Occupational Health Effects of Chlorine Spraying in Healthcare Workers: A Systematic Review and Meta-Analysis of Alternative Disinfectants and Application Methods
Luca Fontana, Luca Stabile, Elisa Caracci, Antoine Chaillon, Kavita U. Kothari, Giorgio Buonanno

TL;DR
This study reviews the health risks of chlorine spraying for healthcare workers and finds it increases respiratory issues, suggesting safer alternatives and better protection.
Contribution
The paper provides a systematic review and meta-analysis comparing chlorine-based disinfectants and application methods with alternatives in healthcare settings.
Findings
Chlorine-based products significantly increase respiratory condition risk (OR 1.71).
Spraying is associated with higher respiratory risk compared to other methods (OR 2.25).
Moderate-certainty evidence supports safer disinfectants and protective measures over banning methods.
Abstract
Chlorine spraying was widely used during filovirus outbreaks, but concerns about occupational health risks led to a shift toward wiping. This systematic review aimed to evaluate the health risks associated with exposure to disinfectants among healthcare workers (HCWs), with a specific focus on chlorine-based products and spraying compared to alternative disinfectants and general disinfection tasks (GDTs). PubMed, Embase, and Scopus were searched from inception to March 2025. Eligible studies included observational or experimental research on HCWs exposed to chemical disinfectants. Two reviewers independently screened studies, assessed the risk of bias using a validated occupational health tool, and evaluated evidence certainty with the GRADE approach. Meta-analyses used fixed- and random-effects models; heterogeneity was assessed with I2 statistics. Out of 7154 records, 29 studies were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
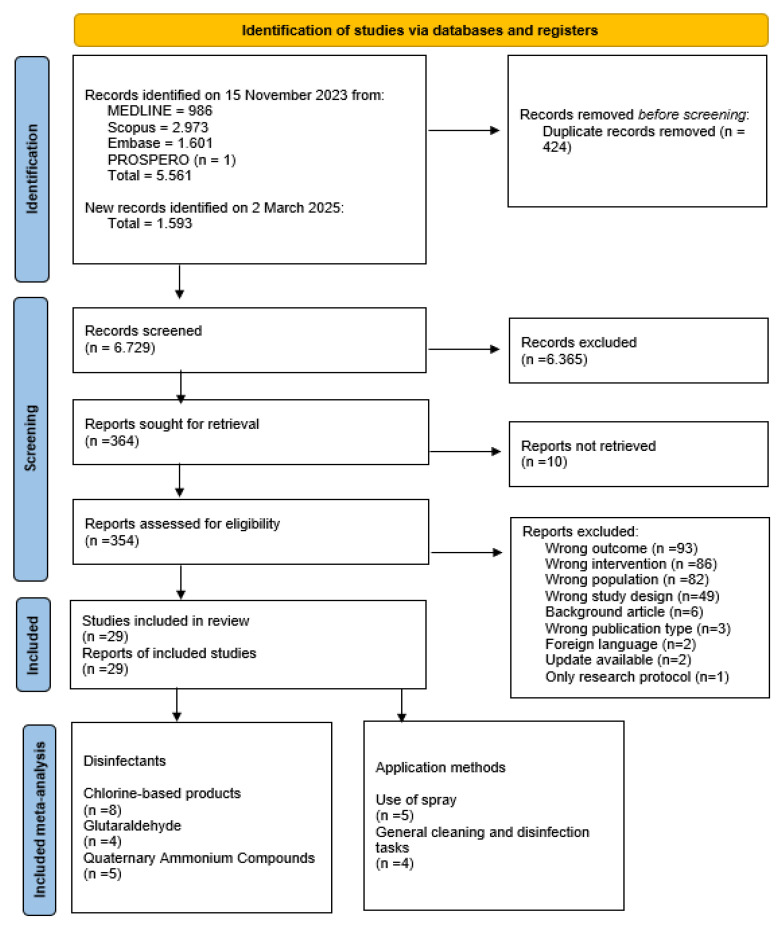 Figure 1
Figure 1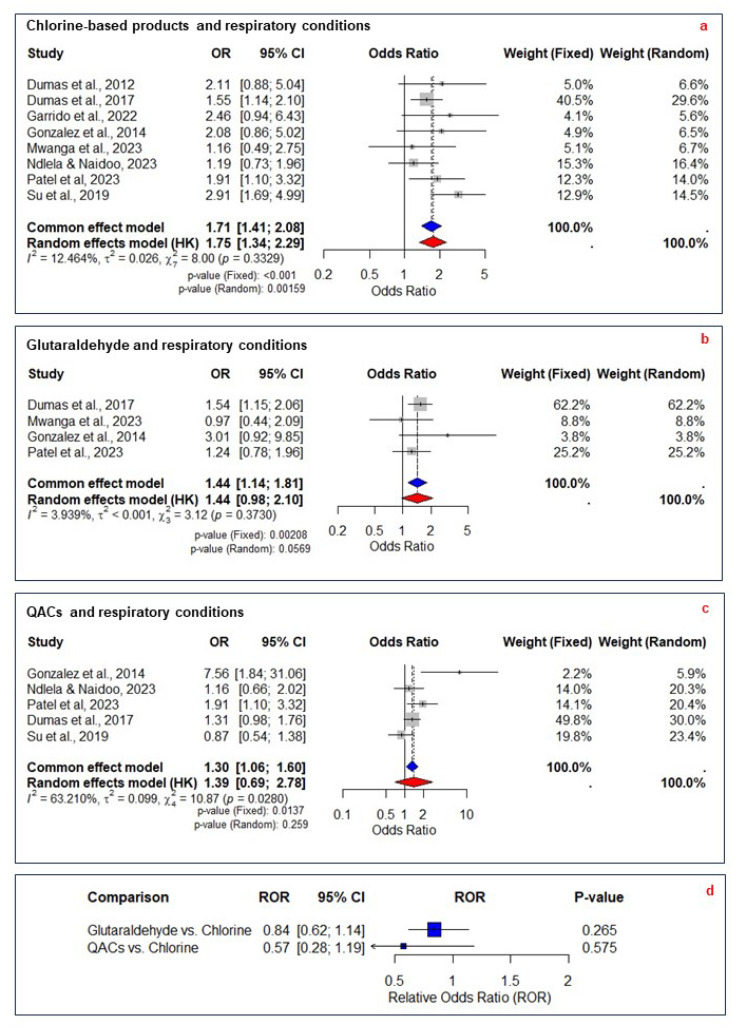 Figure 2
Figure 2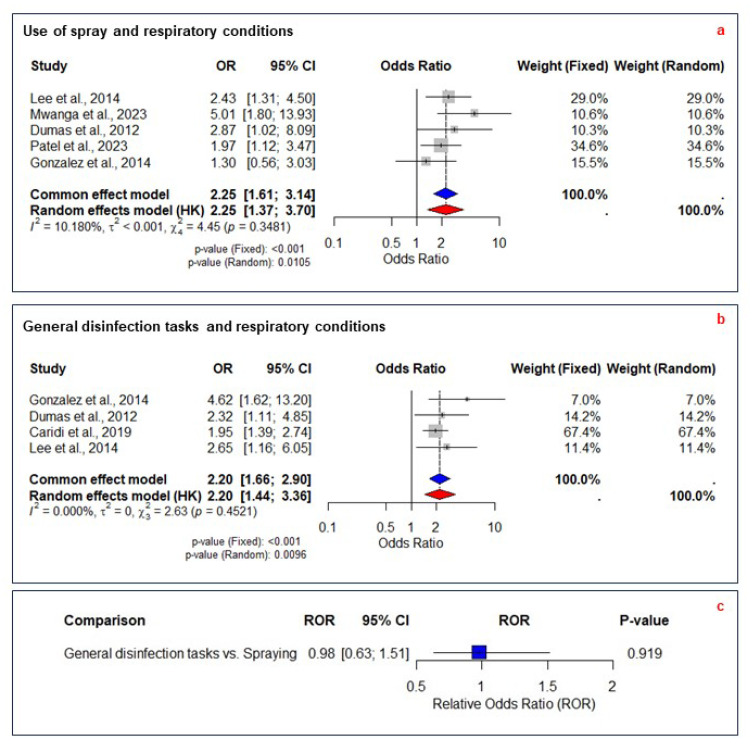 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfection Control and Ventilation · Infection Control in Healthcare · Occupational Health and Safety Research
1. Introduction
The Filoviridae family comprises two genera, Orthoebolavirus and Orthomarburgvirus, both of which have caused numerous outbreaks with high fatality rates over the past few decades [1]. Human-to-human transmission occurs through contact with an infected person’s body fluid. Infection prevention and control guidance from organizations like the U.S. Centers for Disease Control and Prevention and the World Health Organization (WHO) [2,3] used to recommend spraying 0.5% chlorine on surfaces and healthcare workers (HCWs) wearing personal protective equipment (PPE) who were in direct or indirect contact with the virus. Biocidal products used in healthcare settings undergo regulatory assessment prior to market authorization. Under EU Regulation No. 528/2012, this process includes the evaluation of toxicity and exposure to ensure that products do not present local or systemic health risks when used according to their approved conditions, including specified PPE and ventilation requirements.
However, over the last few years, the use of chlorine spraying has raised concerns about occupational health risks [4,5], prompting public health institutions to revise recommendations. WHO now bans direct spraying of HCWs and recommends chlorine wiping as the preferred disinfection method instead of spraying [6].
However, the systematic review supporting this decision found no evidence differentiating spraying from wiping in terms of efficacy or adverse health events. Consequently, the recommendation is primarily based on expert judgment and, as stated in the published guideline, on very low-certainty evidence [6]. Because wiping is labor-intensive and time-consuming, spraying remains a logistically attractive option [7], especially for HCWs in impermeable PPE working in hot, humid environments, where prolonged PPE use increases risks of heat stress and related injuries [8]. Additionally, the discomfort and decreased efficiency associated with PPE in high-temperature environments can pose health risks for staff [9].
Given the contrasting viewpoints and the limited evidence supporting changes to disinfection guidance, a systematic review was conducted to clarify the health risks associated with different disinfectants and application methods. Specifically, this review addresses two key research questions: (1) Are chlorine-based disinfectants more hazardous to HCWs than other types of disinfectants? (2) Does spraying disinfectants pose a greater risk to HCWs compared to other general disinfection tasks (GDTs) defined as all disinfection-related activities other than spraying, including wiping, mopping, disinfecting patient rooms, furniture surfaces, and equipment, as well as preparing and diluting products.
2. Materials and Methods
This systematic review followed the preferred reporting items for systematic reviews and meta-analysis (PRISMA-P) protocol [10]. The research protocol was registered a priori with the PROSPERO database (ID: CRD42023479363).
We searched PubMed, Scopus, and Embase on 15 November 2023 and updated the search on 2 March 2025 for full-text English articles without restricting the publication period. Additional studies were searched manually by examining the references of the included studies using ResearchRabbit^®^ [11]. The search strategy combined free-text and indexed terminology reflecting the eligibility criteria and was adapted for each database (Supplementary Materials, Table S1).
Eligibility criteria were based on the population (P), exposure (E), comparison (C), outcome (O), and study design (S) approach [12] as follows: P: HCWs exposed to chemical disinfectant products in occupational settings; E: occupational exposure to chlorine-based disinfectants or non-chlorine-based disinfectants; C: HCWs exposed to different disinfectants (chlorine-based versus non-chlorine-based), no disinfectants, or different application methods; O: occupational diseases or symptoms, such as respiratory conditions, respiratory symptoms, lung dysfunction, eye symptoms, skin symptoms, reproductive outcomes, and exposure markers; and S: case–control studies, cohort studies, cross-sectional studies, experimental studies, observational studies, case reports, and case series.
Qualitative studies, abstracts, conference papers, reviews, letters, and editorials were excluded. Full inclusion and exclusion criteria are detailed in Table S2 (Supplementary Materials).
2.1. Study Selection and Data Extraction
Two authors (LF and EC) independently screened titles, abstracts, and full texts against eligibility criteria. Data extraction was also conducted independently, with disagreements resolved through consultation with a third reviewer (GB or LS). Mendeley was used for reference management, and reasons for exclusion were recorded during the full-text review. A predesigned sheet (Supplementary Materials, Table S3) was used to extract and synthesize data on study characteristics, sample recruitment, exposure assessment, outcomes, and findings.
2.2. Risk of Bias and Quality of Evidence
Two authors (LF and EC) independently assessed the risk of bias (high, low, unclear) across eight domains using a validated occupational health tool [13,14,15]. Disagreements were resolved by discussion with a third reviewer (LS). The hybrid tool, incorporating elements from the Scottish Intercollegiate Guidelines Network [16] and Critical Appraisal Skills Program [17], is provided in Table S4 (Supplementary Materials).
2.3. Summary
This review primarily evaluates associations between occupational disinfectant exposure, including different application methods, and the incidence of occupational diseases.
2.4. Meta-Analysis
Studies were grouped by intervention: four groups for disinfectants (chlorine-based products; glutaraldehyde; peracetic acid [PAA], acetic acid [AA] and hydrogen peroxide [HP]; and quaternary ammonium compounds [QACs]), two groups for application methods (use of spray and GDTs), and one group for mitigation measures such as indoor ventilation and PPE which were included for completeness.
Health outcomes were clustered based on their relevance as respiratory, ocular-nasal, neurological, gastrointestinal, reproductive, immunological, and skin conditions (see “Outcome clustering” in Supplementary Materials). Meta-analysis was conducted when at least two primary studies with similar exposures and outcomes were available. When a study reported multiple outcomes, they were combined to create a single pairwise comparison [18] to avoid unit-of-analysis errors (see “Single pairwise comparison” in the Supplementary Materials).
The fixed-effects and random-effects models were used to generate pooled effect sizes. Higgins I^2^ statistic quantified the proportion of variability due to heterogeneity, while tau-squared (τ^2^) measured the between-study variance. Model selection was based on the I^2^ statistic, with significant heterogeneity defined as I^2^ ≥ 50% [19]. τ^2^ complemented this by contextualizing the variability in true intervention effects and informing the interpretation of random-effects models. Parameters were estimated using the Restricted Maximum Likelihood method with the metafor R package 4.3.2. [20]. Egger’s test and funnel plots were used to assess publication biases.
Meta-regression was conducted to examine the impact of study design and sample size on the observed heterogeneity. Residual heterogeneity was assessed, and the significance of the moderators was tested using the omnibus test for moderators (QM statistic) [21]. The R^2^ statistic quantified the proportion of heterogeneity explained by the model. Subgroup and sensitivity analyses were performed to explore potential sources of heterogeneity based on outcome type (e.g., asthma-related vs. nonspecific symptoms) and methodological differences and to evaluate their impact on overall results and heterogeneity. Subgroup analyses by disinfectant type and application method were pre-specified based on anticipated differences in exposure and toxicological profiles. Additional subgroup analyses, such as those based on outcome type, were exploratory and informed by observed heterogeneity. To address potential concerns of non-independence, evaluate the robustness, and determine the importance of individual studies on the overall meta-analysis results, a leave-one-out sensitivity analysis was conducted. To compare the risks associated with chlorine-based products to other disinfectants—and spraying to GDTs—the relative odds ratio (ROR) was calculated. Statistical analyses were performed using R version 4.3.2.
The certainty of evidence was assessed using the GRADE approach [22] across five domains: risk of bias, inconsistency, indirectness, imprecision, and publication bias. Conclusions were framed according to GRADE recommendations: terms such as “is”, “does”, “has”, or “will” for high-certainty evidence, “probably” or “likely” for moderate certainty, “may” or “the evidence suggests” for low certainty, and “very uncertain” for findings with very low certainty (see “GRADE” in the Supplementary Materials for more details).
3. Results
A total of 7154 articles were retrieved from the database search. After removing duplicates, 6729 articles remained for screening. Of these, 364 articles were eligible for full-text review. Ten full texts could not be retrieved and were excluded. After applying eligibility criteria, 29 studies were included (Figure 1). The data are synthesized in Table 1. Study categorization, quantitative data, and exclusion reasons are available in Supplementary Material Figure S1, Tables S5 and S6. Of the included studies, there were sixteen cross-sectional, six cohort, two case-control, two case series, two case reports, and one mixed-method experimental/observational study. Additionally, 6 studies had a low risk of bias, while 23 had a high risk (Supplementary Materials, Table S7). Most cross-sectional studies were deemed high risk due to their retrospective design, relying on self-reported surveys, which introduce potential biases related to outcome source and validation.
3.1. Chlorine-Based Products
Twelve studies examined the occupational health effects of chlorine-based product exposure (Table 1). Most were cross-sectional, with two cohort and one case–control study. The majority had a high risk of bias due to the retrospective design and reliance on self-reported exposure and outcome data, while three had a low risk. Dumas et al. [32] and Patel et al. [50] and Dumas et al. [29] reported a significant association between bleach exposure and poor asthma control [32], new asthma onset [50], and chronic obstructive pulmonary disease (COPD) [29]. Similarly, Su et al. categorized HCWs based on asthma symptoms and exposure to cleaning and disinfection activities, identifying a strong association between chlorine product use and undiagnosed/untreated asthma and asthma attacks/exacerbations [51]. However, earlier and later studies found no significant association between bleach exposure and new-onset asthma [28,30,37] or other respiratory conditions such as chest tightness and shortness of breath [35,47]. Mwanga et al. reported a significant association between bleach exposure exceeding 100 min per week and ocular–nasal symptoms, while no association was found with work-related asthma [44]. During the 2014–2016 Ebola outbreak, direct chlorine spraying on HCWs was common. Mehtar et al. found that multiple chlorine exposures were significantly associated with increased respiratory, eye, and skin conditions [5]. Similarly, Kobos et al. identified an association between bleach use and skin disorders or allergic reactions [39].
The meta-analysis was limited to respiratory conditions due to the availability of primary studies with similar exposures and outcomes. The analysis on chlorine-based products included eight studies with 7123 participants, comparing exposed and non-exposed groups across 11 respiratory effects. Outcomes from Ndlela et al. and Su et al. were combined into a single pairwise comparison (Supplementary Materials, Table S8) [46,51]. Four studies were excluded [29,30,39,44], with the reasons detailed in Supplementary Materials, Table S9. The fixed-effect model estimated an OR of 1.71 (95% CI 1.41–2.08, p < 0.001), while the random-effects model yielded an OR of 1.75 (95% CI 1.34–2.29, p = 0.002), with low heterogeneity (I^2^ = 12.5%, τ^2^ = 0.03, p = 0.33) (Figure 2a). The symmetrical funnel plot and Egger’s test (p = 0.45) indicated no substantial publication bias (Supplementary Materials, Table S10). The meta-regression analysis showed a negative coefficient for cross-sectional study design, suggesting that studies with this design type reported a slightly lower effect estimate (Supplementary Materials, Table S11). Leave-one-out analysis confirmed the stability of the effect estimate, with ORs ranging from 1.59 to 1.84 in the fixed-effect model (Supplementary Materials, Table S12). The evidence was rated as moderate certainty (Table 2).
3.2. Glutaraldehyde
Ten studies examined the occupational health effects of glutaraldehyde exposure (Table 1). Most were cross-sectional, with three cohort studies, one case series, and one mixed-methods study. Six had a high risk of bias due to the retrospective design and reliance on self-reported exposure and outcome data, while four had a low risk. Three studies applied air sampling techniques and found that glutaraldehyde can cause adverse health effects even below occupational limits, particularly occupational asthma [32,34], COPD [29], skin and airway symptoms, and headaches [48]. Additionally, poor work practices appear to increase exposure risk [45]. However, other studies found no significant association between glutaraldehyde exposure and new-onset asthma [30,31,37,45,51]. While one study reported a significant association between glutaraldehyde exposure exceeding 100 min per week and work-related ocular–nasal symptoms, no association was found with work-related asthma [44].
Meta-analysis was limited to respiratory conditions due to the availability of primary studies with similar exposures and outcomes. The analysis on glutaraldehyde exposure included four studies with 6256 participants, comparing exposed and non-exposed groups across six respiratory effects. Mwanga et al. [44] reported outcomes for three exposure levels, which were combined into a single pairwise comparison (Supplementary Materials, Table S8). Six studies were excluded, with the reasons detailed in Supplementary Materials, Table S9. The fixed-effect model estimated an OR of 1.44 (95% CI 1.14–1.81, p < 0.01), while the random-effects model yielded an OR of 1.44 (95% CI 0.98–2.10, p = 0.57), with low heterogeneity (I^2^ = 3.93%, τ^2^ < 0.001, p = 0.37) (Figure 2b).
The symmetrical funnel plot and Egger’s test (p = 0.96) indicated no substantial publication bias (Supplementary Materials, Table S10). Meta-regression did not identify significant moderators (Supplementary Materials, Table S11). Leave-one-out analysis confirmed the stability of the effect estimate, with ORs ranging from 1.28 to 1.51 in the fixed-effect model (Supplementary Materials, Table S12). The evidence was rated as moderate certainty (Table 2).
3.3. Peracetic Acid, Acetic Acid, and Hydrogen Peroxide
Nine studies examined the occupational health effects of products containing PAA, AA, and HP (Table 1). Most were cross-sectional, with three cohort studies and one case report. Five had a high risk of bias, while four had a low risk. Two studies applied air sampling. Casey et al. reported a higher prevalence of watery eyes and over three times the rate of current asthma among workers in the highest exposure department despite HP and AA levels being below OSHA’s permissible exposure limits (PELs) [26].
Hawley et al. and Blackley et al. identified significant associations between disinfectant exposure and eye and airway symptoms, even at levels below occupational limits [24,38]. Kobos et al. found that HCWs using HP-based products were 2- to 6-fold more likely to report allergic reactions than those who did not [39]. Similarly, Dumas et al. [29] reported an increased risk of developing COPD for nurses exposed to HP [29]. However, other studies found no significant association between HP and asthma incidence [30,31,32] or respiratory issues related to PAA [49]. Meta-analysis was not conducted due to the lack of comparable primary studies.
3.4. Quaternary Ammonium Compounds
Nine studies examined the occupational health effects of QAC exposure (Table 1). Most were cross-sectional, with two cohort studies. Six had a high risk of bias due to the retrospective design and reliance on self-reported data, while three had a low risk. Gonzalez et al. reported a significant association between QAC exposure and asthma and nasal symptoms among HCWs [37]. Patel et al. [50] and Dumas et al. [29] also found a significant association between QAC exposure and new-onset asthma [50] and COPD [29]. Ndlela and Naidoo reported an increased risk of respiratory issues, particularly shortness of breath [46]. Conversely, other studies found no significant association between QAC exposure and respiratory symptoms [30,32,45,52]. Kobos et al. identified a significant increase in skin disorders and allergic reactions among QAC users [39].
The meta-analysis was limited to respiratory conditions due to the availability of primary studies with similar exposures and outcomes. The analysis included five studies with 9270 participants, comparing exposed and non-exposed groups across nine respiratory effects. Ndlela et al. and Su et al. reported multiple outcomes, which were combined into a single pairwise comparison (Supplementary Materials, Table S8) [46,51]. Four studies were excluded, with the reasons detailed in Supplementary Materials, Table S9. The fixed-effect model estimated an OR of 1.30 (95% CI 1.06–1.60, p = 0.01), while the random-effects model yielded an OR of 1.39 (95% CI 0.69–2.78, p = 0.259), with significant heterogeneity (I^2^ = 63.2%, τ^2^ = 0.099, p = 0.03) (Figure 2c). The symmetrical funnel plot and Egger’s test (p = 0.29) indicated no substantial publication bias (Supplementary Materials, Table S10). Meta-regression did not identify significant moderators (Supplementary Materials, Table S11). Leave-one-out analysis confirmed that the effect estimate remained stable (fixed-effect model OR 1.22–1.44), except when Patel et al. [50] (p = 0.08) and Dumas et al. [32] (p = 0.09) were omitted (Supplementary Materials, Table S12). The evidence was rated as very low certainty due to the risk of bias, significant heterogeneity, and wide confidence intervals crossing the null value (Table 2).
3.5. Other Disinfectants
Six studies evaluated the occupational health risks from exposure to other disinfectants. Mwanga et al. reported a 4-fold increase in ocular–nasal symptoms with frequent use of alcohol-based products (OR 4.56), with similar risks for orthophthalaldehyde (OR 3.40), enzymatic cleaners (OR 2.57), and chlorhexidine (OR 1.84) [44]. Su et al. identified asthma risks associated with high-level disinfectants, alcohols, enzymes, formaldehyde, detergents, glass cleaners, and phenolic products [51]. Laborde-Castérot et al. linked aerosolized EDTA to respiratory conditions, with 10 of 28 patients showing positive nasal provocation tests [41]. Mac Hovcová et al. found disinfectants to be the most common chemical agents causing allergic skin diseases, though specific products were not identified [43]. Similarly, Nettis et al. identified disinfectant components as major triggers of occupational allergic contact dermatitis [47].
3.6. Relative Odds Ratios for Disinfectants
We assessed the RORs of respiratory conditions associated with different disinfectants, using chlorine-based products as the reference. The RORs were derived from ORs previously calculated against the non-exposed group. The ROR for glutaraldehyde relative to chlorine-based products was 0.84 (95% CI 0.62–1.14, p = 0.26), while for QACs, it was 0.81 (95% CI 0.39–1.68, p = 0.57) (Figure 2d). Both RORs were rated as low certainty due to the risk of bias and imprecision in pooled ORs (Table 2).
3.7. Application Methods
Eight studies assessed the occupational health risks associated with spray use and general disinfection tasks (Table 1). All were cross-sectional. Six had a high risk of bias, while two had a low risk. Lee et al. found that medium spray exposure (0.5–2 h/day with PPE) was significantly associated with respiratory conditions, while high exposure (>2 h/day without PPE) was not. High-exposure spraying was linked to chemical-related symptoms. Other application methods, such as mopping and wiping, were not significantly associated with respiratory or chemical-related symptoms at medium and high exposure levels. A variety of cleaners, degreasers, finishers, sealers, and polishes were used in the study setting [42]. Caridi et al. reported that cleaning and disinfecting fixed surfaces was significantly associated with current asthma, moderate exacerbation, and bronchial hyper-responsiveness [25]. Kurth et al. reported a significant association between cleaning/disinfection tasks and asthma or asthma-like symptoms [40]. Mwanga et al. reported that spray use, compared to wiping, was associated with nearly 5-fold higher odds of having a higher asthma symptom score. Manual sterilization and disinfection of medical instruments were associated with work-related ocular–nasal symptoms, though no details on specific disinfectants were provided [44]. Dumas et al. [28] found significant associations between moderate-to-high exposure (at least once a week) to GDTs and spray use with current asthma [28]. Mehtar et al. found that multiple versus single exposure to chlorine spray was associated with an increase in respiratory, eyes, and skin conditions [5]. Gonzalez et al. found that new-onset asthma among HCWs was significantly associated with GDTs and disinfectant dilution but not spray use [37]. Conversely, Patel et al. found that the use of spray for surface disinfection was significantly associated with new asthma onset [50].
Meta-analysis was limited to respiratory conditions due to the availability of primary studies with similar exposures and outcomes. The meta-analysis on spray use and respiratory conditions included five studies with 4568 individuals, comparing exposed and non-exposed groups across six adverse respiratory effects. Lee [42] reported separate health outcomes for medium and high exposure, which were combined into a single pairwise comparison (Supplementary Materials, Table S8). Mehtar’s [5] study was excluded, with the reasons detailed in Supplementary Materials, Table S9. The fixed-effects model estimated an OR of 2.25 (95% CI 1.61–3.14, p < 0.01), while the random-effects model yielded an OR of 2.25 (95 %CI 1.37–3.70, p = 0.010), with low heterogeneity (I^2^ = 10.18%, τ^2^ < 0.001, p = 0.35) (Figure 3a). Although the funnel plot showed some asymmetry, Egger’s test (p = 0.48) indicated no statistically significant publication bias (Supplementary Materials, Table S10). Meta-regression identified no significant moderators (Supplementary Materials, Table S11). Leave-one-out analysis confirmed stability, with ORs ranging from 2.05 to 2.49 in the fixed-effect model (Supplementary Materials, Table S12). The evidence was rated as moderate certainty, with minimal heterogeneity and stable estimates confirmed through sensitivity analyses (Table 2).
The meta-analysis on general disinfection tasks and respiratory conditions included four studies with 3480 individuals, comparing exposed and non-exposed groups across eight adverse respiratory effects.
Gonzalez, Caridi, and Lee [25,37,42], reported multiple outcomes, which were combined into a single pairwise comparison (Supplementary Materials, Table S8). Kurth [42] study was excluded, with the reasons detailed in Supplementary Materials, Table S9. The fixed-effect model estimated an OR of 2.20 (95% CI 1.66–2.90, p < 0.01), while the random-effects model yielded an OR of 2.20 (95% CI 1.44–3.36, p = 0.009), with no heterogeneity (I^2^ = 0%, τ^2^ = 0, p = 0.45) (Figure 3b).
Although the funnel plot showed some asymmetry, Egger’s test (p = 0.09) indicated no statistically significant publication bias. Meta-regression identified no significant moderators (Supplementary Materials, Table S11). Leave-one-out analysis confirmed stability, with ORs ranging from 2.08 to 2.82 in the fixed-effect model (Supplementary Materials, Table S12). The evidence was rated as moderate certainty, with no heterogeneity and consistent results confirmed across analyses (Table 2).
3.8. Relative Odds Ratios for Application Methods
We assessed the ROR of respiratory conditions associated with general disinfection tasks, using spray exposure as the reference. The ROR was 0.98 (95% CI 0.63–1.51, p = 0.9) (Figure 3c). The certainty of evidence was rated as low due to bias and imprecision in the pooled ORs.
3.9. Mitigation Measures
Five studies evaluated the effects of indoor ventilation on disinfectant exposure. Chang et al. found that adjusting air changes per hour (ACH) from 4 to 12–19 kept aerosolized chlorine dioxide levels below occupational limits, indicating minimal risk in ventilated rooms [27]. Norbäck reported that properly maintained ventilation maintained glutaraldehyde levels below Swedish limits, while poorly ventilated areas exceeded them, though specific ventilation rates were not provided [48]. Lee et al. found that continuous or frequent ventilation reduced the likelihood of respiratory or neurological symptoms in HCWs (OR 0.77, p < 0.05) [42]. Nayebzadeh et al. found no correlation between ACH and glutaraldehyde levels, suggesting that general ventilation alone was insufficient during solution changeover [45]. Estrin et al. assessed the concentration of ethylene oxide in the breathing zone of HCWs and concluded that it can cause neurological dysfunctions at low concentrations [33]. Multiple studies considered the use of PPE [39,42,44], but only one quantified the impact. Gaskins et al. assessed the impact of HLDs on fecundity in 1739 female nurses. HLD-exposed nurses using no PPE, one type of PPE, or two or more types of PPE experienced conception delays of 18%, 16%, and 0%, respectively. PPE use ranged from 9% for respiratory protection to 69% for gloves, suggesting that PPE can mitigate the reproductive risks of HLD exposure, though the composition of HLDs was not specified [36].
Certainty of evidence was assessed across five domains: risk of bias, inconsistency, indirectness, imprecision, and publication bias. Evidence was downgraded for high risk of bias, significant heterogeneity (I^2^ ≥ 50%), lack of alignment with the population, exposures, or outcomes of interest, wide confidence intervals crossing the null value, and evidence of publication bias from funnel plot asymmetry or Egger’s test. Certainty was classified as high, moderate, low, or very low based on the strength of evidence and identified limitations. For relative odds ratios, certainty was influenced by the quality and precision of pooled estimates, with downgrades applied when CIs included both harm and benefit.
4. Discussion
This systematic review and meta-analysis assessed the occupational health risks associated with exposure to various disinfectants and application methods among HCWs.
4.1. Disinfectants
Consistent with previous findings [52], the meta-analysis indicates that exposure to chlorine-based disinfectants likely increases the odds of developing respiratory conditions by 71% compared to non-exposed groups. No publication bias was detected, and leave-one-out analysis supported the stability of the results. Moreover, the evidence was assessed as moderate certainty. This underscores the importance of heightened precautions during outbreak responses, when the use of chlorine-based products is likely to increase. Additionally, the systematic review identifies non-respiratory health effects, including skin disorders, eye conditions, and allergic reactions, emphasizing the importance of comprehensive protective measures in occupational settings.
The meta-analysis shows that exposure to glutaraldehyde is likely to result in a 44% increase in the odds of developing respiratory conditions compared to non-exposed groups. This moderate-certainty evidence reflects reasonably strong confidence in the association despite some variability in study methodologies. Several studies support this finding: Gannon et al. reported occupational asthma at glutaraldehyde levels well below current exposure limits [34], and Dumas et al. [32] linked glutaraldehyde exposure to suboptimal asthma control [32]; this study contributed the largest weight in the meta-analysis due to its substantially larger sample size. Conversely, Gonzalez et al. [37] and later studies by Dumas et al. (2020, 2021) found no association with asthma incidence [30,31]. These results partially confirm previous findings [53], underscoring the need for further research. Beyond respiratory effects, studies also report associations with skin symptoms, headaches, and ocular–nasal irritation, highlighting broader health risks.
Due to the lack of primary studies with comparable exposures and outcomes, a meta-analysis was not conducted for peracetic acid, acetic acid, and hydrogen peroxide. Individual studies reported mixed findings. Casey et al. observed higher rates of watery eyes and current asthma among workers with the highest exposure levels to these chemicals [26]. Other studies, such as those by Otterspoor and Farrell, found no significant increases in respiratory issues or IgE levels [49]. This variability highlights the need for further research.
Exposure to QACs appears to increase the odds of developing respiratory conditions by 39% compared to non-exposed groups, but the evidence is very uncertain. High heterogeneity and wide confidence intervals further reduce the reliability of this pooled estimate. High heterogeneity likely reflects variability in effect sizes, study contexts, and outcome definitions. Subgroup analysis by outcome type (asthma-related vs. nonspecific symptoms) increased I^2^, indicating that outcome definitions alone do not fully explain the observed heterogeneity.
Sensitivity analysis revealed that excluding [37]—an outlier with a very high OR and wide confidence interval (7.56; 95% CI 1.84–31.05)—reduced heterogeneity to I^2^ = 36.3%. Even after omitting [37] the pooled OR for developing respiratory conditions remained significant at 1.25 (95% CI 1.01–1.55, p = 0.03), confirming the robustness of the meta-analysis results. The extreme effect size reported by [37] may reflect its unique study design, including a detailed occupational exposure assessment, small sample size, and a focus on high-risk tasks such as manual mixing of concentrated disinfectants. These factors likely amplify the observed association compared to studies relying solely on self-reported exposures or assessing broader healthcare populations. This combination of methodological and contextual differences likely explains the study’s disproportionate influence on heterogeneity. Individual studies presented mixed results. Gonzalez et al. found a significant risk of asthma associated with QACs [37], whereas Dumas et al. (2017, 2020) found no significant association with suboptimal asthma control or asthma incidence [30,32]. Kobos et al. reported an increased risk of skin disorders and allergic reactions [39], and Ndlela and Naidoo linked QAC exposure to respiratory issues [46]. These results highlight variability in study outcomes and underscore the need for further research.
The ROR for glutaraldehyde and QACs compared to chlorine-based products suggests 16% and 19% lower odds of developing respiratory conditions, respectively. However, the low certainty of evidence and the confidence intervals crossing the null value limit confidence in these findings, preventing firm conclusions.
4.2. Application Methods
The meta-analysis showed that spraying likely increases the odds of developing respiratory conditions by 125% (OR 2.25) compared to non-exposed groups, while general disinfection tasks likely increase the risk by 120% (OR 2.20). The ROR comparing GDTs to spraying suggests no significant difference in respiratory risk between application methods, but this finding is based on low-certainty evidence. This finding challenges the rationale for preferring wiping over spraying, suggesting that the focus should shift from prohibiting specific methods to improving overall safety measures. Enhancing ventilation, ensuring consistent PPE use, and selecting less hazardous disinfectants are likely to be more effective in reducing respiratory risks than banning spraying alone. The low certainty of evidence highlights some limitations, underscoring the need for more robust studies to clarify the relative risks of different disinfection methods.
Although respiratory symptoms were the most frequently reported adverse effects, few studies conducted air sampling to quantify exposure levels, complicating the interpretation of associations between disinfectant use and respiratory health outcomes. While a meta-analysis was not feasible, all studies consistently concluded that ventilation reduces airborne chemical concentrations, mitigating health risks. A similar protective effect is suggested for PPE use.
Limitations include the exclusion of non-English studies and potential misclassification of exposures and outcomes. Not all studies controlled for the same confounders, although low heterogeneity justified the use of a fixed-effects model. Underreporting of skin and ocular conditions limited broader assessment of disinfectant-related risks. Variations in exposure assessment and missing disinfectant concentration data complicated comparisons. Inconsistent reporting on disinfectants, ventilation, and PPE limited the attribution of health effects to specific chemicals, protective measures, or application methods. Moreover, very few studies provided both stratified exposure levels and clearly defined health outcomes, nor did they consistently describe whether biocidal products were used in accordance with manufacturers’ recommendations or regulatory guidelines. Detailed reporting on the use of PPE and risk mitigation measures was also lacking, which limits the ability to determine whether observed health effects reflect misuse or whether current guidance is insufficient to prevent harm. Respiratory outcomes were pooled across both nonspecific symptoms (e.g., cough) and clinically diagnosed conditions (e.g., asthma), which may limit the specificity of the effect estimates.
Recall bias remains a concern, given the retrospective design of most studies and the distinctive odors of disinfectants. The cross-sectional design of most studies limits causal inference between disinfectant exposure and respiratory outcomes. Nonetheless, the statistical significance of findings and consistency with prior research reinforce that disinfectant exposure, regardless of application method, poses an occupational health risk.
The increased risks associated with chlorine-based disinfectants compared to glutaraldehyde and QACs underscore the need for safer alternatives. Emerging evidence suggests that methylene blue may be an effective, less hazardous option, warranting further research [54,55]. The comparable risks between spraying and general disinfection tasks highlight the necessity of mitigation measures regardless of application method. These measures should include appropriate PPE, improved ventilation, and worker training on safe disinfection practices to minimize exposure.
Further prospective cohort studies with precise quantitative exposure and outcome assessments, including air sampling, are needed to clarify causal agents, environmental mechanisms, and how factors such as exposure duration, disinfectant concentration, PPE use, and ventilation contribute to risk variation.
5. Conclusions
This systematic review indicates that occupational exposure to chlorine-based products, glutaraldehyde, and QACs is associated with an increased risk of respiratory conditions compared to non-exposed groups. Among these, chlorine-based products likely pose the highest risk, supported by moderate-certainty evidence. Glutaraldehyde also likely increases the risk, with moderate-certainty evidence, despite some variability in study methodologies. In contrast, the evidence for QACs remains very uncertain due to high heterogeneity and limited data. Relative comparisons between disinfectants did not reveal statistically significant differences in respiratory risk; however, these findings are based on low-certainty evidence and should be interpreted with caution.
Both spraying and general disinfection tasks likely increase respiratory risk, supported by moderate-certainty evidence. Their relative comparison suggests nearly equal odds, though it is based on low-certainty evidence. These findings suggest that a blanket ban on spraying may not be justified. Instead, this review underscores the need for safer disinfectant alternatives and robust mitigation measures, including adequate ventilation, appropriate PPE, and strict adherence to safety protocols.
Efforts should prioritize replacing high-risk disinfectants with less hazardous alternatives whenever possible, especially in settings with poor ventilation. Respiratory protection must be ensured and correctly used in high-exposure procedures such as spraying. Regular assessment and improvement of ventilation systems are also critical. In parallel, comprehensive training and strict enforcement of safety protocols are essential to ensure safe handling and effective risk reduction.
Further research, particularly prospective cohort studies with quantitative exposure assessments, is needed to clarify the causal relationships between disinfectant exposure, application methods, and respiratory health outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1International Committee on Taxonomy of Viruses (ICTV) The ICTV Report on Virus Classification and Taxon Nomenclature. Genus: Orthoebolavirus 2024 Available online: https://ictv.global/report/chapter/filoviridae/filoviridae/orthoebolavirus(accessed on 12 April 2024)
- 2World Health Organization, Centers for Disease Control and Prevention Infection Control for Viral Haemorrhagic Fevers in the African Health Care Setting. Public Health Service 1998 Available online: https://iris.who.int/handle/10665/65012(accessed on 2 March 2019)
- 3World Health Organization Ebola Guidance Package Infection Prevention and Control (IPC) Guidance Summary Background 2014 Available online: https://iris.who.int/handle/10665/131828(accessed on 4 March 2019)
- 4Carpenter A. Cox A.T. Marion D. Phillips A. Ewington I. A case of a chlorine inhalation injury in an Ebola treatment unit J. R. Army Med. Corps 201616222923110.1136/jramc-2015-00050126472120 · doi ↗ · pubmed ↗
- 5Mehtar S. Bulabula A.N.H. Nyandemoh H. Jambawai S. Deliberate exposure of humans to chlorine-the aftermath of Ebola in West Africa Antimicrob. Resist. Infect. Control 201654510.1186/s 13756-016-0144-127895903 PMC 5109677 · doi ↗ · pubmed ↗
- 6World Health Organization Infection Prevention and Control Guideline for Ebola and Marburg Disease 2023 Available online: https://www.who.int/publications/i/item/WHO-WPE-CRS-HCR-2023.1(accessed on 4 January 2024)
- 7Wiemken T.L. Powell W. Carrico R.M. Mattingly W.A. Kelley R.R. Furmanek S.P. Johnson D. Ramirez J.A. Disinfectant sprays versus wipes: Applications in behavioral health Am. J. Infect. Control 2016441698169910.1016/j.ajic.2016.05.02827590110 · doi ↗ · pubmed ↗
- 8Quinn T. Kim J.-H. Strauch A. Wu T. Powell J. Roberge R. Shaffer R. Coca A. Physiological Evaluation of Cooling Devices in Conjunction with Personal Protective Ensembles Recommended for Use in West Africa Disaster Med. Public Health Prep.20171157357910.1017/dmp.2016.20928303772 PMC 9903158 · doi ↗ · pubmed ↗