Causal Relationship Between Cerebrospinal Fluid Metabolites and Intervertebral Disc Disease: A Bidirectional Mendelian Randomization Study
Jiheng Xiao, Tianyi Xia, Xianglong Zhou, Xin Xing, Yanbin Zhu, Yingze Zhang, Liming Xiong

TL;DR
This study finds a causal link between cerebrospinal fluid metabolites and intervertebral disc disease using genetic data.
Contribution
The study provides new causal evidence using bidirectional Mendelian randomization to link cerebrospinal fluid metabolites with intervertebral disc degeneration.
Findings
11 cerebrospinal fluid metabolites increase the risk of intervertebral disc degeneration.
6 cerebrospinal fluid metabolites have a protective effect against intervertebral disc degeneration.
Reverse analysis shows IVDD also influences cerebrospinal fluid metabolite levels.
Abstract
Background: Intervertebral disc degeneration (IVDD) is caused by an imbalance between the catabolic and anabolic processes within intervertebral disc tissue. Several studies have suggested a potential association between cerebrospinal fluid metabolites (CFMs) and the development of IVDD. However, the existing evidence on the relationship between CFM and IVDD is limited and inconsistent. Methods: The data on 338 cerebrospinal fluid metabolites and intervertebral disc degeneration analyzed in this study were sourced from their respective genome-wide association studies (GWAS). MR analysis employed single nucleotide polymorphisms (SNPs) closely associated with disease as instrumental variables (IVs). The inverse variance weighted (IVW) method was employed as the primary statistical approach, complemented by MR-Egger, the Weighted median, Simple mode, and the Weighted mode for result…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
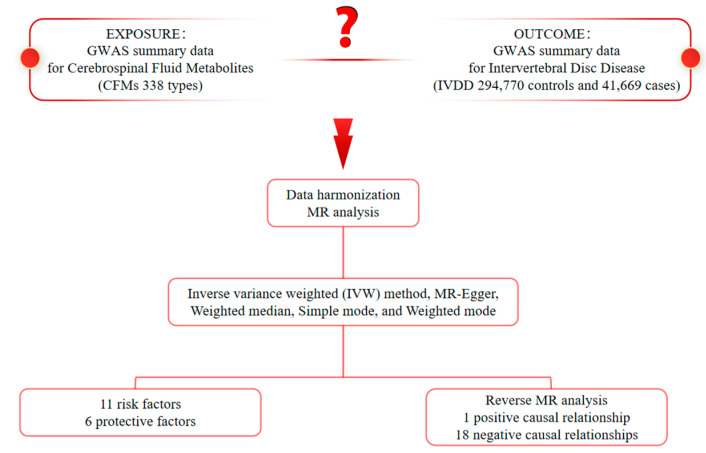 Figure 1
Figure 1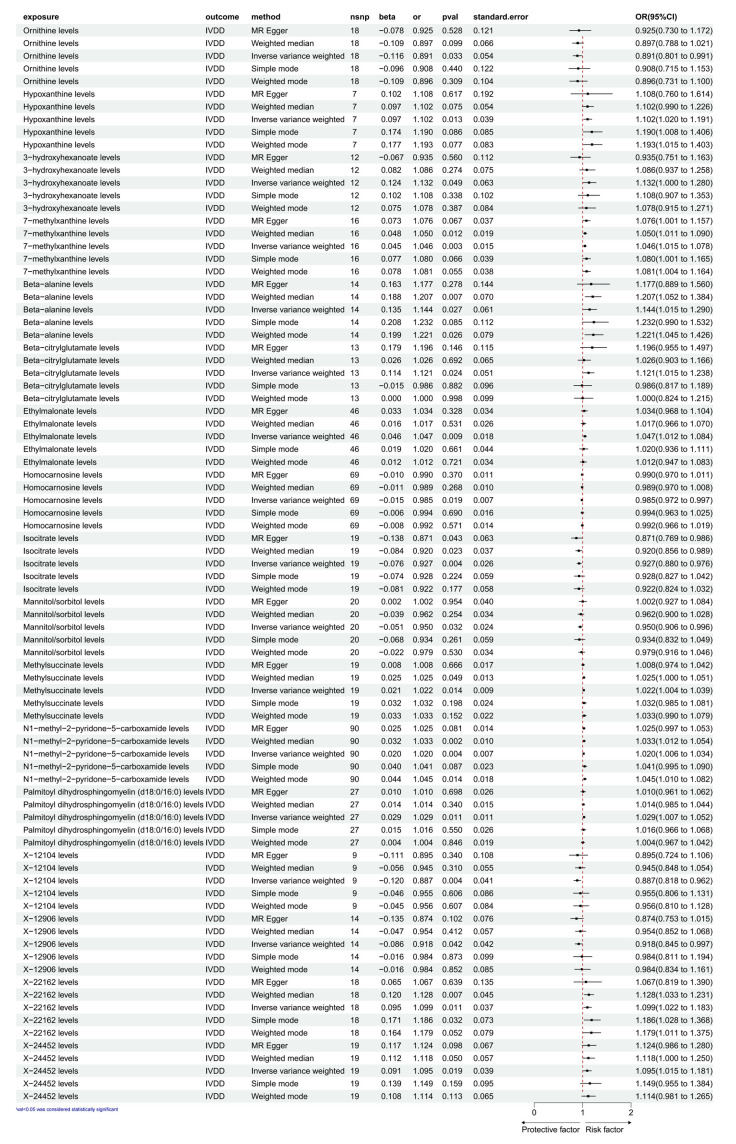 Figure 2
Figure 2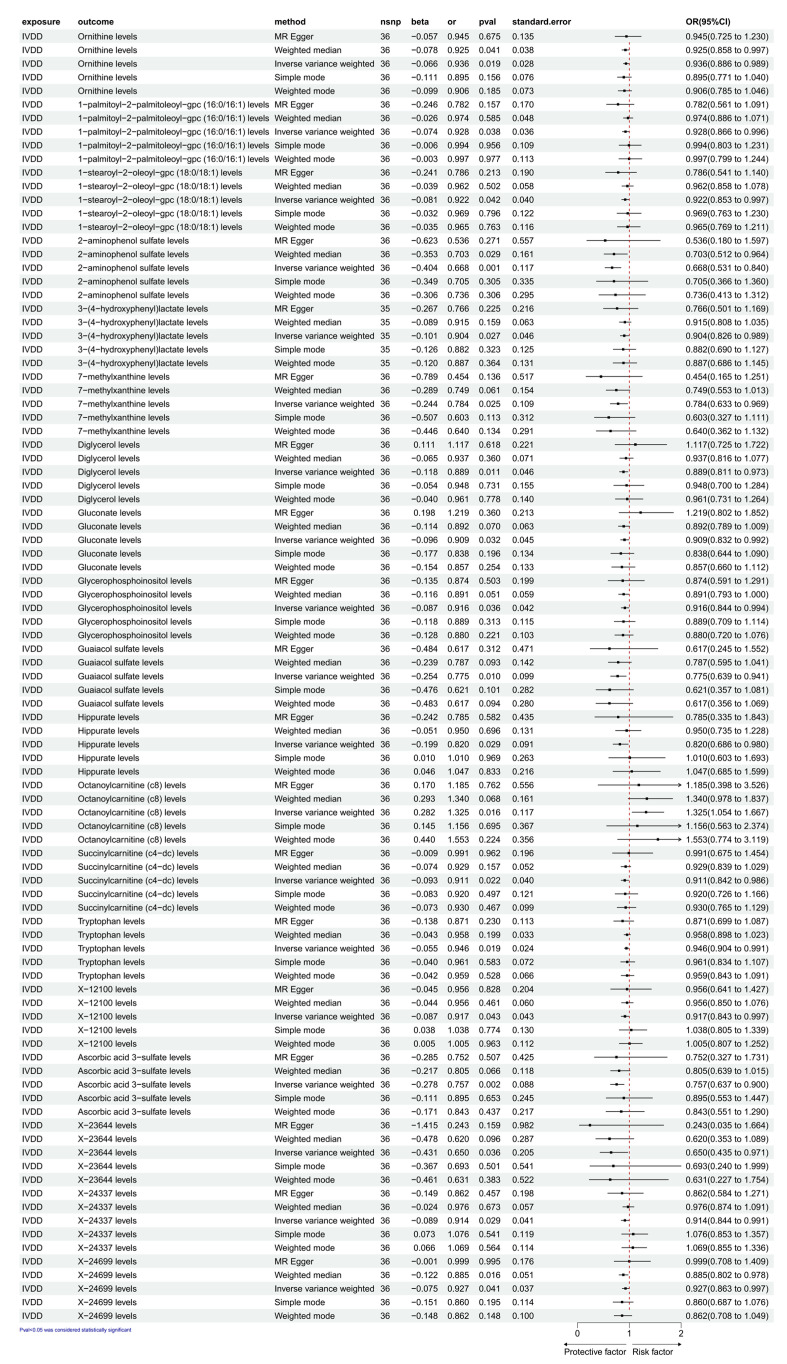 Figure 3
Figure 3- —Hygiene and Health Innovation Project of Major project assignment for research and development in Hebei province
- —Hubei Xianning Science and Technology Program Project
- —Integration Project of NSFC Joint Fund for Regional Innovation and Development
- —Key Projects of the National Natural Science Foundation of China
- —Huazhong University of Science and Technology 19th Batch of Graduate Student Innovation Fund Project
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpine and Intervertebral Disc Pathology · Musculoskeletal pain and rehabilitation · Spondyloarthritis Studies and Treatments
1. Introduction
Intervertebral disc degeneration (IVDD) is a common, age-associated condition stemming from metabolic disturbances, characterized by the progressive depletion of proteoglycans and water in the nucleus pulposus, potentially culminating in disc rupture among vertebrae [1,2]. Degenerated discs are more susceptible to herniation, which can impinge on spinal nerves and cause symptoms such as low-back pain and sciatica [3]. IVDD, although sometimes asymptomatic, is often associated with disc herniation, low back pain, and lumbar radiculopathy, particularly affecting the L4-S1 nerve roots [4]. This underscores the significance of understanding the pathogenesis and risk factors involved in IVDD for effective management and treatment strategies. Emerging evidence indicates a potential involvement of metabolomics disturbances in the pathogenesis of IVDD [5,6].
Early studies have indicated an association between abnormal metabolites and the subsequent development of IVDD [7,8,9]. Among various metabolites, cerebrospinal fluid (CSF) is often used by researchers to explore the interaction with the nervous system because of its unique physical and chemical properties [10]. For instance, Dong et al. derived principal components from 308 CSF metabolites and presented evidence of the association between CSF metabolites and Alzheimer’s disease biomarkers [11]. Recently, Panyard et al. conducted a metabolome-wide association study (MWAS) on 338 CSF metabolites, performing metabolome-wide and genome-wide association analyses, identifying 16 genotype-metabolite associations, testing them against 27 neurologic and psychiatric phenotypes, and discovering 19 significant CSF metabolite–phenotype associations, further confirming a potential close link between CSF and neurologic disorders [12]. However, there is currently no research exploring the mutual association between CSF and IVDD, possibly due to challenges in obtaining CSF and conducting metabolic studies. There is no definitive conclusion at the genetic level regarding a causal relationship between cerebrospinal fluid metabolites and intervertebral disc degeneration, which has led to inadequate academic attention being paid to this issue.
Mendelian randomization (MR) is a crucial analytical method for inferring etiology in epidemiological studies [13]. It is grounded in Mendel’s law of independent assortment [14]. MR employs genetic variation as an instrumental variable to evaluate the impact of risk factors on outcomes [15]. By maintaining a plausible causal sequence, MR effectively mitigates biases associated with confounding and reverse causality, distinguishing it from other statistical approaches [16]. Hence, this study used a dual-sample Mendelian randomization approach to analyze cerebrospinal fluid metabolites and osteoporosis samples, aiming to elucidate their causal relationship. This could connect cerebrospinal fluid metabolites to IVDD pathogenesis, offering novel insights into understanding and treating IVDD (Figure 1).
2. Materials and Methods
2.1. Study Design
Forward and reverse Mendelian randomization analyses were used to investigate the bidirectional causal effects of 338 cerebrospinal fluid and intervertebral disc degeneration. Three important assumptions need to be made when analyzing Mendelian randomization: (1) the assumption of correlation, meaning the assumption that there is a solid correlation between the instrumental variable (IVs) and the exposure factor; (2) the assumption of independence, assuming that the instrumental variable is independent of confounders; and (3) the assumption of exclusivity, claiming that the instrumental variable can only have an effect on the outcome through the exposure factor [17]. Exposure refers to the potential risk factors explored in the study or variables that may affect the outcome, which is strongly correlated with the instrumental variables. The outcome is the health outcome or disease state that is being looked at in the study and is the endpoint variable that the exposure may affect. In the article, single nucleotide polymorphisms (SNPs) associated with cerebrospinal fluid metabolite levels were used as instrumental variables to test whether these SNPs affect the risk of disc degeneration by altering metabolite levels. With this approach, Mendelian randomization analyses can help determine a causal relationship between exposure (cerebrospinal-fluid metabolite levels) and outcome (intervertebral disc degeneration) rather than a simple correlation. In addition, all data used in the analysis came from publicly available and previously published datasets, so no ethical approval or informed consent was required.
2.2. Genome-Wide Association Study (GWAS) Data Sources for IVDD
The GWAS data used in this study were obtained from the Integrative Epidemiology Unit (IEU) Open GWAS project, managed by the Medical Research Council (MRC) Integrative Epidemiology Unit at the University of Bristol. This initiative integrates and analyzes GWAS datasets from various sources, including the UK Biobank, peer-reviewed studies, and the FinnGen biobank. Published GWAS studies had passed ethical review at the time of study and all data used were publicly available, anonymized, and de-identified. Ethical approval from an institutional review board was not required for our study, as it adhered to standard ethical guidelines.
Summary-level data for intervertebral disc degeneration (IVDD) were sourced from the FinnGen database R10 (https://r10.finngen.fi/pheno/M13_INTERVERTEB, accessed on 6 December 2024), comprising 41,669 cases and 294,770 controls. The disease phenotype for IVDD was defined based on the International Classification of Diseases (ICD) coding system, including the Tenth (ICD-10), Ninth (ICD-9), and Eighth (ICD-8) editions. FinnGen’s phenotype library categorizes diseases according to the ICD-10, ICD-9, and ICD-8 codes, ensuring the reliability of the data for subsequent analyses. For this study, IVDD data were classified using the following ICD definitions: ICD-10 M51 refers to intervertebral disc disease of the thoracic, thoracolumbar, and lumbosacral spine; ICD-9 722 encompasses intervertebral disc disorders; and ICD-8 725 defines intervertebral disc displacement or slippage.
2.3. CFMs GWAS Data Sources
We utilized the most comprehensive and extensive collection of CFMs-related GWAS Catalog data (https://www.ebi.ac.uk/gwas/studies/GCST90025999, https://www.ebi.ac.uk/gwas/studies/GCST90026336, accessed on 6 December 2024). The study by Panyard DJ et al. measured cerebrospinal fluid metabolites in 689 participants, totaling 338 CFMs (PubMed ID: 33437055) [12].
2.4. Selection of Instrumental Variables (IVs)
To ensure compliance with the association hypothesis of Mendelian randomization analysis, (1) SNPs with a strong correlation with exposure were selected using a p < 5 × 10^−8^ threshold; (2) the threshold parameters were set (R^2^ = 0.001, kb = 10,000) to avoid the effect of chain disequilibrium; then, SNPs with allele frequencies less than 0.01 were excluded, and duplicates and palindromic SNPs were removed. (3) In order to reduce the bias caused by weak instrumental variables, the F statistic was chosen to assess the strength of association between instrumental variables and inflammatory proteins, calculated as F = [R^2^(N − 1 − K)]/[K × (1 − R^2^)], where R^2^ = β^2^ × 2 × MAF × (1 − MAF), and N denotes the sample size. SNPs with an F value lower than 10 were excluded to minimize the bias caused by the weak instrument; (4) SNPs associated with confounders and disc degeneration outcomes were manually screened and removed [18].
2.5. Statistical Analysis
All analyses were conducted using R 4.3.2 software. To investigate the causal relationship between candidate functional metabolites (CFMs) and intervertebral disc degeneration (IVDD), we employed several Mendelian Randomization (MR) methods, including the inverse variance weighted (IVW) method, the MR-Egger method, the weighted median (WM), and weighted mode approaches [19]. Among these, the primary method was IVW analysis, which assumes no intercept term in the regression model and utilizes outcome variance to provide reliable estimates, particularly in the absence of directed pleiotropy of instrumental variables (IVs) [20]. Heterogeneity across the selected IVs was assessed using Cochran’s Q statistic, with corresponding p-values. If the null hypothesis was rejected, we used the random-effects IVW model. To identify and exclude potential horizontal pleiotropic outliers that could significantly affect the results, we applied both the MR-Egger and MR-PRESSO methods [21,22]. Additionally, leave-one-out and scatter plots demonstrated that outliers had minimal influence on the results, underscoring the robustness and consistency of the findings, as well as the absence of significant heterogeneity in the correlations.
3. Results
3.1. Exploration of the Causal Effect of CFM on IVDD
As illustrated in Figure 2, based on the selection criteria for SNPs and the p values denoting significance, we identified 17 CFMs with causal relationships with IVDD. These SNPs could serve as IVs in the MR analysis. We employed IVW as the primary analytical method. The IVW analysis detected 11 CFMs as risk factors for IVDD. The specific MR results are as follows: hypoxanthine levels (OR, 1.132; 95% CI, 1.000 to 1.280; nsnp = 7; β = 0.097; p = 0.013; SE = 0.039); 3-hydroxyhexanoate levels (OR, 1.102; 95% CI, 1.020 to 1.191; nsnp = 12; β = 0.124; p = 0.049; SE = 0.063); 7-methylxanthine levels (OR, 1.046; 95% CI, 1.015 to 1.078; nsnp = 16; β = 0.045; p = 0.003; SE = 0.015); beta-alanine levels (OR, 1.144; 95% CI, 1.015 to 1.290; nsnp = 14; β = 0.135; p = 0.027; SE = 0.061); beta-citrylglutamate levels (OR, 1.121; 95% CI, 1.015 to 1.238; nsnp = 13; β = 0.114; p = 0.024; SE = 0.051); ethylmalonate levels (OR, 1.047; 95% CI, 1.012 to 1.084; nsnp = 46; β = 0.046; p = 0.009; SE = 0.018); methylsuccinate levels (OR, 1.022; 95% CI, 1.004 to 1.039; nsnp = 19; β = 0.021; p = 0.014; SE = 0.009); N1-methyl-2-pyridone-5-carboxamide levels (OR, 1.020; 95% CI, 1.006 to 1.034; nsnp = 90; β = 0.020; p = 0.004; SE = 0.007); palmitoyl dihydrosphingomyelin (d18:0/16:0) levels (OR, 1.029; 95% CI, 1.007 to 1.052; nsnp = 27; β = 0.029; p = 0.011; SE = 0.011); X-22162 levels (OR, 1.099; 95% CI, 1.022 to 1.183; nsnp = 18; β = 0.095; p = 0.011; SE = 0.037); and X-24452 levels (OR, 1.095; 95% CI, 1.015 to 1.181; nsnp = 19; β = 0.091; p = 0.019; SE = 0.039). Additionally, the IVW analysis identified six CFMs that serve as protective factors against IVDD: ornithine levels (OR, 0.891; 95% CI, 0.801 to 0.991; nsnp = 18; β = −0.116; p = 0.033; SE = 0.054); homocarnosine levels (OR, 0.985; 95% CI, 0.972 to 0.997; nsnp = 69; β = −0.015; p = 0.019; SE = 0.007); isocitrate levels (OR, 0.927; 95% CI, 0.880 to 0.976; nsnp = 19; β = −0.076; p = 0.004; SE = 0.026); mannitol/sorbitol levels (OR, 0.950; 95% CI, 0.906 to 0.996; nsnp = 20; β = −0.051; p = 0.032; SE = 0.024); X-12104 levels (OR, 0.887; 95% CI, 0.818 to 0.962; nsnp = 9; β = −0.120; p = 0.004; SE = 0.041); and X-12906 levels (OR, 0.918; 95% CI, 0.845 to 0.997; nsnp = 14; β = −0.086; p = 0.042; SE = 0.042). Pleiotropy analysis (Table 1) showed that the MR-Egger test function results for the 17 CFMs with IVDD had p values greater than 0.05, indicating no significant effects. Data visualization in Supplementary Figure S1A–K indicates a positive slope (greater than 0) for the overall SNP effect of exposure factors such as hypoxanthine, 3-hydroxyhexanoate, 7-methylxanthine, beta-alanine, beta-citrylglutamate, ethylmalonate, methylsuccinate, N1-methyl-2-pyridone-5-carboxamide, palmitoyl dihydrosphingomyelin (d18:0/16:0), X-22162, and X-24452 levels, suggesting an increase in the SNP effect of the outcome variable IVDD. Conversely, exposure factors such as ornithine, homocarnosine, isocitrate, mannitol/sorbitol, X-12104, and X-12906 levels show a negative slope (less than 0), indicating a decrease in the SNP effect of IVDD (Figure S1L–Q). When the SNP effect of exposure is zero, the outcome variable is also zero, supporting that our study is not influenced by horizontal pleiotropy. For heterogeneity detection, IVW analysis of the 17 CFMs with IVDD showed p > 0.05, suggesting no heterogeneity among SNPs. The funnel plot (Figure S2) appears roughly symmetrical, indicating minimal bias due to heterogeneity in this study. In the heterogeneity Q test (Table 2), the IVW method for the 17 CFMs and IVDD showed p > 0.05, indicating no heterogeneity among SNPs. Leave-one-out analyses showed similar IVW results with all SNPs included, identifying no SNPs significantly influencing the causal estimates (Figure S3).
3.2. Exploration of the Causal Effect of IVDD on CFM
As shown in Figure 3, with IVDD as the exposure factor, a total of 36 SNPs were strongly correlated and used as instrumental variables (IVs) for subsequent analysis. Based on significant p values, we detected a causal relationship between IVDD and 19 types of CFM. According to the IVW analysis results, we found that IVDD can cause the production of only one cerebrospinal fluid metabolite. The specific MR analysis results are as follows: octanoylcarnitine (c8) levels (OR, 1.325; 95% CI, 1.0541.667; nsnp = 36; β = 0.282; pval = 0.016; SE = 0.117). And then, we detected that IVDD might decrease the levels of 18 types of CFM: ornithine levels (OR, 0.936; 95% CI, 0.8860.989; nsnp = 36; β = −0.066; pval = 0.019; SE = 0.028); 1-palmitoyl-2-palmitoleoyl-gpc (16:0/16:1) levels (OR, 0.928; 95% CI, 0.8660.996; nsnp = 36; β = −0.074; pval = 0.038; SE = 0.036); 1-stearoyl-2-oleoyl-gpc (18:0/18:1) levels (OR, 0.922; 95% CI, 0.8530.997; nsnp = 36; β = −0.081; pval = 0.042; SE = 0.040); 2-aminophenol sulfate levels (OR, 0.668; 95% CI, 0.5310.840; nsnp = 36; β = −0.404; pval = 0.001; SE = 0.117); 3-(4-hydroxyphenyl) lactate levels (OR, 0.904; 95% CI, 0.8260.989; nsnp = 36; β = −0.101; pval = 0.027; SE = 0.046); 7-methylxanthine levels (OR, 0.784; 95% CI, 0.6330.969; nsnp = 36; β = −0.244; pval = 0.025; SE = 0.109); diglycerol levels (OR, 0.889; 95% CI, 0.8110.973; nsnp = 36; β = −0.118; pval = 0.011; SE = 0.046); gluconate levels (OR, 0.909; 95% CI, 0.8320.992; nsnp = 36; β = −0.096; pval = 0.032; SE = 0.045); glycerophosphoinositol levels (OR, 0.916; 95% CI, 0.8440.994; nsnp = 36; β = −0.087; pval = 0.036; SE = 0.042); guaiacol sulfate levels (OR, 0.775; 95% CI, 0.6390.941; nsnp = 36; β = −0.254; pval = 0.010; SE = 0.099); hippurate levels (OR, 0.820; 95% CI, 0.6860.980; nsnp = 36; β = −0.199; pval = 0.029; SE = 0.091); succinyl carnitine (c4-dc) levels (OR, 0.911; 95% CI, 0.8420.986; nsnp = 36; β = −0.093; pval = 0.022; SE = 0.040); tryptophan levels (OR, 0.946; 95% CI, 0.9040.991; nsnp = 36; β = −0.055; pval = 0.019; SE = 0.024); X-12100 levels (OR, 0.917; 95% CI, 0.8430.997; nsnp = 36; β = −0.087; pval = 0.043; SE = 0.043); ascorbic acid 3-sulfate levels (OR, 0.757; 95% CI, 0.6370.900; nsnp = 36; β = −0.278; pval = 0.002; SE = 0.088); X-23644 levels (OR, 0.650; 95% CI, 0.4350.971; nsnp = 36; β = −0.431; pval = 0.036; SE = 0.205); X-24337 levels (OR, 0.914; 95% CI, 0.8440.991; nsnp = 36; β = −0.089; pval = 0.029; SE = 0.041); and X-24699 levels (OR, 0.927; 95% CI, 0.863~0.997; nsnp = 36; β = −0.075; pval = 0.041; SE = 0.037). In the pleiotropy analysis (Table 3), the MR-Egger test function results for IVDD and the 19 types of CFM suggested that the p value was greater than 0.05. Data-visualization analysis indicated that under the IVW method, the overall SNP effect of the exposure factor IVDD increased, and the SNP effect of the outcome variable octanoylcarnitine (c8) levels also increased (slope greater than 0) (Figure S4A). In contrast, the overall SNP effect of the exposure factor IVDD increased, while the SNP effects of the outcome variables decreased, including ornithine levels; 1-palmitoyl-2-palmitoleoyl-gpc (16:0/16:1) levels; 1-stearoyl-2-oleoyl-gpc (18:0/18:1) levels; 2-aminophenol sulfate levels; 3-(4-hydroxyphenyl) lactate levels; 7-methylxanthine levels; diglycerol levels; gluconate levels; glycerophosphoinositol levels; guaiacol sulfate levels; hippurate levels; succinyl carnitine (c4-dc) levels; tryptophan levels; X-12100 levels; ascorbic acid 3-sulfate levels; X-23644 levels; X-24337 levels; and X-24699 levels (slope less than 0) (Figure S4B–S). These results suggest that this study is not affected by horizontal pleiotropy. In heterogeneity testing, the IVW p > 0.05 for IVDD and 19 types of CFM, suggesting no heterogeneity among the SNPs. The funnel plot showed an approximately symmetrical shape, indicating a low possibility of result bias due to heterogeneity in this study (Figure S5). In the heterogeneity Q test (Table 4) and after sequentially excluding SNPs using the leave-one-out method, the IVW analysis results for IVDD and 19 types of CFM were similar to those when all of the SNPs were included. No SNP with a significant impact on causal association estimates was found, indicating the stability of the causal associations shown in the analysis results (Figure S6).
4. Discussion
IVDD is a leading cause of low back pain and a common degenerative disease [23]. While IVDD’s exact etiology remains unclear, multiple factors contribute, including genetics, mechanical load, inflammation, nutrition, and aging [24,25,26]. Early IVDD research emphasized mechanical stress, nutrient deficits in annulus fibrosus/cartilaginous endplate, and nucleus pulposus degeneration [27]. Recent IVDD research has increasingly focused on ECM alterations, impaired MSC differentiation, and inflammatory dysregulation [28]. For example, during IVDD, the increased release of inflammatory factors such as TNF-α, IL1-β, interleukin (IL)-6, IL-8, and prostaglandin E2 (PGE2) is stimulated by high catabolic metabolism and low synthetic metabolism of ECM [29,30,31]. Likewise, a decreased nutrient supply leads to an acidic shift in the IVD microenvironment, further exacerbating ECM degradation and pro-inflammatory cytokine release [32]. Hence, the pathologic process of IVDD often includes inflammatory reactions in the intervertebral disc and surrounding tissues. Furthermore, studies have shown that during cellular senescence, cells cease proliferation while persistently releasing various inflammatory factors (including homocarnosine) and matrix metalloproteinases, thereby exacerbating intervertebral disc degeneration [33]. Activated inflammatory cells secrete cytokines, maintaining the inflammatory microenvironment. These inflammatory mediators can penetrate the blood–brain barrier (BBB) or the cerebrospinal fluid–spinal cord barrier, inducing alterations in specific metabolites within the cerebrospinal fluid.
CSF, a crucial part of the central nervous system (CNS), possesses distinct physiological properties that can impact the development and advancement of neurovascular diseases. CSF biochemically reflects CNS status and, given its spinal proximity, may influence or mirror adjacent pathology. Studies have demonstrated significant shifts in CSF metabolic profiles in degenerative and inflammatory diseases. For instance, Horvatić et al. [34] applied a multi-omics approach in canine disc herniation and observed distinct metabolic changes in CSF, implicating energy metabolism and amino-acid dysregulation in disc pathology. Studies by Kosek et al. report elevated levels of IL-8 in the CSF of patients with knee osteoarthritis [35], suggesting that there may be a strong association between certain cerebrospinal fluid components and other inflammatory responses throughout the body. Furthermore, research indicates that alterations in CSF components can lead to a reduction in the extracellular matrix in soft tissues, triggering degenerative changes and inflammatory reactions. For example, elevated levels of the CSF metabolite homocysteine lead to the accumulation of toxic free radicals at the BBB, thereby activating matrix metalloproteinases (MMPs) [36,37]. MMPs critically degrade ECM, with increased activity releasing collagen fragments and proteoglycans into CSF, altering its composition [38].
This research marks the first exploration of bidirectional causality between 338 CFMs and IVDD, employing Mendelian randomization with a broad, publicly accessible genetic dataset. Based on the results of MR analysis, we found that 11 metabolites, including hypoxanthine levels, were risk factors for IVDD, and 6 metabolites, including ornithine levels, were protective factors, suggesting that patients with high indicators of above 11 metabolites should be alerted to the risk of subsequent IVDD. Notably, elevated levels of hypoxanthine, a purine metabolism intermediate, were causally linked with increased IVDD risk. This aligns with previous research indicating that hypoxanthine accumulation contributes to oxidative stress and mitochondrial dysfunction, both of which are detrimental to disc cell viability [39]. Conversely, ornithine, a key component in the urea-cycle and tissue-regeneration pathways, exhibited a protective effect against IVDD in both forward and reverse MR analysis. This is consistent with the recent literature emphasizing ornithine’s role in anti-inflammatory responses and collagen synthesis, potentially aiding in ECM repair and maintaining disc integrity [40]. Our reverse MR analysis revealed that IVDD could lead to increased levels of octanoylcarnitine (C8) and decreased levels of 18 CFMs, including gluconate and glycerophosphoinositol. These changes may represent downstream metabolic responses secondary to chronic inflammation, altered vascular perfusion, and ECM catabolism within degenerated discs. For example, a decline in gluconate—a compound with osmoprotective and antioxidant roles—may reflect the oxidative microenvironment prevalent in IVDD [41]. Importantly, the metabolites identified in this study intersect key biological pathways, including the urea cycle, fatty acid oxidation, purine metabolism, and mitochondrial energy regulation—all of which have been previously implicated in disc degeneration and neuroinflammatory responses [42].
Our findings also emphasize the potential bidirectional relationship between systemic metabolism and localized spinal pathology. Prior metabolomics reveals that disc-related metabolic changes actively drive, rather than merely reflect, degeneration progression [43]. Collectively, this is the first MR-based study to explore the causal interplay between CFMs and IVDD across both directions. These insights underscore the need to further investigate CSF metabolite profiles, not only as biomarkers for early IVDD detection but also as potential therapeutic targets for halting or reversing disc degeneration. Therapeutic strategies aimed at modulating CFM levels, such as enhancing ornithine bioavailability or mitigating purine-related oxidative stress, could complement existing mechanical and surgical interventions. In light of these findings, future work should integrate longitudinal metabolomics, multi-tissue transcriptomics, and functional validation models to unravel the precise mechanistic links between CSF metabolites and intervertebral disc health.
5. Limitation
Despite the strengths of this bidirectional Mendelian randomization (MR) analysis, several limitations should be acknowledged. First, while our analysis identified several cerebrospinal fluid metabolites (CFMs) potentially causally associated with intervertebral disc degeneration (IVDD), the underlying biological mechanisms remain largely undefined. Their roles in disc-matrix homeostasis, inflammation, or cellular metabolism have not been fully elucidated and warrant further mechanistic investigation in vitro and in vivo. Second, a fundamental assumption of MR is that the selected genetic instruments are valid—i.e., strongly associated with the exposure, independent of confounders, and exerting effects on the outcome exclusively through exposure. While we employed stringent quality control and sensitivity analyses to mitigate bias, the possibility of horizontal pleiotropy and residual confounding cannot be entirely excluded. Third, MR estimates represent the lifelong effect of genetically proxied exposure. This time-invariant assumption may not adequately capture the dynamic nature of metabolite levels, which can fluctuate due to metabolic status, disease stage, or environmental influences. This physiological variability could obscure causal interpretations and introduce temporal mismatches. Fourth, the GWAS summary statistics used in this study were derived from the Finnish population, predominantly of European ancestry. Such ancestry homogeneity may limit the generalizability of our findings to more genetically diverse populations. Population stratification, although adjusted for using principal components, may still introduce subtle bias. Finally, IVDD phenotyping relied on ICD-10 diagnostic codes, which, although widely used in genetic epidemiology, may lack the granularity needed to distinguish clinical subtypes or disease severity. This potential for misclassification and phenotype heterogeneity could attenuate observed associations or introduce residual bias.
6. Conclusions
This study employed a bidirectional two-sample Mendelian randomization (MR) framework based on large-scale genome-wide association study (GWAS) summary data to investigate the potential causal effects between cerebrospinal fluid metabolites (CFMs) and intervertebral disc degeneration (IVDD). Our results provide genetic evidence supporting a causal link, identifying 11 CFMs that may increase susceptibility to IVDD and 6 CFMs with potential protective effects. The reverse MR analysis further demonstrated that IVDD itself can causally influence specific CFMs, with one metabolite positively and 18 metabolites negatively affected, suggesting the possibility of reverse metabolic alterations secondary to disc pathology. By integrating multiple robust MR methodologies, such as inverse variance weighting, the MR-Egger method, and the weighted median method, and by performing extensive sensitivity tests, we minimized the influence of confounding factors, reverse causality, and horizontal pleiotropy. These methodological strengths enhance the reliability of our causal inferences and provide a foundation for future mechanistic exploration. The findings not only expand the current understanding of IVDD pathogenesis from a metabolic perspective but also highlight CFMs as potential biomarkers or targets for early diagnosis and therapeutic intervention. Overall, this study offers novel insights into the metabolic contributions to IVDD. Further research incorporating functional validation, longitudinal metabolic profiling, and systems biology approaches will be essential to clarify the underlying molecular mechanisms and assess clinical applicability.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Buchbinder R. van Tulder M. Öberg B. Costa L.M. Woolf A. Schoene M. Croft P. Lancet Low Back Pain Series Working Group Low back pain: A call for action Lancet 20183912384238810.1016/S 0140-6736(18)30488-429573871 · doi ↗ · pubmed ↗
- 2Ropper A.H. Zafonte R.D. Sciatica N. Engl. J. Med.20153721240124810.1056/NEJ Mra 141015125806916 · doi ↗ · pubmed ↗
- 3Kague E. Turci F. Newman E. Yang Y. Brown K.R. Aglan M.S. Otaify G.A. Temtamy S.A. Ruiz-Perez V.L. Cross S. 3D assessment of intervertebral disc degeneration in zebrafish identifies changes in bone density that prime disc disease Bone Res.202193910.1038/s 41413-021-00156-y 34465741 PMC 8408153 · doi ↗ · pubmed ↗
- 4Risbud M.V. Shapiro I.M. Role of cytokines in intervertebral disc degeneration: Pain and disc content Nat. Rev. Rheumatol.201410445610.1038/nrrheum.2013.16024166242 PMC 4151534 · doi ↗ · pubmed ↗
- 5Wu J. Chen Y. Liao Z. Liu H. Zhang S. Zhong D. Qiu X. Chen T. Su D. Ke X. Self-amplifying loop of NF-κB and periostin initiated by PIEZO 1 accelerates mechano-induced senescence of nucleus pulposus cells and intervertebral disc degeneration Mol. Ther.2022303241325610.1016/j.ymthe.2022.05.02135619555 PMC 9552911 · doi ↗ · pubmed ↗
- 6Ma K. Chen S. Li Z. Deng X. Huang D. Xiong L. Shao Z. Mechanisms of endogenous repair failure during intervertebral disc degeneration Osteoarthr. Cartil.201927414810.1016/j.joca.2018.08.02130243946 · doi ↗ · pubmed ↗
- 7Ji L. Wang Y. Lu T. Yang J. Luo C. Qiu B. Identification of blood metabolites linked to the risk of intervertebral disc diseases: A comprehensive Mendelian randomization study Postgrad. Med. J.2023991148115310.1093/postmj/qgad 05237399049 · doi ↗ · pubmed ↗
- 8Luo Z. Wei Z. Zhang G. Chen H. Li L. Kang X. Achilles’ Heel-The Significance of Maintaining Microenvironmental Homeostasis in the Nucleus Pulposus for Intervertebral Discs Int. J. Mol. Sci.2023241659210.3390/ijms 24231659238068915 PMC 10706299 · doi ↗ · pubmed ↗