Linear regression of chemerin between change value and baseline level between groups.
*Plasma chemerin levels for IDC (n = 46) and control (n = 42) participants at baseline and 6 months.The scatter dot plots were lined at mean with SD. ***P < 0.0001.
Associations of chemerin with markers of CVD, body composition and physical function
There was a significant correlation between chemerin and SPPB in all participants at baseline (β = 0.264, p = 0.017) (Table 3) (Fig 2). After adjustment for covariates including age, BMI, sex, hemoglobin, dialysis vintage, ultrafiltration volume, presence of diabetes and history of CVD, the correlation was no longer significant (β = 0.127, p = 0.245) (Table 4). There was no significant correlation of chemerin with CVD, body composition and other physical function markers at baseline and in the change value over 6 months (Table 3).
Table 3: Unadjusted linear regression of chemerin with CVD, body composition and physical function markers at baseline.
Table 4: Association between chemerin and SPPB at baseline, adjusted for covariates.
Scatter plot of the unadjusted correlation between SPPB and chemerin at baseline.There was a significant correlation between chemerin and SPPB in all participants at baseline. SPPB, short physical performance battery.
Discussion
This study reported 6-month of IDC had no effect on circulating chemerin concentrations, which were seen to be elevated after 6-month on hemodialysis. There were no significant associations between circulating chemerin (both at baseline and in the change value over 6 months) and the measure of CVD or body composition. A positive association between chemerin and SPPB was shown, however, this did not remain after adjustment.
This study has found a considerable elevation in plasma levels of chemerin following 6-month of hemodialysis treatment. However, a 6-month program of IDC did not have any effect on circulating levels of chemerin. As chemerin plays a noticeable role in inflammation, this result mirrors the change of other inflammatory markers (interleukin-6, interleukin-10, tumor necrosis factor alpha and C-reactive protein) in previously published data for other circulating inflammatory markers from the CYCLE-HD trial [21] and suggests no effect of a 6-month program of IDC on the inflammatory state of those on hemodialysis [5,22]. As the molecular weight of chemerin exceeds the filtration limit of hemodialysis, circulating chemerin would be poorly cleared. This result may be the case that the length of the intervention may not be sufficient to modify circulating levels of chemerin. Furthermore, it is well understood that exercise intensity plays a key role in the activation of anti-inflammatory cytokines and as such the moderate exercise intensity (Rating of Perceived Exertion 12 ~ 14) is likely to be insufficient to induce a significant response [23]. In spite of our findings here, there is evidence that habitual physical activity may be able to modify systemic inflammation in the hemodialysis population [21].
No correlation has been detected between chemerin and prognostically significant measures of cardiac structure and function assessed with cardiac magnetic resonance imaging, which suggests that it may not play a role in the cardiovascular remodeling (Table 3). Chemerin has been implicated in the development of CVDs in CKD, such as coronary artery disease, hypertension and heart failure [3,11,12]. in vitro studies have showed a chemerin-induced apoptosis of murine cardiomyocytes and remodeling of vascular smooth muscle cells with the regulation of insulin and inflammatory cytokines [10,24], while chemerin has been reported as an inhibitor of vascular calcification based on the observation in CKD patients [14]. In spite of the potential paradoxical role of chemerin in the development of CVDs [11,13,25], it did not associate with any of the cardiovascular structure or function markers in this data.
To the best of our knowledge, this is the first study to identify the positive correlation between chemerin and physical performance in hemodialysis population, which is contrary to the findings of other inflammatory factors [21]. This correlation was no longer significant when adjusting for age, BMI, sex, hemoglobin, dialysis vintage, ultrafiltration volume, presence of diabetes and history of CVDs. Physical inactivity is significant associated with increased adverse CV events and mortality of hemodialysis population [26], which could also contribute to exacerbation of muscle loss, consequently leading to sarcopenia [27]. Studies have previously reported a disruption mediated by chemerin in bone metabolism and insulin signaling in muscle, which may contribute to the muscle wasting [16,17], osteoporosis [28], and associated frailty in people with metabolic disorders. Given that the systemic biological environment of hemodialysis population is complex, and is characterized by persistent inflammation, repeated disturbance in protein-energy balance, and a myriad of medications, further investigations are required to elucidate the role of chemerin in musculoskeletal complications in the hemodialysis environment [5,29]. In addition, although chemerin is mainly secreted from adipose tissue [6,7], no correlation has been detected between chemerin and body composition. Reduced glomerular filtration rate in ESKD patients would provide part of explanation for this finding [7,25] but further investigation is required to confirm or deny this hypothesis.
Limitation and future research
Several limitations of this study should be acknowledged. Firstly, available technologies only allowed us to measure prochemerin, the circulating in-active full-length form of chemerin. Future work should look to quantify the cleaved active forms of chemerin in order to better elucidate the mechanistic effects of this adipokine and its metabolites. This would be repeated in other clinical populations where sarcopenia is prevalent to further understand the relationship between chemerin and musculoskeletal health. Future work should also look to ascertain the true origin of chemerin production in those with CKD, in order to understand both mechanism of action and potential therapeutic interventions, particularly in the context of musculoskeletal health and exercise interventions. In addition, the concentration of chemerin in local metabolic organs and its interaction with the circulating level are suggested to be taken into consideration when exploring its biological roles [6].
Conclusion
This study has observed an increased circulatory level of chemerin over 6-month hemodialysis. No correlation has been shown to support a role of chemerin in CV benefits in response to intradialytic exercise. The significant correlation between chemerin and SPPB at baseline suggested that chemerin may be associated with physical function in the hemodialysis population. Further studies should explore the link between chemerin and musculoskeletal health in hemodialysis population in order to further understand its role in cardio/muscular health.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chirakarnjanakorn S, Navaneethan SD, Francis GS, Tang WH. Cardiovascular impact in patients undergoing maintenance hemodialysis: Clinical management considerations. Int J Cardiol. 2017;232:12–23.28108129 10.1016/j.ijcard.2017.01.015PMC 5316356 · doi ↗ · pubmed ↗
- 2Graham-Brown MPM, March DS, Young R, Highton PJ, Young HML, Churchward DR, et al. A randomized controlled trial to investigate the effects of intra-dialytic cycling on left ventricular mass. Kidney Int. 2021;99(6):1478–86. doi: 10.1016/j.kint.2021.02.027 34023029 · doi ↗ · pubmed ↗
- 3Jankowski J, Floege J, Fliser D, Böhm M, Marx N. Cardiovascular disease in chronic kidney disease: pathophysiological insights and therapeutic options. Circulation. 2021;143(11):1157–72.33720773 10.1161/CIRCULATIONAHA.120.050686 PMC 7969169 · doi ↗ · pubmed ↗
- 4Filipska I, Winiarska A, Knysak M, Stompór T. Contribution of Gut Microbiota-Derived Uremic Toxins to the Cardiovascular System Mineralization. Toxins (Basel). 2021;13(4):274. doi: 10.3390/toxins 13040274 33920096 PMC 8070663 · doi ↗ · pubmed ↗
- 5Highton PJ, March DS, Churchward DR, Grantham CE, Young HML, Graham-Brown MPM, et al. Intradialytic cycling does not exacerbate microparticles or circulating markers of systemic inflammation in haemodialysis patients. Eur J Appl Physiol. 2022;122(3):599–609. doi: 10.1007/s 00421-021-04846-7 34854982 PMC 8854296 · doi ↗ · pubmed ↗
- 6Lin X, Yang Y, Qu J, Wang X. Aerobic exercise decreases chemerin/CMKLR 1 in the serum and peripheral metabolic organs of obesity and diabetes rats by increasing PPARγ. Nutr Metab. 2019;16:17.10.1186/s 12986-019-0344-9PMC 640213630873215 · doi ↗ · pubmed ↗
- 7Ferland DJ, Mullick AE, Watts SW. Chemerin as a driver of hypertension: a consideration. Am J Hypertens. 2020;33(11):975–86.32453820 10.1093/ajh/hpaa 084PMC 7759724 · doi ↗ · pubmed ↗
- 8Bonomini M, Pandolfi A. Chemerin in renal dysfunction and cardiovascular disease. Vascul Pharmacol. 2016;77:28–34. doi: 10.1016/j.vph.2015.10.007 26545628 · doi ↗ · pubmed ↗