A Closer Look at Radiation Exposure During Percutaneous Cryoablation for T1 Renal Tumors
Luna van den Brink, Michaël M. E. L. Henderickx, Otto M. van Delden, Harrie P. Beerlage, Daniel Martijn de Bruin, Patricia J. Zondervan

TL;DR
This study finds that kidney tumor cryoablation exposes patients to 26 mSv of radiation, which is lower than the radiation from follow-up scans.
Contribution
The study quantifies radiation exposure during cryoablation and identifies factors that influence it.
Findings
The median radiation dose during cryoablation was 26 mSv.
Follow-up CT scans expose patients to 105-158 mSv of radiation.
Higher BMI, more needles, and additional procedures increase radiation exposure.
Abstract
Radiation Exposure During Kidney Tumor Cryoablation Percutaneous cryoablation (PCA) is a minimally invasive treatment for renal tumors, offering an alternative to surgical removal. However, this CT-guided procedure exposes patients to radiation, and little is known about the magnitude of this. This study analyzed 164 PCA procedures performed on kidney cancer patients between 2014 and 2024. The radiation exposure of each procedure was measured and was compared to the estimated radiation exposure acquired during follow-up after treatment. The key findings showed that the median radiation dose during PCA was 26 mSv (millisieverts), which is relatively modest. To put this in perspective, patients typically receive much more radiation from the multiple CT scans required for long-term monitoring after treatment - between 105-158 mSv depending on which urological guidelines are followed.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
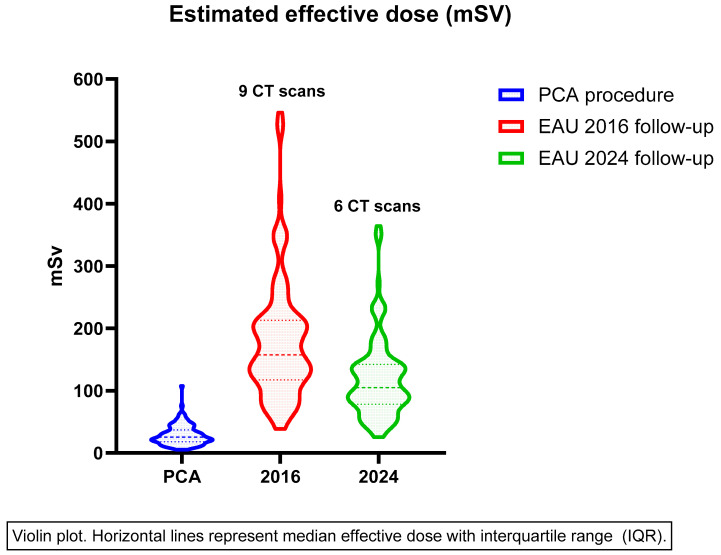 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRenal cell carcinoma treatment · Radiation Dose and Imaging · MRI in cancer diagnosis
1. Introduction
The increasing use of cross-sectional imaging has resulted in more frequent detection of small renal masses (SRMs), defined as renal tumors ≤ 4 cm [1]. Although European Association of Urology (EAU) guidelines report partial nephrectomy as the gold standard for treatment of SRMs, alternative kidney sparing treatments such as thermal ablation have gained popularity. Moreover, the guidelines consider CA as a valid treatment option for frail and/or comorbid patients with an SRM [2].
Ablative therapies have evolved rapidly over the past two decades due to the collaboration between urologists, interventional radiologists, biomedical engineers and radiation oncologists [3]. Cryoablation (CA), microwave ablation (MWA), radiofrequency ablation (RFA), stereotactic ablative radiotherapy (SABR) and irreversible electroporation (IRE) have advanced significantly in the past twenty years, with CA emerging as a well-established treatment option for SRM currently. CA has shown favorable oncological outcomes for SRMs, with local recurrence rates ranging from 2 to 8% [4,5]. This technique can be performed using a laparoscopic or percutaneous approach. Both approaches demonstrate success rates exceeding 95% and show no significant differences in complication rate, overall survival, disease-specific survival or recurrence-free survival. Nonetheless, percutaneous cryoablation (PCA) has become more commonly applied in current clinical practice due to the trend towards more minimally invasive techniques [6,7]. Studies show that for patients with tumors ranging from 4 to 7 cm, the risk of disease progression is higher after PCA [8,9]. Nevertheless, it is still employed for patients who are unfit for surgery [10].
In comparison to partial nephrectomy, advantages of PCA include lower risk of complications, a shorter hospital stay and that it is relatively non-invasive [11,12]. In the majority of PCA procedures, computed tomography (CT) imaging is utilized for planning, placement of the cryo-needles, during freezing cycles to monitor the enlarging ice ball and after freezing to assess whether the CA is complete and to establish if there are any per-ablative complications, which makes radiation exposure an inherent aspect of this technique. The literature shows that ionizing radiation can cause DNA damage, and in some cases misrepair can result in point mutations, chromosomal translocations and gene infusions. These changes are associated with an increased risk of malignancies when a cumulative radiation threshold is crossed [13,14,15]. A meta-analysis based on 111.6 million participants showed that the lifetime attribution risk (LAR) for cancer in adults following CT scans was increased (odds ratio [OR] 10) compared to adults exposed only to global background radiation (defined as 2.4 mSv per year). Cancer risk increased with a high radiation dose (OR 33) and multiple CT scan sites (OR 14) [16]. According to the ALARA-principle, physicians should strive to keep radiation exposure ‘As Low As Reasonably Achievable’ to decrease the risk of negative long-term effects of radiation for patients and medical staff whilst maintaining high image quality and providing curative treatment [17].
The literature investigating radiation exposure during PCA for the treatment of renal masses is scarce and the cohorts in these studies are small [18,19]. However, one study reported substantial radiation doses, reaching up to 8267 mG*cm, with authors suggesting that interventional radiologists should be alerted to prompt dose reduction protocols [20]. Given these findings, it is if importance to quantify the radiation exposure in a larger cohort and determine its significance.
This study aims to quantify the radiation exposure associated with PCA and to investigate factors that are associated with higher radiation exposure during this procedure. Additionally, we aim to compare the radiation exposure of PCA to the estimated exposure during follow-up after treatment.
2. Methods
2.1. Data Collection
This is a retrospective analysis of a prospectively maintained database of patients who underwent PCA in a tertiary referral center between January 2014 and September 2024. Approval to conduct this study was given by our Institutional Review Board (W22_296#22.357). Patients for whom the radiation data were available were extracted for analysis. Radiation data consisted of the dose length product (DLP) in mGy·cm, which was retrieved from the Picture Archiving Communication System (PACS). The DLP was converted into the effective dose (mSV) by using the conversion factor specific to the anatomical region (0.015 mSV·mGy^−1^·cm^−1^ for adult CT abdomen or pelvis scans), which estimates the intra-abdominal radiation based on the output from the scanner [18,21]. An online calculator was used, taking into account the age of the patient and the targeted body part. In order to depict the overall radiation exposure associated with CT scans made during follow-up, an estimation was made of the cumulative radiation exposure, assuming complete follow-up by all patients. The cumulative radiation exposure according to 2016 and 2024 EAU guidelines was estimated using the median effective dose of the first CT chest and abdomen made during follow-up.
2.2. PCA Procedure
Patients were discussed in a multidisciplinary meeting to determine the indication for PCA. Final decision on the treatment was made in a shared decision setting between urologist and patient. All patients underwent a renal tumor biopsy. Ideally, this was performed during the diagnostic process prior to the treatment, as described in a study by Widdershoven et al. [22]. Still, due to different factors, in some cases the biopsy was performed in the same session as the PCA.
The percutaneous procedures were performed under CT guidance by an experienced interventional radiologist and assistance was given by a dedicated urologist, as described by Truesdale et al. [23].
Procedures were performed under general anesthesia. After prone or lateral decubitus positioning of the patient, a spiral CT was performed to visualize the renal mass. Then, the cryoprobes were positioned under CT guidance (Siemens Sensation 64 slice, Siemens, Erlangen, Germany). If deemed necessary by the interventional radiologist and urologist, hydro- or aero-dissection was performed to prevent complications. The number and type of cryoprobes (Galil Medical^®^; Arden Hills, MN, USA) was dependent on the volume of the tumor. Short acquisition CT scans were made during the placement of the cryoprobes. The number of scans was dependent on the number of cryoprobes and whether adjustment of the probes was necessary. The freeze–thaw cycle was performed twice and consisted of ten minutes of freezing, followed by four minutes of passive thawing and one minute of active thawing. In the earliest PCA, Argon and helium gas were used for freezing and active thawing cycles, respectively, until the helium-free CX cryoprobes (Galil Medical^®^; Arden Hills, MN, USA) were used, making helium gas obsolete. After the last passive thaw cycle, the active thaw cycle was continued until the cryoprobes could easily be removed. During the freezing cycles, several spiral CT scans were made to visualize the ice ball. The goal of the ablation was to create a circumferential ablative margin around the tumor. A control CT scan was performed, during the last freeze cycle, to visualize the ablation area and assess the immediate treatment result and per-procedural complications. In general, patients were hospitalized for one night after the ablation for observation.
2.3. Follow-Up
Follow-up imaging was performed at three months to determine persistence by means of a multi-phase CT scan of the abdomen alone or chest and abdomen combined. These follow-up scans consisted of a non-enhanced scan and an arterial and venous scan. According to our institution’s protocol, follow-up scans did not include a CT of the chest, but in some cases, a scan of the chest was also made at the discretion of the treating urologist. If radiological enhancement of the ablation zone was seen at three months follow-up, it was considered persistence [24]. Subsequent follow-up was performed according to EAU guideline recommendations. Notably, EAU guideline recommendations regarding radiological follow-up after ablative therapy have changed in the past decade. Up to 2017, patients who underwent CA were classified as intermediate/high risk of recurrence and underwent more frequent imaging during follow-up compared to current guideline recommendations. The 2024 EAU guidelines do not distinguish CA from surgical treatment for follow-up imaging, thus presumably most focal ablation cases are considered low risk based on tumor size and histology from renal tumor biopsies. [2]. Table 1 shows follow-up schedules post-ablation according to different guidelines.
2.4. Statistical Analysis
Descriptive statistics were performed to show baseline characteristics and were expressed as means, medians or percentages. The effective dose (mSV) was expressed as median with interquartile range (IQR). The cumulative radiation exposure during follow-up was estimated according to the 2016 and 2024 EAU guidelines including the first CT scan at 3 months to determine persistence. Assuming complete follow-up, this corresponds to nine CT scans according to 2016 guidelines and six according to 2024 guidelines. Multivariate linear regression was performed to identify factors that are predictive of a higher effective dose during PCA procedures. The backward elimination method was used for multivariate regression. Statistical analyses were performed using SPSS version 28 (IBM Corp., Armonk, NY, USA).
3. Results
3.1. Baseline Characteristics
A total of 164 PCA procedures were performed of which radiation data was available for 133 cases. The mean age of the included patients was 65 years (±11) and the average diameter of the lesion was 28 mm (±9.6). RENAL nephrometry scores were distributed as follows: 56 patients (42%) had low anatomical complexity, 70 patients (53%) had intermediate, and 7 patients (5.3%) had high anatomical complexity. The median number of CT scans performed per procedure was 16 (11–36). Baseline characteristics are shown in Table 2. In 45 (34%) patients, procedures such as hydro- or aero-dissection were conducted during PCA. There were 13 cases of hydro-dissection, 18 cases of aero-dissection and 11 patients had both. In three cases an artificial pneumothorax was performed. More details on additional procedures are displayed in Supplementary Table S1. Three patients suffered from complications higher than Clavien Dindo grade 3. Two patients suffered a cerebral infarction the day after the PCA procedure requiring intervention, and one patient experienced neuropathic pain due to nerve damage requiring intervention by means of a nerve block.
3.2. Effective Dose
The median effective dose of a PCA procedure was 26 mSV (IQR 18–37). Follow-up imaging by means of a multiphase CT scan, of the abdomen alone or chest and abdomen combined, was available in 116 patients. There were 13 patients who had MRI and/or ultrasound during follow-up instead of CT scans. Follow-up information was not available for four patients as they were referred back to their referring urologist for follow-up.
The estimated cumulative effective dose of follow-up CT scans according to 2016 and 2024 EAU guidelines was 10 mSV (IQR 78–142) and 154 (IQR 117–213), respectively. The median effective doses of PCA and follow-up imaging are displayed in the violin plot in Figure 1. The median effective dose of PCA fluctuated slightly over the years, though it appears to remain stable between 2019 and 2024 as shown in Supplementary Figure S1.
3.3. Factors Influencing Radiation Exposure
Multivariate linear regression showed BMI (OR 1.727, p < 0.001), increasing the number of needles (OR 4.323, p < 0.001) and additional procedures (OR 7.632, p = 0.002) to be predictive for the effective dose, though the regression coefficient was low (R^2^ = 0.410, p < 0.001). Regression analyses are shown in Table 3. Age and RENAL score were not associated with increased radiation exposure.
4. Discussion
To date, CA is the most studied ablative technique and is a kidney-sparing alternative offered to patients with an SRM who are unable to undergo partial nephrectomy. This study quantified the radiation exposure during PCA and investigated factors contributing to increased radiation exposure during this procedure. We found a median effective dose of 26 mSV for a PCA procedure. Factors such as a higher BMI, a greater number of needles and the performance of hydro- or aero-dissection during PCA were correlated with a higher effective dose, whereas RENAL score and age were not.
Although the literature on this topic is limited, some small retrospective cohort studies have described radiation exposure during PCA prior to this study. A retrospective study by Tracy et al. also reported the radiation exposure for patients who underwent PCA and found a median effective dose of 30 mSV (IQR 21–47), which is similar to the findings in this study [18]. On the other hand, a study by Arnold et al. evaluated radiation exposure in a cohort of 30 patients and found a higher effective dose for PCA procedures, with an average of 40 mSV [25]. Finally, Bjorgberg et al. found a lower effective dose for PCA procedures (18 mSV), despite using the same CT scanner and number of cryoprobes as in our center, as well as a patient group with a comparable BMI [26]. This discrepancy may be attributable to the higher number of CT scans made during different phases of the PCA procedure at our institution. The amount of CT scans made during PCA procedures can vary among interventional radiologists due to preference or experience. While monitoring with spiral CT allows for the early detection of peri-operative complications and optimal evaluation of the ice ball, thereby maximizing the chance of freezing the entire lesion and minimizing the risk of damage to surrounding organs, these CT scans contribute to the overall radiation exposure [27].
In this study, factors such as BMI, the amount of needles used and the performance of hydro- and aero-dissection were associated with an increased effective dose. Obese patients often require a higher effective dose to minimize scattered radiation and maintain image quality [28]. A retrospective study by Fukushima et al. found that increased radiation exposure, expressed as the entrance skin dose (ESD), was associated with a higher number of cryoprobes and the combined use of hydro- and aero-dissection [18]. It can be expected that performing hydro- or aero-dissection will require more spiral CT scans, thereby causing the effective dose to increase. The same applies for the use of more cryoprobes, as the positioning of each probe is verified through intermittent CT scans. Also, cryoprobes are highly attenuating, and can cause artifacts in case the radiation dose is too low [29]. Lastly, factors such as the length of the scan and the desired image quality, which is subjective per physician, can also contribute to the effective dose [30]. As PCA gains a more prominent role in the treatment of SRMs, interventional radiologists should collaborate to identify where radiation exposure can be reduced when possible. Nonetheless, when physicians determine an indication for a CT scan, the benefit of radiation exposure should exceed the harm of an increased risk of malignancies [12].
Arguably, the significance of the radiation burden associated with the PCA procedure is questionable. In fact, it appears to be relatively minor when compared to the cumulative radiation exposure from CT scans during follow-up after ablative therapy. The BEIR VII model, based on studies of survivors of the atomic bombings in Hiroshima and Nagasaki, and on studies regarding occupational and medical exposures to radiation, estimates the risk of radiation-induced malignancies associated with CT scans. The American College of Radiology created a calculator based on this model to determine the LAR for developing cancer, incorporating patient age, gender and the type of exam [31]. For example, a 65-year old male has a lifetime cancer risk of 45%, and an additional risk of 0.09% after undergoing PCA for treatment of an SRM. Assuming follow-up according to the 2024 and 2016 EAU guidelines, there would be an additional cancer risk of 0.35% and 0.53%, respectively. Therefore, the additional cancer risk associated with PCA seems low when compared to radiological follow-up schedules proposed by the guidelines. Follow-up schedules proposed by international guidelines lack evidence, thus research should be carried out to determine if a reduction in CT scans is warranted in order to decrease radiation exposure. Levesque et al. described that decreasing the number of monitoring scans and a reduction in the current and kilovoltage of targeting and monitoring scans can reduce the radiation dose. Furthermore, the use of CT fluoroscopy instead of helical CT’s during targeting and monitoring can lead to further reduction [20].
Nonetheless, procedures such as ultrasound-guided or cone beam CT PCA serve as alternative ablation techniques that offer a lower radiation dose, with a mean effective dose of 4.3 mSv for abdominal cone beam CT [32]. A case series with ultrasound-guided targeting and CT-guided ice ball monitoring PCA showed promising short-term results with technical success achieved in 100% and a 1-year progression-free survival rate of 96% [33]. A recently published study comparing cone beam CT-guided PCA with CT-guided PCA found a recurrence-free survival (RFS) of 90% at a median follow-up of 40 months for cone beam and 88% for CT-guided PCA (p = 0.083) [34]. However, other series report a higher RFS for CT-guided ablation in larger cohorts [34,35,36]. Compared to CA, CT-guided RFA has shown a lower radiation exposure [37]. This can be explained by factors that are inherent to each specific treatment. RFA generally requires only one needle, whereas cryoablation requires multiple. The placement of these needles will then again require more imaging to assure correct positioning. However, even though CA has a higher radiation dose, it does have a great advantage in regard to RFA or other ablative techniques. Namely, one can visualize the extent of the ice-ball during the procedure. This allows the treating physician to treat the entire tumor with a lower change in persistence and a lower risk of complications (i.e., damage to adjacent structures) [20].
This study is one of the few studies uncovering the radiation exposure associated with PCA and reported a relatively large series of patients of a prospectively maintained database. There are some limitations to this study. First, even though this study is based on a prospectively maintained database including all procedures, the major limitation of these results lies within the retrospective nature of the study design. Second, this is a single-center study, thus it may not be reflective of patient populations in other institutions. Nonetheless, the effective dose found in this study did not differ greatly from priorly reported radiation doses in other institutions. Third, the data in this study comprises a timeframe of 10 years, meaning there could be a learning curve in performing PCAs, potentially influencing the number of CT scans made during the procedure. However, despite some fluctuation in the first five years, we did not see a significant difference in the effective dose from 2014 until 2024. Lastly, radiation data was missing in 31 patients, all of whom were treated in the beginning of the study period, which could have impacted the median effective dose.
5. Conclusions
This study found a median effective dose of 26 mSV for a PCA procedure. Though factors such as a higher BMI, the use of more cryoprobes and the performance of hydro- or aero-dissection seem to correlate with a higher effective dose, the overall radiation exposure of PCA is relatively low, specifically when compared to the estimated cumulative effective dose of surveillance CT scans.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Capitanio U. Bensalah K. Bex A. Boorjian S.A. Bray F. Coleman J. Gore J.L. Sun M. Wood C. Russo P. Epidemiology of Renal Cell Carcinoma Eur. Urol.201975748410.1016/j.eururo.2018.08.03630243799 PMC 8397918 · doi ↗ · pubmed ↗
- 2Ljungberg B. Albiges L. Abu-Ghanem Y. Bensalah K. Dabestani S. Fernández-Pello S. Giles R.H. Hofmann F. Hora M. Kuczyk M.A. European Association of Urology Guidelines on Renal Cell Carcinoma: The 2022 Update Eur. Urol.20228239941010.1016/j.eururo.2022.03.00635346519 · doi ↗ · pubmed ↗
- 3Zondervan P.J. Buijs M. De Bruin D.M. van Delden O.M. Van Lienden K.P. Available ablation energies to treat c T 1 renal cell cancer: Emerging technologies World J. Urol.20193744545510.1007/s 00345-018-2546-630448873 PMC 6424924 · doi ↗ · pubmed ↗
- 4Nielsen T.K. Lagerveld B.W. Keeley F. Lughezzani G. Sriprasad S. Barber N.J. Hansen L.U. Buffi N.M. Guazzoni G. van der Zee J.A. Oncological outcomes and complication rates after laparoscopic-assisted cryoablation: A European Registry for Renal Cryoablation (Eu RECA) multi-institutional study BJU Int.201711939039510.1111/bju.1361527488479 · doi ↗ · pubmed ↗
- 5Pickersgill N.A. Vetter J.M. Kim E.H. Cope S.J. Du K. Venkatesh R. Giardina J.D. Saad N.E. Bhayani S.B. Figenshau R.S. Ten-Year Experience with Percutaneous Cryoablation of Renal Tumors: Tumor Size Predicts Disease Progression J. Endourol.2020341211121710.1089/end.2019.088232292059 · doi ↗ · pubmed ↗
- 6Pessoa R.R. Autorino R. Laguna M.P. Molina W.R. Gustafson D. Nogueira L. da Silva R.D. Werahera P.N. Kim F.J. Laparoscopic Versus Percutaneous Cryoablation of Small Renal Mass: Systematic Review and Cumulative Analysis of Comparative Studies Clin. Genitourin. Cancer 201715513519.e 510.1016/j.clgc.2017.02.00328442227 · doi ↗ · pubmed ↗
- 7Goyal J. Verma P. Sidana A. Georgiades C.S. Rodriguez R. Single-center comparative oncologic outcomes of surgical and percutaneous cryoablation for treatment of renal tumors J. Endourol.2012261413141910.1089/end.2012.024422642574 · doi ↗ · pubmed ↗
- 8Hebbadj S. Cazzato R.L. Garnon J. Shaygi B. Buy X. Tsoumakidou G. Lang H. Gangi A. Safety Considerations and Local Tumor Control Following Percutaneous Image-Guided Cryoablation of T 1b Renal Tumors Cardiovasc. Intervent. Radiol.20184144945810.1007/s 00270-017-1820-029075877 · doi ↗ · pubmed ↗