Pediatric Heterotopic Gastric Mucosa of the Cervical Esophagus (Inlet Patch): Case Series with Clinical, Endoscopic, and Histopathological Correlation
Javier Arredondo Montero, Samuel Sáez Álvarez, Andrea Herreras Martínez, Ana Fernández-García, Cristina Iglesias Blázquez

TL;DR
This study examines a rare condition called inlet patch in children, finding that it is often asymptomatic but can cause symptoms related to inflammation and H. pylori infection.
Contribution
The study provides a detailed clinical, endoscopic, and histopathological analysis of pediatric inlet patch cases, identifying a potential link with H. pylori and gastritis.
Findings
Endoscopic examination revealed characteristic salmon-red plaques in all patients with inlet patch.
A potential association was found between IP inflammation severity, gastritis severity, and H. pylori presence.
Symptoms improved in all cases with proton pump inhibitors, suggesting a therapeutic benefit.
Abstract
Introduction: Inlet patch (IP) is a congenital anomaly characterized by gastric heterotopia in the cervical esophagus. While extensively described in adults, it remains poorl characterized in pediatric populations. Material and Methods: This retrospective, single-center study included all pediatric patients (0–14 years) diagnosed with IP between 2018 and 2025. Sociodemographic and clinical data were collected. A blinded pathologist assessed the presence and severity of inflammation within the IP. Results: Nine patients (median age, 12 years; range, 6–14 years) were included, with 78% beingmale. Cervical esophageal symptoms were identified in 67%, primarily dysphagia and gastroesophageal reflux disease-related complaints, although concomitant conditions such as eosinophilic esophagitis were frequently present. Three patients had symptoms potentially attributable to IP (33%). Endoscopic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
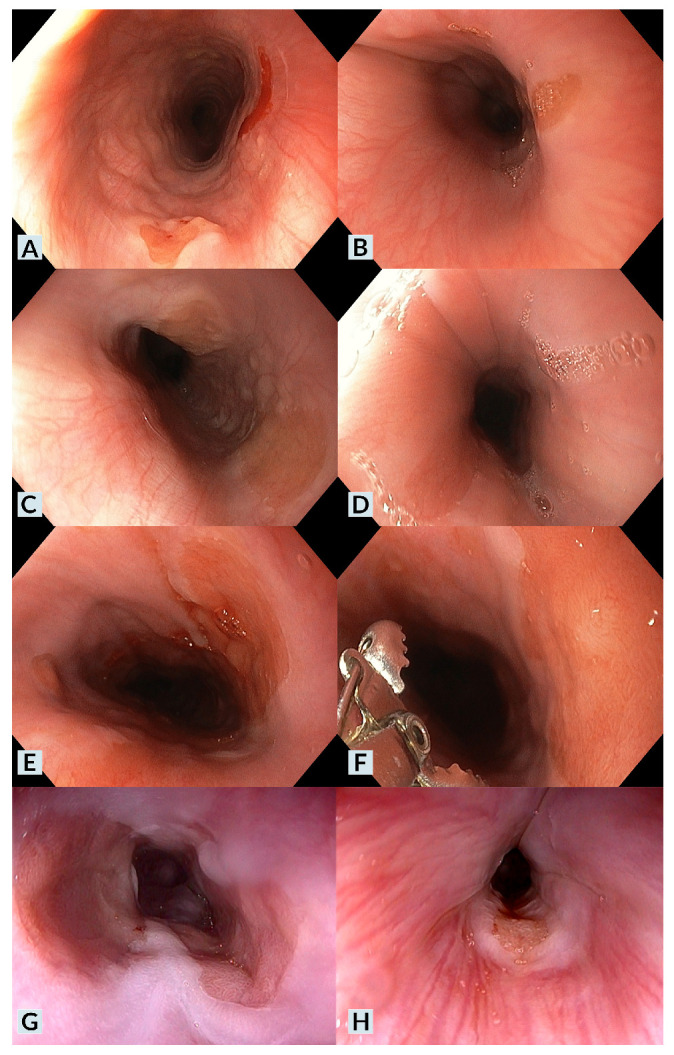 Figure 1
Figure 1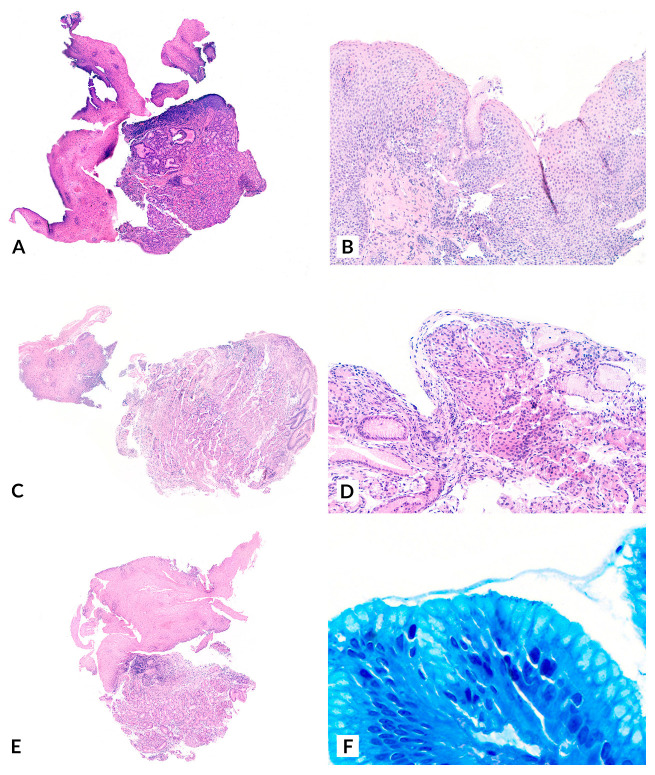 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal disorders and treatments · Eosinophilic Esophagitis · Gastrointestinal Tumor Research and Treatment
1. Introduction
Inlet patch (IP) is an anomaly characterized by gastric heterotopia in the cervical esophagus [1,2,3]. It is considered an infrequent pathology, especially in pediatric populations, although the literature regarding its prevalence is inconsistent [1,2,3,4,5,6,7].
IP etiology is presumed to be congenital, resulting from abnormal epithelial development during embryogenesis [8,9]. However, alternative hypotheses—such as an acquired origin secondary to metaplastic changes in the squamous mucosa caused by chronic acid injury—have also been proposed [7].
Clinically, IP is most often an asymptomatic lesion, incidentally diagnosed during upper gastrointestinal endoscopy (UGIE) performed for unrelated reasons. It should be noted, however, that its identification can be challenging due to its proximal location within the esophagus [1,2,3,4,5,6,7]. Nevertheless, a wide range of IP-related symptoms has been described, including dyspepsia, dysphagia, esophageal strictures or membranes, gastroesophageal reflux, bleeding, and even respiratory manifestations such as chronic bronchitis or laryngospasm [9,10,11,12,13].
From an endoscopic perspective, it is a distinctive lesion, appearing as a well-demarcated pink or salmon-colored patch. It is typically located in the upper third of the esophagus, just below the upper esophageal sphincter (UES). However, it has also been described, albeit exceptionally, in other locations, such as the mid-esophagus [14].
Although there is general agreement that incidentally detected IP should not be treated in asymptomatic patients, evidence on the management of symptomatic IP remains scarce. Proton pump inhibitors (PPIs) are considered the first-line treatment [1,2,3], as they are effective in most cases, while endoscopic therapies, such as argon plasma coagulation, are reserved for refractory cases [15]. This study aims to characterize pediatric cases diagnosed with IP at our center from 2018 to 2025.
2. Materials and Methods
This retrospective, single-center study included all pediatric patients (0–14 years) diagnosed with IP at our institution between 2018 and 2025. Two researchers collected and anonymized the patients’ sociodemographic and clinical data. A blinded pathologist evaluated all biopsies and classified the degree of IP inflammation using a qualitative scale: absence of inflammation, mild chronic inflammation, moderate to severe chronic inflammation, and acute inflammation. A descriptive analysis was performed. The study was approved by our Institutional Review Board (code 24227). Written informed consent was obtained from all legal guardians of all patients before inclusion. The study was conducted following the principles outlined in the Declaration of Helsinki (2013 statement).
3. Results
Nine patients were included, with a median age at diagnosis of 12 years (range: 6–14). Seven were male (78%), and two were female (22%).
Regarding medical history, four patients (44%) had a prior diagnosis of eosinophilic esophagitis (EoE). Among them, one also had a concomitant diagnosis of celiac disease (CD). In contrast, another had a serological and genetic profile compatible with CD but did not meet the ESPGHAN 2012 criteria, nor had histopathological confirmation of CD. Additionally, one patient in the series had insulin-resistant type 1 diabetes mellitus, and another had a previous diagnosis of gastroesophageal reflux (GER) secondary to H. pylori infection. Two patients had no relevant medical history.
Cervical esophageal symptoms were identified in six cases (67%). The most common symptoms were chronic dysphagia (60%) and GER-related symptoms (60%). Two of these six patients (40%) had experienced at least one prior episode of food impaction. When considering symptomatic IP, those in which there were no gastrointestinal comorbidities or those in which cervical esophageal symptoms were present despite the absence of underlying disease activity (e.g., cases where IP was diagnosed during an UGIE follow-up for EoE with biopsies showing no active EoE), we identified three patients (33%) with symptoms potentially attributable to IP (Case 1, Case 8, Case 9). In two of these cases, the predominant symptom was dysphagia, while in the other case, it was GER-related symptoms. IP symptoms (subacute dysphagia) in the absence of other gastrointestinal comorbidities were identified in only one case (20%) [12]. Notably, this patient had an unusually extensive IP, covering a large portion of the esophageal circumference (Figure 1, Case 1).
In all cases, a distinct lesion was identified at the level of the cervical esophagus, just below the upper esophageal sphincter. The lesion appeared as a well-demarcated, salmon-red plaque (Figure 1). Lesion size and the percentage of the affected esophageal circumference varied, with multiple IP lesions observed in three cases (Cases 1, 2, 6). A nodular or villous pattern was sometimes present at the center of the plaque (Cases 1, 3, 6). In nearly all cases, the IP exhibited friability upon contact with the endoscope and during biopsy sampling, with a tendency to bleed after endoscopic manipulation. Additionally, endoscopic findings of gastric antritis were identified in two cases (22%), while endoscopic findings suggestive of EoE were observed in four cases (44%).
Histopathological analysis of all cases confirmed gastric heterotopia in the biopsied lesions, establishing the diagnosis of IP (Figure 2). The proportion of specialized gastric epithelium (with oxyntic glands) and non-specialized gastric epithelium (with mucinous glands) varied across biopsies. Regarding the degree of inflammation, all cases exhibited different levels of chronic inflammation. Chronic inflammation was classified as “mild” in five cases (56%) and “moderate-to-severe” in four cases (44%). Among the latter, H. pylori was identified in gastric biopsies from three patients (75%), with one case (25%) also testing positive for H. pylori at the IP site using Giemsa staining. Acute inflammation was not identified histologically in any of the cases. No cytological atypia, dysplasia, or malignancy was observed in the analyzed cases.
Regarding treatment, all patients except one received oral proton pump inhibitors (PPI). PPI therapy was indicated even in asymptomatic cases due to concomitant conditions such as EoE or H. pylori-associated gastritis. Patients diagnosed with H. pylori gastritis underwent antibiotic treatment with subsequent confirmation of eradication by stool antigen testing. Additionally, three patients received dietary modifications as part of their management. All patients responded favorably to PPI therapy, with symptom improvement or complete resolution of symptoms. None exhibited refractory symptoms or required endoscopic ablation of the IP.
The duration of follow-up varied among patients; however, eight of the nine cases were diagnosed within the past 12 months, while one was diagnosed seven years ago. Table 1 presents the main sociodemographic and clinical characteristics of the patients included in the study.
4. Discussion
The present study reports a series of nine pediatric cases of IP, with a detailed description of their clinical, endoscopic, and histological features.
Regarding the prevalence of IP, recent series have reported an endoscopic prevalence rate of 1.4% [1]. However, significant variability exists among reported rates [1,4], with some specialized centers focused on adult esophageal pathology documenting an endoscopic prevalence of up to 14.8% [5]. Although outdated, pediatric autopsy series have reported even higher prevalence rates, reaching 21% [6]. A plausible explanation for this discrepancy is the underdiagnosis of IP in cases where a thorough and targeted evaluation of the cervical esophagus is not performed during UGIE [16]. In this regard, recent meta-analyses have demonstrated that studies in which endoscopists specifically focused on detecting this lesion reported a higher pooled prevalence of IP [7]. The endoscopists’ expertise in this series, who systematically examined the cervical esophageal region in all patients, likely contributed to a higher number of diagnoses in a relatively short period, potentially identifying cases that might have otherwise been missed. Given that this is a relatively unknown endoscopic finding, selectively located in a region that is challenging to explore and not routinely assessed, we believe that many patients with IP remain undiagnosed.
Immunohistochemical studies have demonstrated that IP and Barrett’s esophagus (BE) share a similar expression profile for Alcian blue pH 2.5/PAS [8], high iron diamine/Alcian blue pH 2.5 [8], cytokeratins 7/20 [9], and mucin-secreting glycoproteins (MUC) [9]. This profile differs from that observed in the ectopic gastric mucosa of Meckel’s diverticulum [8] and healthy antral mucosa [9]. These findings suggest that both IP and BE may originate from submucosal esophageal glands, which are particularly abundant at both the upper and lower ends of the esophagus [9]. Based on this hypothesis, one proposed etiopathogenic mechanism for IP is a focal upper esophageal mucosal developmental anomaly [9]. This theory may also be relevant to the malignant potential of IP through the classic BE metaplasia-dysplasia-carcinoma sequence, as cases of adenocarcinoma arising from IP have been reported [17,18,19,20,21,22,23]. Further supporting this hypothesis, some studies have documented cases of synchronous adenocarcinoma arising from cervical IP and BE-related dysplasia [24].
It is also important to note that the definition of BE varies geographically. In Asian studies, BE is often used interchangeably with gastric metaplasia. In contrast, European and Western studies refer specifically to intestinal metaplasia, which carries a higher risk of progression to adenocarcinoma. The fact that Asian studies establish a diagnosis of BE based solely on the presence of columnar epithelium in the esophagus may contribute to an overestimation of BE cases. From an endoscopic perspective, recent studies have reported concomitant BE in up to 17% of patients with IP [25]. To the best of our knowledge, malignant transformation of IP has not been documented in pediatric patients, likely due to the relatively short pediatric period within a lifetime and the low incidence of BE and esophageal neoplasms in childhood. However, given the unclear malignant potential of IP, this possibility should not be disregarded. Further studies are required to determine whether follow-up protocols for IP are necessary.
In our patient series, a significant proportion had comorbid conditions, including EoE, CD, and Insulin-dependent type 1 diabetes mellitus. However, there is a considerable selection bias, as routine UGIE is not performed in healthy and asymptomatic pediatric patients. Establishing a causal relationship between these conditions and IP is not feasible, and we believe that IP was most likely an incidental finding in patients undergoing UGIE for other indications. The same consideration applies to H. pylori-related gastritis, another reason for sometimes performing a UGIE.
Three of our patients exhibited symptoms attributable to IP, while six did not. Determining whether IP solely causes symptoms is challenging, particularly in patients with concomitant conditions, such as EoE, which can present with similar clinical manifestations. The most illustrative case in our series is Case 1, in which the patient had no gastrointestinal comorbidities. In two other cases, gastrointestinal comorbidities were present; however, the absence of EoE activity in the diagnostic UGIE for IP (Case 9) and the lack of other gastrointestinal abnormalities that could justify the symptoms (Case 8) suggest that their cervical esophageal symptoms may be attributed to IP. Nevertheless, it is essential to acknowledge that symptom attribution in these two cases remains challenging.
Some studies have attempted to demonstrate the potential role of IP in symptom development by monitoring acid secretion. In 1985, Jabbari et al. [26] reported a decrease in pH at the IP site following the intravenous administration of pentagastrin, although this was only observed in cases with large IP. Similarly, in 2001, Kim et al. [27] described a patient with pharyngeal symptoms in whom 24 h ambulatory pH monitoring demonstrated acid secretion in the cervical esophagus, with symptom improvement following PPI treatment. In our series, only one patient underwent 24 h pH monitoring, which yielded normal results.
A notable finding in our series was that all IP cases presented some degree of chronic inflammation, with some reaching moderate to severe levels. Interestingly, a potential association was observed between the severity of gastritis in the stomach, the severity of inflammation in the IP, and the presence of H. pylori. Specifically, four patients exhibited moderate to severe inflammationin the IP, and in three of them (75%), the same severity was confirmed in the gastric chamber, accompanied by H. pylori infection. Additionally, in one of these cases, H. pylori was detected within the IP tissue through Giemsa staining. However, the pathological significance of this finding remains unclear.
Several mechanisms could contribute to the development of chronic gastritis in IP, including repeated mechanical trauma due to its location in a high-transit region during swallowing (both saliva and food). It should also be considered that the IP may act as a potential reservoir for H. pylori [28,29]. Further studies systematically comparing the degree of gastritis in IP and the gastric chamber are necessary to elucidate this aspect. Similarly, future research should investigate the relationship between IP and H. pylori, focusing on prevalence, therapeutic response, and associated symptoms.
Additionally, we identified both types of gastric mucosa within the IP lesions. However, we were unable to assess their relative proportions due to limitations, including the small tissue samples obtained from endoscopic biopsies and the potential heterogeneity of epithelial distribution within the IP. We hypothesize that certain lesion areas may predominantly contain oxyntic glands (gastric corpus-type epithelium), while others may be enriched with mucin-secreting glands (gastric antrum-type epithelium). Investigating this further in living patients is highly challenging; however, autopsy studies, which allow for a comprehensive examination of the entire IP lesion, could provide valuable insights.
IP remains an underdiagnosed and poorly characterized entity in pediatric populations. It is likely congenital in origin and, while often asymptomatic, may occasionally be associated with clinical manifestations. In most cases within our series, IP was an incidental finding during UGIE, and most patients had concomitant gastrointestinal conditions. Chronic inflammation was present in all reported cases.
This manuscript has several relevant limitations that warrant discussion: (1) it is a retrospective study, which may have introduced selection bias or resulted in missing relevant clinical data; while we attempted to mitigate this by conducting an exhaustive review of all patients who underwent UGIE during the study period, this limitation cannot be entirely ruled out; (2) it is a single-center study, and therefore the clinical, endoscopic, and histopathological findings may not be generalizable to other populations, as factors such as genetics, environment, or local clinical practices could influence the presentation and are not accounted for; (3) the sample size is small, which precludes formal statistical comparisons between subgroups of interest and limits the strength of inferential analyses. On the other hand, the study also presents notable strengths: (1) the exhaustive endoscopic and histological documentation, which contributes to a thorough and accurate characterization of the reported cases; (2) the novel contribution of correlating the presence of H. pylori, the degree of gastritis, and the level of inflammation within the inlet patch, which opens the door to new lines of investigation.
Reporting additional case series with detailed endoscopic and histopathological correlation is essential to further our understanding of the etiopathogenesis, pathophysiology, diagnosis, management, and prognosis of IP.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rodríguez-Martínez A. Salazar-Quero J.C. Tutau-Gómez C. Espín-Jaime B. Rubio-Murillo M. Pizarro-Martín A. Heterotopic gastric mucosa of the proximal oesophagus (inlet patch): Endoscopic prevalence, histological and clinical characteristics in paediatric patients Eur. J. Gastroenterol. Hepatol.2014261139114510.1097/MEG.000000000000017725099680 · doi ↗ · pubmed ↗
- 2Georges A. Coopman S. Rebeuh J. Molitor G. Rebouissoux L. Dabadie A. Kalach N. Lachaux A. Michaud L. Inlet patch: Clinical presentation and outcome in children J. Pediatr. Gastroenterol. Nutr.20115241942310.1097/MPG.0b 013e 3181 f 2a 91321240021 · doi ↗ · pubmed ↗
- 3Di Nardo G. Cremon C. Bertelli L. Oliva S. De Giorgio R. Pagano N. Esophageal Inlet Patch: An Under-Recognized Cause of Symptoms in Children J. Pediatr.201617699104.e 110.1016/j.jpeds.2016.05.05927318379 · doi ↗ · pubmed ↗
- 4Borhan-Manesh F. Farnum J.B. Incidence of heterotopic gastric mucosa in the upper oesophagus Gut 19913296897210.1136/gut.32.9.9681916499 PMC 1379030 · doi ↗ · pubmed ↗
- 5Akar T. Aydın S. The true prevalence of cervical inlet patch in a specific center dealing with esophageal diseases Eur. Rev. Med. Pharmacol. Sci.2022263127313110.26355/eurrev_202205_2872935587062 · doi ↗ · pubmed ↗
- 6Variend S. Howat A.J. Upper oesophageal gastric heterotopia: A prospective necropsy study in children J. Clin. Pathol.19884174274510.1136/jcp.41.7.7423410970 PMC 1141581 · doi ↗ · pubmed ↗
- 7Yin Y. Li H. Feng J. Zheng K. Yoshida E. Wang L. Wu Y. Guo X. Shao X. Qi X. Prevalence and Clinical and Endoscopic Characteristics of Cervical Inlet Patch (Heterotopic Gastric Mucosa): A Systematic Review and Meta-Analysis J. Clin. Gastroenterol.202256 e 250e 26210.1097/MCG.000000000000151633780217 · doi ↗ · pubmed ↗
- 8Bogomoletz W.V. Geboes K. Feydy P. Nasca S. Ectors N. Rigaud C. Mucin histochemistry of heterotopic gastric mucosa of the upper esophagus in adults: Possible pathogenic implications Hum. Pathol.1988191301130610.1016/S 0046-8177(88)80285-53181950 · doi ↗ · pubmed ↗