How Obesity Complicates Breast Cancer Care: Insights From a Systematic Review of Case Reports
Adam M Bowen, Dania Baraka, Bilal Ali, Shannon Pierce, Maha Bayya

TL;DR
Obesity complicates breast cancer care by causing diagnostic delays and treatment issues, as shown through case reports.
Contribution
This systematic review highlights obesity-specific challenges in breast cancer care using individual patient case reports.
Findings
Obesity leads to delayed or misattributed breast cancer diagnoses.
Obese patients face higher risks of surgical infections and reconstructive failure.
Obesity-related factors can alter drug metabolism and treatment toxicity.
Abstract
The global rise in obesity has intersected with increasing breast cancer incidence, generating a critical need to understand how excess adiposity affects diagnostic accuracy, treatment delivery, and patient outcomes. Although large epidemiologic studies have established associations between obesity and worse breast cancer prognosis, individual-level clinical nuances remain underrepresented. This review systematically evaluates case-based evidence to identify how obesity contributes to diagnostic delays and treatment complications in breast cancer care. This systematic review was conducted according to PRISMA 2020 guidelines and registered with PROSPERO. Databases searched included PubMed, Embase, Scopus, and Google Scholar through April 2025, using terms related to breast cancer, obesity, and case reports. Eligible studies included English-language case reports or series describing…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
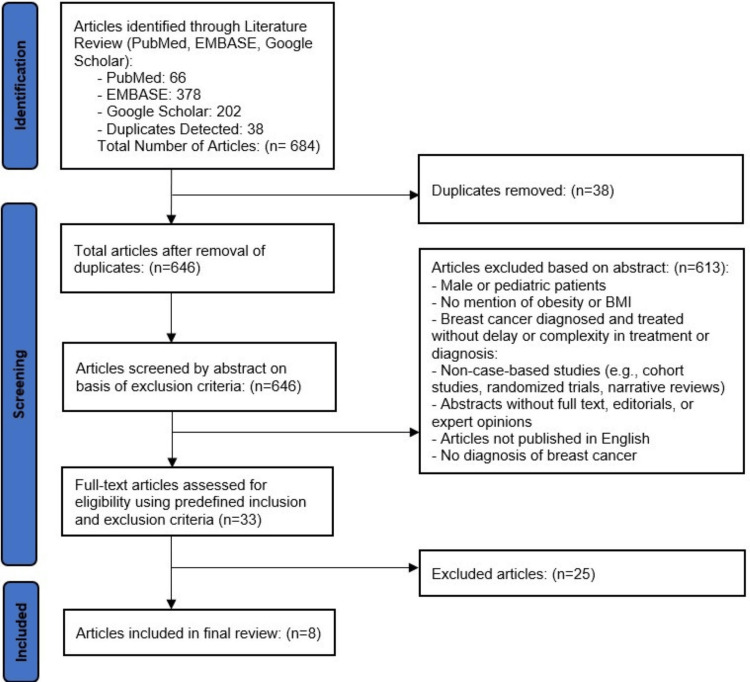 Figure 1
Figure 1| Author | Year | Country of Report | Age (years) | BMI (kg · m⁻²) | Comorbidities | Ethnicity or Race | Healthcare Setting | Obesity Description | Primary Symptoms/Atypical Presentation | Initial Misdiagnosis or Delay Cause | Time from Complication from Diagnosis | Imaging or Physical Exam Challenges | Tumor Stage at Diagnosis (I–IV or TNM) | Receptor Status (ER/PR/HER2) | Initial Treatment & Outcome | Recurrence or Progression | Survival or Follow-Up Status | Attribution to Obesity |
| Saito et al. [ | 2021 | Japan | 50s | 32.4 | Diabetes, hyperlipidemia, integration disorder syndrome | Not stated | Hospital (Hokkaido University Hospital) | BMI 32.4 kg/m²; obesity mentioned in discussion | Hypertriglyceridemia during neoadjuvant docetaxel | No delay | Detected during routine chemo labs after the 3rd cycle | Not applicable | Stage IIB | ER >90%, PR 20%, HER2+ | Neoadjuvant (DOC + HER2-targeted therapy, surgery | Not reported | Alive at last follow-up; no adverse outcomes post-surgery | Obesity, along with diabetes, may have contributed to hypertriglyceridemia |
| Mayer et al. [ | 2024 | Argentina | 64 | 31.1 | Hypertension, ischemic heart disease, obesity, smoking | Not stated | Hospital (Hospital Italiano de Buenos Aires University Institute (IUHIBA)) | BMI 31.1 kg/m², globular abdomen, visceral fat predominant | Cellulitis, mild erythema over mastectomy flaps, no fever | No delay | 12 months post-radiotherapy to infection and salvage | Radiation-induced soft tissue changes | Stage IIIC (T2N3M0) | ER+, PR+, HER2- | Modified radical mastectomy, adjuvant chemo/radiotherapy, implant-based reconstruction; infection managed conservatively, then salvaged with reverse abdominoplasty | Not reported | 2-year follow-up with good outcome | Obesity noted as a contributing risk factor for surgical site infection; affected reconstructive strategy choice |
| Nain et al. [ | 2023 | USA | 39 | 45.4 | Essential hypertension, cardiomyopathy, pregnancy (twin gestation) | Not stated | Hospital/Cardio-Oncology Clinic (Medical College of Georgia at Augusta University) | BMI explicitly reported (45.4 kg/m²) | Right breast mass with intermittent bloody nipple discharge | Patient delayed presentation (~1 year of symptoms), pregnancy complicated clinical management | Diagnosed at eight weeks gestation, chemotherapy started at 15 weeks gestation | Pregnancy complicated imaging interpretation and choice of modality | Stage IIb | ER 5%, PR 13%, HER2- | Mastectomy, chemotherapy (AC regimen), successful preterm C-section delivery at 32 weeks, stable cardiac function on medication | Not reported | Alive with close postpartum follow-up | Obesity mentioned as comorbidity complicating pregnancy and cardiovascular management |
| Swaminathan et al. [ | 2020 | USA | 60 | Not reported, but obesity mentioned | Diabetes mellitus, hypertension, obesity | Not stated | Not specified (presumably hospital-based oncology/gastroenterology clinic) | Mentioned as a risk factor for NAFLD, contributing to fibrosis | Fatigue, abdominal pain, nausea after chemotherapy | NAFLD and SOS not detected on standard imaging, delayed recognition | Approximately two weeks from chemotherapy to liver failure | Standard imaging failed to detect pre-existing liver disease | Not reported | Not reported | Cyclophosphamide chemotherapy; developed fatal SOS; transitioned to hospice | Progression to liver failure | Discharged to hospice | Obesity and NAFLD likely worsened liver injury from chemotherapy |
| Papadakis et al. [ | 2018 | Germany | 59 | 50.8 | Hypertension, diabetes mellitus Type 2, hyperlipoproteinemia, asthma, osteoporosis | Not stated | Hospital-based reconstructive surgery unit | Super obesity (BMI ≥50 kg/m²) | Breast skin necrosis after implant reconstruction | No delay | One month after the initial surgery | Not specifically stated, but preoperative mapping was required due to high BMI | pT1a, pN0, G2, R0 | Not reported | Mastectomy with implant; implant removed due to necrosis; successful DIEP flap reconstruction | None reported at 3-month follow-up | Alive with satisfactory aesthetic outcome; declined further contralateral procedure | Obesity increases surgical risk but is not a contraindication for autologous DIEP flap reconstruction |
| Atwood et al. [ | 2018 | USA | 41 | 31 | Type II diabetes mellitus, obesity | Not stated | Hospital-based surgical reconstruction (post-mastectomy) | Obese, BMI 31 | Bilateral seromas, skin necrosis, recurrent cellulitis, seroma colonized with Mucor | Initial management focused on bacterial infection; delay in diagnosis of fungal infection (Mucor) | ~5 days from seroma onset to dehiscence and culture confirmation | No imaging challenges described; initial mild erythema underestimated | Stage II (right breast) | Not reported | Tissue expander and ADM reconstruction, treated with posaconazole and antibiotics without explantation | Recurrent seromas and two episodes of cellulitis, no systemic fungal invasion | Well at 3-year follow-up post second-stage reconstruction | Obesity was a contributing risk factor for infection and impaired healing, necessitating vigilant management |
| Shen et al. [ | 2014 | China | 56 | 28.8 | Obesity, fatty liver, calculus on left renal | Not reported | Hospital (Shantou University Medical College) | BMI 28.8, described as obese | Postmenopausal vaginal bleeding, pelvic pain, palpable pelvic mass, large, hard and poorly mobile lump in the right breast | No delay | Not reported | Not reported | Uterine: Stage IB (FIGO), Breast: Stage III (T3N2M0) | ER+, PR-, HER2+ | Uterine: Hysterectomy and BSO; Breast: Mastectomy and lymph node dissection; No adjuvant therapy due to poor health | Not reported | Died 8 months after diagnosis | Obesity, along with tamoxifen use and nulliparity, increased risk for both uterine carcinosarcoma and contralateral breast cancer |
| Wills et al. [ | 2010 | USA | 58 | Not Reported (history of morbid obesity) | Secondary hyperparathyroidism, calcium malabsorption | Not reported | Beaumont Hospitals, Michigan | Morbid obesity; Roux-en-Y GBP in 2003 | Concern over tamoxifen malabsorption | No delay | Tamoxifen for ~22 months before concern | Not reported | DCIS | ER+ | Lumpectomy + radiation + tamoxifen; tamoxifen stopped due to low serum level | Not reported | Ongoing observation | Yes, malabsorption post-bariatric surgery |
| Wills et al. [ | 2010 | USA | 53 | Not reported (history of morbid obesity) | Iron deficiency | Not reported | Beaumont Hospitals, Michigan | Morbid obesity; Roux-en-Y GBP in 1997 | Concern over tamoxifen malabsorption | No delay | Tested ~8 weeks after starting tamoxifen | Not reported | T1cN0M0 | ER+ | Lumpectomy + tamoxifen; dose increased after low level | Not reported | Improved tamoxifen level to within therapeutic range | Yes, malabsorption post-bariatric surgery |
| Authors | Year | Patient Description Clear | History and Presentation Clear | Timeline Included | Diagnostic Assessment Adequate | Intervention Described Clearly | Post-Intervention Outcome Reported | Clinical Takeaway/Discussion Provided | Confounding Factors Considered | Overall Quality Rating (High/Moderate/Low) |
| Saito et al. [ | 2021 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | High |
| Mayer et al. [ | 2024 | Yes | Yes | Partial. The timeline is somewhat inferred but not explicitly structured (dates or durations are missing). | Yes | Yes | Yes | Yes | No, the study does not deeply discuss confounders or alternative explanations for the outcome. | Moderate |
| Nain et al. [ | 2023 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | High |
| Swaminathan et al. [ | 2020 | Yes | Yes | Partial. Relative timeline described (after 2nd cycle → admission → 2 weeks of worsening) but could benefit from more precise dates or intervals. | Yes | Yes | Yes | Yes | Yes | Moderate |
| Papadakis et al. [ | 2018 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | High |
| Atwood et al. [ | 2018 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | High |
| Shen et al. [ | 2014 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | High |
| Wills et al. [ | 2010 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | High |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Risks and Factors · Metabolism, Diabetes, and Cancer · Metastasis and carcinoma case studies
Introduction and background
As obesity and breast cancer rates rise globally, understanding how obesity impacts diagnosis and treatment is increasingly urgent. Obesity has been linked to higher recurrence and mortality rates in breast cancer patients and increases susceptibility to infections, including fungal infections, which are particularly concerning in immunocompromised cancer patients [1,2]. Excess adiposity can obscure physical examination findings, limit imaging accuracy, and complicate diagnostic assessments [3]. Comorbidities commonly associated with obesity, such as diabetes and nonalcoholic fatty liver disease, can further compromise treatment tolerance and outcomes [4,5]. Moreover, chronic inflammation, impaired immunity, and altered chemotherapy pharmacokinetics in obese patients may contribute to heightened infection risks and diminished treatment efficacy [6,7].
Recent National Health and Nutrition Examination Survey data show that 42% of U.S. adult women meet criteria for obesity, a prevalence that substantially overlaps with the population most affected by breast cancer [8]. Meta-analyses confirm that these women present with more advanced-stage tumors and experience 30-50 % higher breast-cancer-specific mortality than their normal-weight peers [9]. Diagnostic performance suffers as well: in a cohort of 100,622 screening mammograms, women with BMI ≥ 30 kg/m² had a 20 % higher false-positive rate, driving additional workups and anxiety [10]. Biologic mechanisms, namely increased aromatase-derived estrogen, heightened insulin-like-growth-factor-1 signaling, and chronic low-grade inflammation, further accelerate tumor initiation and progression [11]. Once treatment begins, severe obesity alters the volume of distribution and clearance of lipophilic agents such as taxanes and anthracyclines, yet real-world audits still document frequent empiric dose-capping despite ASCO guidance endorsing full weight-based dosing, leading to systematic undertreatment [12].
Despite growing recognition of these risks, the early diagnostic and treatment challenges faced by obese breast cancer patients remain underrepresented in the literature. This systematic review synthesizes published case reports and series that illustrate diagnostic delays, atypical presentations, and treatment complications specifically in obese women. Unlike cohort studies or higher-level reviews, case reports offer detailed, individual-level insights into barriers and adverse outcomes that may escape detection in larger datasets. Through these cases, this review highlights critical gaps in clinical assessment that underscore the complex interplay between obesity and cancer care and calls for more tailored strategies to improve outcomes in this vulnerable population.
Review
Methods
Study Registration
This systematic review was registered with the International Prospective Register of Systematic Reviews (PROSPERO) under the registration number [13]. No protocol amendments were necessary after registration, and the final report adheres to the methodology originally specified. The review adhered to PRISMA 2020 standards to ensure transparency, reproducibility, and methodological rigor.
Information Sources and Search Dates
A comprehensive literature search was conducted using PubMed, Embase, Scopus, and Google Scholar databases on April 15, 2025. The search included all records from inception through the search date, including English Original studies.
Database and Search Strategy
The following Boolean structure was used in PubMed: ("breast cancer" OR "breast neoplasm") AND (obesity OR "body mass index" OR “overweight”) AND ("case report" OR "case series")
Google Scholar was queried using: ("case report" OR "case study" OR "clinical case") AND ("breast cancer" OR "breast neoplasm" OR "ductal carcinoma") AND ("obese woman" OR "woman with obesity" OR "high BMI" OR "morbidly obese") AND ("misdiagnosis" OR "diagnostic delay" OR "atypical presentation" OR "misinterpreted symptoms")
Embase search syntax included: ('breast cancer'/exp OR 'breast neoplasm':ti,ab,kw) AND ('obesity'/exp OR obese*:ti,ab,kw OR 'high bmi':ti,ab,kw) AND ('case report'/exp OR 'case study':ti,ab,kw OR 'case series':ti,ab,kw) AND [english]/lim AND [humans]/lim AND [female]/lim
The search strategy was tailored for each database, incorporating both controlled vocabulary (e.g., MeSH, EMTREE) and free-text terms.
Eligibility and Exclusion Criteria
We included published case reports or case series that described female patients diagnosed with breast cancer who were reported to be obese, defined by body mass index (BMI) of ≥30 kg/m² or through explicit clinical descriptors indicating obesity. Eligible reports had to describe a delay in diagnosis and/or treatment or breast cancer treatment complications, including but not limited to cardiotoxicity, infection, or surgical risk. Only articles published in English were included, and all included reports had to provide individual-level clinical details encompassing the patient's presentation, diagnostic process, treatment course, and outcomes.
We excluded articles that involved male or pediatric patients, lacked any mention of obesity or BMI, or described breast cancer diagnosed and treated without delay or diagnostic complexity. Non-case-based publications, including cohort studies, randomized trials, and narrative reviews, were excluded along with abstracts without full text, editorials, expert commentaries, and any articles not published in English. Additionally, reports without a confirmed diagnosis of breast cancer were excluded from the final analysis.
Selection Process
Consistent with PRISMA 2020 guidance, records were first de-duplicated and then subjected to a two-stage, independent screening by two reviewers. Titles and abstracts were examined in Rayyan: citations that plainly satisfied an exclusion criterion were discarded, while all others advanced to full-text review. The same reviewers then assessed the full texts against the predefined inclusion and exclusion criteria to determine study eligibility. Any disagreements were resolved through discussion, and a third author adjudicated if consensus could not be reached.
Data Extraction and Management
All included case reports and case series were critically appraised using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist method for evaluating Case Reports. Each article was independently reviewed by two authors using the Rayyan systematic review platform, which allowed for blinded screening. Discrepancies in appraisal were resolved through discussion. Quality ratings were categorized as high, moderate, or low based on completeness, clarity, and relevance of clinical detail using JBI. These ratings informed the thematic synthesis and interpretation of the review findings, with studies. For this systematic review, we extracted detailed clinical and contextual variables from each included case report or series.
A pre-piloted extraction form on Excel was used to execute the data extraction. These included the first author and year of publication, country of report, patient age, body mass index (BMI), and documented comorbidities. We also recorded the patient's ethnicity or race (when available), the healthcare setting, and the description of obesity (e.g., BMI ≥30 or clinical designation). Clinical variables included the primary presenting symptoms, atypical features, causes of initial misdiagnosis or diagnostic delay, time from symptom onset to diagnosis, and any imaging or physical exam challenges. We also collected tumor staging (I-IV or TNM), receptor status (ER/PR/HER2), initial treatment and outcome, recurrence or progression, survival or follow-up status, and whether the authors attributed any aspect of the delay or complexity to the patient’s obesity.
Results
The summary of the article selection process is shown in Figure 1.
PRISMA Flow Diagram2020 PRISMA Flow Diagram showing the selection process of the publications included in the study.PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Characteristics of Included Cases and Quality Assessment
In total, eight case reports (seven single-patient reports and one case series of two patients) met the inclusion criteria, representing nine unique obese female breast cancer patients. Patient ages ranged from 39 to 64 years, with BMI spanning 28.8 (overweight, but described as “obese”) to 50.8 kg/m. Comorbid conditions were common. Seven out of 10 patients had at least one obesity-related comorbidity such as type 2 diabetes, hypertension, dyslipidemia, or cardiovascular disease. Early-stage breast cancer predominated (most cases were stages I-III at diagnosis), though one case involved synchronous metastatic-equivalent disease (stage IIIC nodal involvement). Tumor biology varied; several were hormone receptor-positive (ER+/PR+), and one case report documented a HER2-positive tumor (Table 1).
Table 1 summarizes the key characteristics of each case, including patient demographics, relevant comorbidities, and tumor stage. All reports clearly identified the patients as having obesity (BMI ≥30 or described as “morbidly obese”). Notably, one case series by Wills et al. described three women with prior Roux-en-Y gastric bypass for morbid obesity who later developed breast neoplasms. Across the cases, obesity often co-existed with other metabolic diseases (e.g. diabetes in four cases, fatty liver disease in two), compounding the clinical complexity [21]. Despite these challenges, initial cancer therapies were initiated in all patients. Each patient described in multi-patient case series was screened individually against the review’s BMI ≥ 30 kg/m² criterion. The three-patient series by Wills et al. [21] contributed only two patients because the third had a BMI < 30 kg/m² and therefore did not meet the predefined obesity threshold.
All included case reports were appraised with the Joanna Briggs Institute (JBI) critical checklist for case reports, and overall methodological quality was moderate to high (Table 2). Every case clearly described patient demographics and history, the diagnostic workup, interventions, and the clinical outcome.
Most reports provided a timeline of events and a discussion of the key learning points, including the influence of obesity on the case. Common minor limitations were a lack of details on long-term follow-up (in cases with short-term outcomes) and incomplete reporting of specific patient details (e.g., exact weight or ethnicity, which were often not stated). Nevertheless, all cases were deemed to have sufficient clinical details and validity for the review.
Diagnostic Challenges and Delays in Obese Patients
Several of the cases illustrated how obesity, especially alongside coexisting conditions, can delay breast cancer diagnosis due to atypical presentations. Nain et al. described a 39-year-old woman (BMI 45.4) who presented with a right breast mass and bloody nipple discharge during a twin pregnancy [16]. She delayed care for about a year, attributing symptoms to pregnancy-related changes. By diagnosis at eight weeks of gestation, the cancer was stage IIb, requiring chemotherapy during pregnancy. This case highlights how obesity and pregnancy together may obscure occult cancer symptoms, leading to delayed diagnosis, as her symptoms were initially misattributed to physiologic changes in the setting of obesity.
Obesity can also complicate the detection of treatment-related complications. Atwood et al. reported an obese, diabetic patient who developed mild erythema and seromas after reconstruction [19]. Initially treated as bacterial cellulitis, the true cause, Mucor fungal infection, was diagnosed only after five days, delaying appropriate management. Obesity-related immune dysfunction and impaired wound healing likely contributed, underscoring the need for heightened suspicion of atypical infections in this population.
Surgical and Reconstructive Complications
Obesity emerged as a significant risk factor for surgical complications in breast cancer cases, particularly regarding wound healing and infection. Three patients in this review experienced major post-surgical morbidity following breast cancer operations, necessitating complex reconstructive strategies. For instance, Papadakis et al. described a woman with super obesity (BMI 50.8) who developed extensive skin flap necrosis after mastectomy and immediate implant reconstruction (Figure 1) [18]. Her case required implant removal, debridement, and eventual salvage with a delayed deep inferior epigastric perforator flap. Despite the heightened risk of complications, the authors argued that extreme BMI should not be a contraindication to microsurgical reconstruction if managed carefully. In another case, Atwood reported an obese patient (BMI 31) who underwent bilateral tissue expander placement with acellular dermal matrix (ADM) and later developed recurrent seromas and wound necrosis infected by Mucor [19]. Prolonged antifungal therapy and surgical drainage preserved her reconstruction without implant removal. This misattribution to typical post-op infection illustrates a diagnostic pitfall, obesity-related immune dysfunction or wound healing issues predisposed the patient to an atypical infection, yet the early signs were subtle.
Similarly, Mayer et al. presented a 64-year-old Argentine woman (BMI 31) who developed a chronic surgical site infection a year after mastectomy, radiotherapy, and implant reconstruction [15]. She presented with erythema and cellulitis over the implant site without systemic symptoms. Imaging confirmed a fluid collection around the implant, and while conservative antibiotic treatment was tried, persistent infection prompted a salvage operation. Due to the patient’s visceral adiposity and poor local tissue quality post-radiation, the team opted for a reverse abdominoplasty flap. This approach leveraged her body habitus and avoided more conventional methods that might have failed in an obese, radiated field. Collectively, these cases reinforce the complexity of surgical and reconstructive planning in obese patients, highlighting the need for tailored strategies and heightened vigilance.
Metabolic and Pharmacologic Complications of Treatment
Obesity contributed to metabolic and pharmacologic complications during breast cancer treatment, particularly through dysregulated metabolism and altered drug absorption. Chemotherapy-induced metabolic toxicities were more severe in patients with obesity and related comorbidities. Saito et al. described a case of extreme hypertriglyceridemia following neoadjuvant docetaxel and trastuzumab, prompting a temporary halt in treatment to prevent pancreatitis. Another patient, reported by Swaminathan et al., developed liver failure (sinusoidal obstruction syndrome) on cyclophosphamide, likely due to underlying NAFLD and diabetes [14,17]. Despite stopping chemotherapy, the patient’s outcome was poor, highlighting how obesity may amplify rare but severe drug toxicities.
Endocrine therapy was also affected, particularly in patients with a history of bariatric surgery. Wills et al. described two women who had undergone Roux-en-Y gastric bypass and were later prescribed tamoxifen for breast cancer or prevention for breast cancer [21]. All showed subtherapeutic tamoxifen levels due to gastrointestinal malabsorption, necessitating dose adjustments or consideration of alternative therapies. Although no recurrences were reported, the risk of undertreatment was clear. The authors advocated for plasma level monitoring and non-oral alternatives when absorption is impaired. Separately, Shen et al. described a 56-year-old obese woman on tamoxifen who developed a rare uterine carcinosarcoma and contralateral breast cancer [20]. Obesity, together with tamoxifen exposure and the patient’s nulliparous status, likely synergistically raised her risk for this aggressive uterine cancer. Together, these reports emphasize that obesity, whether via altered pharmacokinetics, baseline comorbidities, or hormone-related risks, requires tailored therapeutic strategies and vigilant follow-up during breast cancer care.
Multimorbidity and Comorbidity-Driven Complexity
Nearly all cases in this review featured multimorbidity, illustrating how coexisting health conditions frequently complicate breast cancer care in obese patients. Obesity rarely occurs in isolation; it often coexists with diabetes, cardiovascular disease, or a history of bariatric surgery, each adding complexity to diagnostic and treatment decisions. In the study by Nain et al., the patient faced obesity, pregnancy, and peripartum cardiomyopathy [16]. Her heart failure required careful cardiac monitoring and influenced the timing and choice of chemotherapy. A multidisciplinary team enabled her to safely receive anthracycline-based treatment during the second trimester, culminating in a successful preterm delivery of healthy twins and stable cardiac function on follow-up. This case underscores how obesity, pregnancy, and cardiac disease require tailored diagnostic strategies (e.g., use of cardiac MRI over CT angiography) and customized treatment timelines.
Type 2 diabetes appeared in at least four cases and likely contributed to complications such as infections (Atwood et al., Mayer et al.) and metabolic derangements (Saito et al., Swaminathan et al.) [14,15,17,19]. Atwood’s patient may have been more susceptible to fungal infection due to both diabetes and obesity, while in the study by Saito et al., the patient developed extreme hypertriglyceridemia, likely driven by the combined metabolic burden. Prior bariatric surgery also featured prominently (Papadakis et al., Wills et al.), raising additional concerns about wound healing and drug absorption [18,21]. These comorbidities often necessitated deviations from standard care-e.g., preoperative vessel mapping for flap reconstruction or pre-chemotherapy liver screening in those with NAFLD. In the study by Shen et al., clinicians opted against adjuvant therapy, possibly due to her cumulative burden of obesity, liver disease, and dual malignancies, which may have influenced her outcome [20].
Discussion
Obesity adversely affects the accuracy and timing of breast cancer diagnosis, as evidenced by both case findings and broader studies. Obese women are less likely to undergo routine screening mammography, often due to issues like procedural discomfort, leading to lower adherence to early detection programs [3]. Additionally, large body habitus and breast size can mask tumors on physical exam, contributing to delayed recognition of malignancies [22]. Epidemiologic data confirm that overweight and obese patients experience more frequent diagnostic delays and present with more advanced-stage tumors compared to normal-weight women [23]. The examination of the cases in the literature illustrates how obesity can lead to atypical or overlooked presentations. Such real-world scenarios underscore that obesity fosters diagnostic blind spots that allow cancers to progress to higher stage before detection, ultimately worsening initial prognoses [23].
Obesity markedly heightens surgical complexity and complication risk during breast cancer treatment. Obese patients have a well-documented predisposition to postoperative wound complications; a study by Olsen et al. reported that obesity more than doubles the odds of surgical site infection after breast surgery, with increasing BMI driving further risk [24]. Mechanistically, impaired perfusion of adipose tissue, prolonged operative times, and difficulties in wound closure contribute to higher infection rates in this population [25]. In our review, several obese patients suffered wound-healing problems, including severe Mucor wound infection and mastectomy flap necrosis, complications rarely seen in lean patients. These cases align with large-scale analyses linking obesity to increased postoperative infections and thromboembolism [24]. Moreover, obesity can limit reconstructive options, obese women are less likely to receive breast reconstruction, and those who do face higher failure and reoperation rates [3]. Notably, one case of super-obesity (BMI >50) in the review required conversion from implant to autologous flap reconstruction after implant failure, illustrating how surgical strategy must often be tailored for the obese. Taken together, both case evidence and high-impact studies highlight obesity as a significant surgical risk factor that complicates perioperative management and necessitates vigilant, specialized care to prevent and address wound complications [24].
Obesity also compromises the efficacy of systemic breast cancer therapies and is associated with inferior treatment outcomes. Obese breast cancer patients have consistently worse disease-free and overall survival compared to their normal-weight counterparts, even when standard therapies are applied [3]. Population studies have shown lower pathologic complete response rates to neoadjuvant chemotherapy in overweight and obese women; for example, a recent study reported a pCR rate of only ~30% in obese patients versus ~45% in non-obese patients [26]. Biologically, obesity is linked to chemo-resistance via factors like insulin resistance, chronic inflammation, and adipokine-driven tumor growth, and historically some obese patients are underdosed due to safety concerns [12]. Endocrine therapy appears less effective as well; studies suggest that obese women derive smaller benefit from adjuvant hormonal therapy, possibly due to residual estrogenic stimulation from adipose tissue [3]. Several cases in this review exemplified these systemic therapy challenges: one patient with obesity and non-alcoholic fatty liver disease developed fatal liver failure from chemotherapy (unmasking how comorbid metabolic disease amplifies toxicity), and two bariatric surgery patients had subtherapeutic tamoxifen levels, indicating absorption issues. These case-based insights reinforce findings from larger trials that obesity can both blunt treatment efficacy and increase treatment-related toxicity [23]. Ensuring optimal systemic therapy in obese patients thus requires careful dosing, management of comorbidities, and perhaps novel strategies to overcome obesity-related treatment resistance.
This review uniquely contributes to the literature by marrying evidence from high-impact studies with real-world, case-based examples of how obesity complicates breast cancer care. Prior research has quantified obesity’s association with advanced disease and worse outcomes, but our compilation of case reports provides concrete narratives of diagnostic errors, delays, and therapy complications occurring in obese patients. These cases put a human context to statistical trends - showcasing, for instance, how an obese patient’s vague exam findings led to an initial missed diagnosis, or how excess adiposity directly precipitated a surgical infection or drug dosing error. By highlighting such scenarios, the review underscores the clinical urgency of addressing obesity in breast cancer management. We are amid a global obesity epidemic, with roughly 42% of the US population now obese and obesity contributing to a steady rise in breast cancer incidence [23]. As obesity portends higher recurrence and mortality across all breast cancer subtypes, the stakes for improving care in this subgroup are high. In summary, addressing obesity-related diagnostic and treatment complications with proactive, individualized interventions could significantly improve outcomes for this vulnerable and expanding patient population.
Strengths and Limitations
Strengths of this review include prospective protocol registration, exhaustive multi-database searching, duplicate screening and extraction, and use of a validated quality tool. Limitations arise from the reliance on single-case evidence and variability in the completeness of clinical detail, which together constrain generalizability.
Implications for Practice and Research
Clinicians should maintain heightened suspicion for atypical or muted presentations in women with BMI ≥ 30 kg·m⁻², ensure full weight-based systemic dosing, and involve reconstructive surgeons early when planning surgery in patients with central adiposity. Future research should evaluate targeted interventions such as obesity-tailored imaging pathways, perioperative infection-prevention bundles, and pharmacokinetic-guided dosing-to test whether they can narrow the outcome gap in this growing patient population.
Conclusions
This review reinforces that obesity introduces multifactorial challenges across the spectrum of breast cancer care, from diagnosis through treatment and reconstruction. By synthesizing these instructive case reports, we illustrate how obesity compounds diagnostic ambiguity, surgical morbidity, and pharmacologic complexity. These findings support and humanize larger-scale data linking obesity to delayed detection, increased perioperative complications, and diminished therapeutic response. As the obesity epidemic continues to rise, targeted strategies to adapt breast cancer management for this population are urgently needed. Future studies must go beyond association and begin testing specific clinical interventions designed to close the outcome gap for patients with obesity. Enhanced multidisciplinary collaboration and heightened clinician awareness of obesity-specific complications could further improve outcomes in this high-risk group.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Obesity and breast cancer prognosis: evidence, challenges, and opportunities J Clin Oncol Jiralerspong S Goodwin PJ 420342163420162790314910.1200/JCO.2016.68.4480 · doi ↗ · pubmed ↗
- 2Role of fungal infections in carcinogenesis and cancer development: a literature review Adv Pharm Bull Hosseini K Ahangari H Chapeland-Leclerc F Ruprich-Robert G Tarhriz V Dilmaghani A 7477561220223641563410.34172/apb.2022.076PMC 9675916 · doi ↗ · pubmed ↗
- 3The impact of obesity on breast cancer diagnosis and treatment Curr Oncol Rep Lee K Kruper L Dieli-Conwright CM Mortimer JE 412120193091914310.1007/s 11912-019-0787-1PMC 6437123 · doi ↗ · pubmed ↗
- 4Obesity and cancer: a current overview of epidemiology, pathogenesis, outcomes, and management Cancers (Basel) Pati S Irfan W Jameel A Ahmed S Shahid RK 15202310.3390/cancers 15020485 PMC 985705336672434 · doi ↗ · pubmed ↗
- 5Adipocytes sequester and metabolize the chemotherapeutic daunorubicin Mol Cancer Res Sheng X Parmentier JH Tucci J 170417131520172911794510.1158/1541-7786.MCR-17-0338 PMC 5726435 · doi ↗ · pubmed ↗
- 6The association between body mass index and the risk of hospitalization and mortality due to infection: a prospective cohort study Open Forum Infect Dis Yang WS Chang YC Chang CH Wu LC Wang JL Lin HH 08202110.1093/ofid/ofaa 545PMC 781707833511222 · doi ↗ · pubmed ↗
- 7Risk factors for infections, antibiotic therapy, and its impact on cancer therapy outcomes for patients with solid tumors Life (Basel) Kubeček O PaterováP NovosadováM 13871120213494791810.3390/life 11121387 PMC 8705721 · doi ↗ · pubmed ↗
- 8Prevalence of obesity among adults and youth: United States, 2015-2016 NCHS Data Brief, no 288 Hales CM Carroll MD Fryar CD Ogden CL Hyattsville, MD National Center for Health Statistics 2017 https://www.cdc.gov/nchs/data/databriefs/db 288.pdf 29155689 · pubmed ↗