Risk for Recurrence After Liver Resection in Patients with Hepatitis C Virus-Related Hepatocellular Carcinoma Detected After Sustained Virological Response by Direct-Acting Antivirals: A Retrospective Multicenter Study
Shogo Tanaka, Takehiro Noda, Koji Komeda, Satoshi Yasuda, Masaki Ueno, Haruki Mori, Hisashi Kosaka, Ryo Morimura, Hiroji Shinkawa, Naoko Sekiguchi, Hisashi Ikoma, Takeaki Ishizawa, Masaki Kaibori

TL;DR
This study finds that alcohol abuse and tumor size are risk factors for liver cancer recurrence after surgery in patients who achieved a hepatitis C cure with new drugs.
Contribution
Identifies alcohol abuse as a novel independent risk factor for HCC recurrence after liver resection post-DAA SVR.
Findings
3- and 5-year disease-free survival rates after liver resection were 68.7% and 55.3%.
Alcohol abuse and tumor size were independent risk factors for postoperative recurrence.
Patients without alcohol abuse had significantly better survival rates than those with alcohol abuse.
Abstract
The risk factors for postoperative recurrence in patients with hepatitis C virus (HCV)-related hepatocellular carcinoma (HCC) detected after the achievement of a sustained virological response (SVR) by direct-acting antivirals (DAAs) are unknown. The clinical records of 95 patients with initial HCV-related HCC detected after DAA-SVR achievement, who underwent liver resection, were retrospectively reviewed. The 3- and 5-year disease-free survival (DFS) rates after liver resection were 68.7% and 55.3%, respectively. Univariate and multivariate analyses identified alcohol abuse and tumor size as independent risk factors for postoperative recurrence. Continuous alcohol abuse is a risk factor for recurrence after surgery of HCC detected after the achievement of DAA-SVR. Backgrounds: Direct-acting antiviral (DAA) therapy, which achieves a high sustained virological response (SVR) rate, has…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
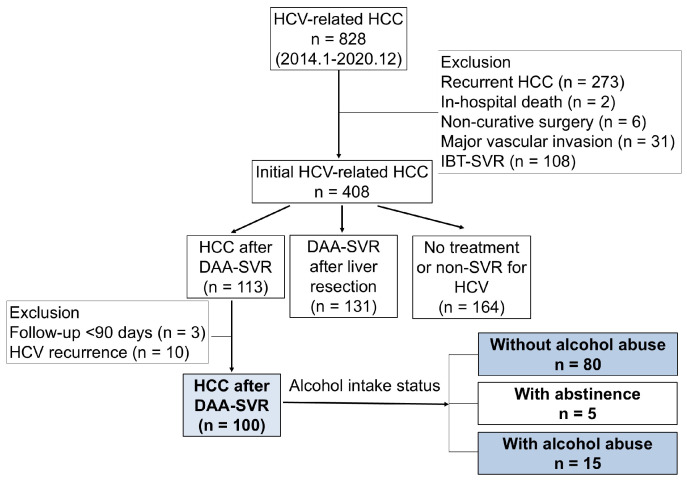 Figure 1
Figure 1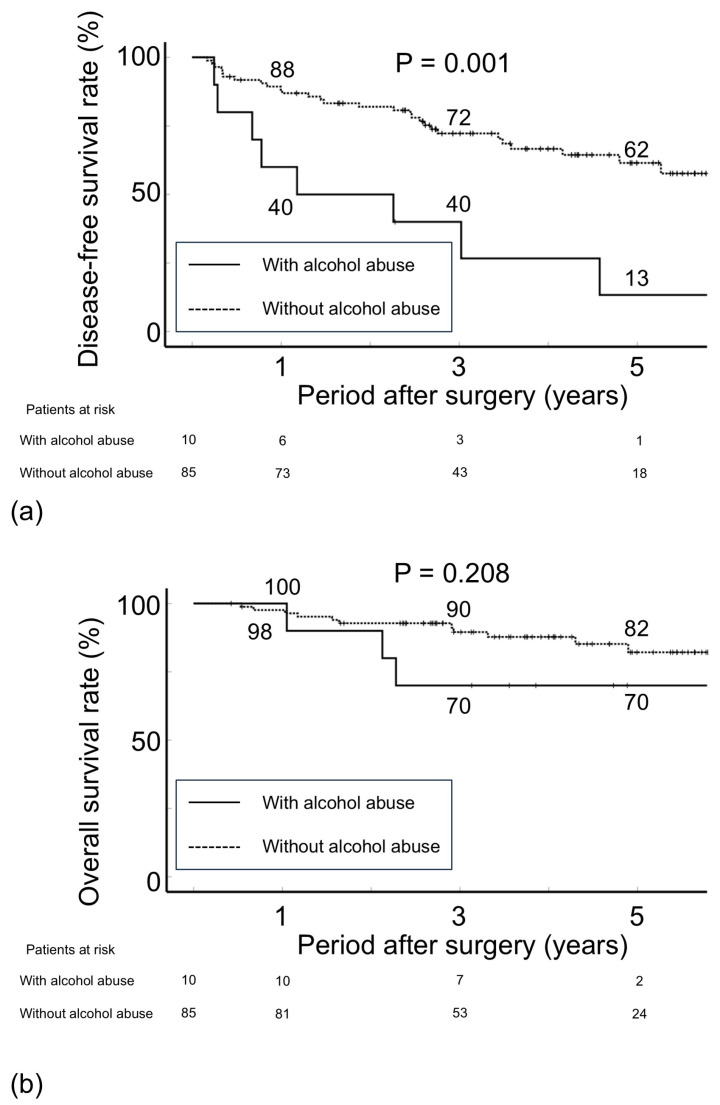 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHepatitis C virus research · Liver Disease Diagnosis and Treatment · Hepatocellular Carcinoma Treatment and Prognosis
1. Introduction
Hepatocellular carcinoma (HCC) is the third leading cause of cancer-related death worldwide [1]. In Japan, viral hepatitis remains the leading cause of HCC; however, the decrease in the prevalence of hepatitis C virus (HCV)-related HCC has changed the distribution of the etiology [2]. HCV accounted for >70% of the total number of HCCs; however, in recent years, this percentage has decreased to 20–40% [3,4]. Moreover, the high recurrence rate after curative treatment for HCV-related HCC remains an issue, with a cumulative recurrence rate of 60–90% five years after hepatic resection [5,6]. Previous studies have indicated that a sustained virologic response (SVR) induced by interferon-based therapy (IBT) decreases HCC recurrence after liver resection [7].
Direct-acting antiviral (DAA) therapy, an alternative to IBT, which achieves a high SVR rate (≥95%), has been established as a standard treatment for patients with HCV infection [8,9,10]. DAA therapy has gained popularity since insurance coverage was established for the treatment of HCV infection on 2 September 2014, in Japan. Our previous report indicated that the disease-free survival (DFS) rate after liver resection for HCC is better in patients who achieved DAA-SVR than in those without treatment or with a non-SVR [11]. However, at present, nearly all patients with HCV-related hepatitis received DAA therapy, achieving an SVR, which was not obtained in patients who had severe comorbidities or refused treatment [12]. Therefore, investigating the risk for postoperative recurrence in patients who achieved DAA-SVR is essential.
In this study, we analyzed the risk factors for postoperative recurrence in patients with HCV-related HCC that was detected after achieving DAA-SVR.
2. Materials and Methods
2.1. Patients
Between September 2014 and December 2020, 828 patients with HCV-related HCC underwent liver resection at eight university hospitals. Among these patients, 424 were excluded from the study for undergoing surgery for recurrent HCC (n = 273), in-hospital death (n = 2), noncurative surgery (n = 6), major vascular invasion (infiltration to the first branch of the portal vein and/or major hepatic vein, n = 3), or IBT-induced SVR (n = 108). Thus, 408 patients underwent liver resection for the treatment of initial HCV-related HCC. Among them, 113 achieved a DAA-SVR before HCC detection. Following the exclusion of patients with HCV recurrence after the DAA-SVR (n = 10), follow-up <90 days after surgery (n = 3), and abstinence (n = 5), 95 patients were retrospectively reviewed (Figure 1). Of the 95 patients, 10 had a history of alcohol abuse. This retrospective study was conducted following the mandates of the Helsinki Declaration and ethical committee guidelines of our institution (Osaka Metropolitan University, registration no. 2023-051).
2.2. Criteria for Hepatic Resection
In general, the criteria for hepatic resection were in accordance with the criteria of Makuuchi et al. [i.e., based on the presence or absence of ascites, the serum total bilirubin level, and the indocyanine green retention rate at 15 min (ICGR15)] [13]. Ascites were either not detected or controllable with diuretics, and the serum total bilirubin concentration was <2.0 mg/dL. Patients with a serum total bilirubin concentration between 1.1 and 1.9 mg/mL or those with ICGR15 ≥ 30% were selected for limited resection or enucleation. In patients with a serum total bilirubin concentration of ≤1.0 mg/dL, two-thirds of noncancerous liver parenchyma could be removed if ICGR15 was ≤10%, and less than one-third could be resected if this value was 10–19%, whereas those with ICGR15 of 20–29% underwent Couinaud’s segmentectomy or less. The hepatic anatomy and type of hepatic resection were classified according to the Brisbane 2000 Terminology of Liver Anatomy and Resections [14]. The treatment plan was decided by the Cancer Board, and liver resection in general was the first choice for initial HCC with good liver function and three or fewer tumors, regardless of tumor size, in accordance with the Clinical Practice Guidelines for Hepatocellular Carcinoma (5th JSH-HCC guidelines) [15].
2.3. Interferon-Free DAA Therapy for Chronic HCV Treatment
The inclusion criteria for DAA therapy were as follows: presence of serum antibodies to HCV and serum HCV RNAs and absence of hepatitis B surface antigen (HBsAg) and severe comorbidities. Among the 95 patients in the DAA group, the planned DAA regimens were as follows: sofosbuvir + ledipasvir for 12 weeks (n = 45 [with ribavirin, n = 11; without ribavirin, n = 34]), asunaprevir + daclatasvir for 24 weeks (n = 30), ombitasvir + paritaprevir + ritonavir for 12 weeks (n = 9), elbasvir + grazoprevir (n = 6), and glecaprevir + pibrentasvir (n = 5). All 95 patients completed the DAA therapy without experiencing side effects. The SVR persisted for ≥24 weeks after the commencement of DAA therapy in all patients.
2.4. Definition
Patients who took >80 g of ethanol each day for at least 5 years were defined as having alcohol abuse [16]. For this study, the cohort was divided into three groups according to the alcohol intake status: patients without alcohol abuse, patients who were once alcohol abusers but were abstinent at the time of HCC diagnosis (patients with abstinence), and patients who were alcohol abusers at the time HCC diagnosis (patients with alcohol abuse). The tumor stage was classified according to the Union for International Cancer Control (UICC) [17]. The recurrence time was defined as the duration from the day of liver resection to the day when recurrence was diagnosed based on imaging assessments. The post-recurrence survival time was measured from the date of recurrence at radiology until the date of death or last follow-up (31 December 2022). The overall survival (OS) time was defined as the interval from liver resection to the date of death or last follow-up [5,18].
2.5. Data Collection
The clinical data of all patients were collected prospectively from electronic chart records and are summarized in Table 1.
2.6. Pathology
Intraoperatively, the liver tissue sample was cut serially into 5 mm thick tissue blocks, fixed in 10% formalin, and stained with hematoxylin and eosin. All specimens were histopathologically evaluated. For non-HCC liver tissue, the histological activity index (HAI) was used, with some modifications [19,20], to evaluate the degree of hepatic fibrosis (hepatic fibrosis score). This score was defined as follows: 1, portal fibrous expansion; 2, portal–portal septa without architectural distortion; 3, portal–central septa with architectural distortion; and 4, cirrhosis.
2.7. Follow-Up Evaluations
All patients attended follow-up appointments every 3 months after discharge for 5 years following hepatic resection and every 3–6 months thereafter [20]. Follow-up evaluations included physical examination, liver function tests, chest radiography or chest-computed tomography to check for pulmonary metastases; and ultrasonography, computed tomography, and magnetic resonance imaging to check for recurrence in the remnant liver or other organs. Bone metastases were diagnosed by magnetic resonance imaging and/or bone scintigraphy. Patients who had a recurrence were treated with appropriate therapeutic modalities such as curative treatment or transcatheter arterial chemoembolization. These treatments were selected based on the patient’s general condition, tumor characteristics, and liver function at the diagnosis of HCC recurrence.
2.8. Statistical Analyses
Continuous variables are expressed as median values (range) and were compared between groups using the Mann–Whitney U test. The differences between categorical variables were analyzed using the chi-squared test or Fisher’s exact test. The Kaplan–Meier method was used to calculate DFS and OS. Differences in the rates between the selected groups were evaluated using a log-rank test. To estimate the risk factors for recurrence after liver resection, Cox’s proportional hazard model with stepwise variable selection was employed. In this study, continuous values were converted into categorical data using their median values. Variables with a p-value < 0.05 in the univariate analysis (log-rank test) were entered into the multivariate analysis. A p-value < 0.05 was considered significant. All statistical analyses were performed using IBM SPSS Statistics version 26.0 (IBM Corp., Armonk, NY, USA).
3. Results
3.1. Clinicopathological Characteristics of Patients with HCV-Related HCC Detected After DAA-SVR
Among all populations, the median follow-up period was 1,370 (range, 146–2929) days. The median duration from the start of DAA-SVR to HCC diagnosis was 788 (range, 27–2269) days (Table 1). The study included 85 patients without alcohol abuse and 10 patients with alcohol abuse. In the liver function tests, one patient had been classified into Child–Pugh class B. Among the surgery-related factors, the proportion of patients who underwent minimal invasive surgery (laparoscopic or robot-assisted liver resection) was high (78% [74/95]). Among the tumor-related factors, the median tumor size was 2.0 cm, and 47% (n = 45), 39% (n = 37), and 14% (n = 13) of the patients had UICC stages IA, IB, and II, respectively. Pathologically, liver cirrhosis was present in 35 (37%) patients.
3.2. Postoperative Recurrence
During the follow-up period, 36 (38%) patients had postoperative recurrence. The 3- and 5-year DFS rates after liver resection were 68.7% and 55.3%, respectively. Alcohol abuse, alanine aminotransferase (ALT, ≥18 IU/L), and tumor size (≥2 cm) were possible factors for postoperative recurrence (Table 2). In total, 8 of 10 patients with alcohol abuse and 28 of 85 patients without alcohol abuse had postoperative recurrence. The 3- and 5-year DFS rates after liver resection were 40.0% and 13.3% for patients with alcohol abuse and 72.2% and 61.5% for those without alcohol abuse (p = 0.001, Table 2 and Figure 2a). There was no significant difference in initial recurrence sites or treatment for recurrence (Table 3). In addition, 2 of 8 patients with alcohol abuse and 9 of 28 patients without alcohol abuse died after recurrence. There was no difference in post-recurrence survival rate among the two groups. The serum levels of aspartate aminotransferase (AST) and ALT were higher in patients with alcohol abuse (n = 10) than in those without alcohol abuse (n = 85, Table 4). However, no difference in tumor-related variables and pathological findings was noted between the two groups. During the follow-up period, in addition to the above 11 patients, 5 patients died of other malignancies or liver-unrelated diseases. The OS rate 3/5 years after surgery was 70.0%/70.0% for patients with alcohol abuse and 89.5%/82.1% for those without alcohol abuse (p = 0.208, Figure 2b).
4. Discussion
The dissemination of DAA therapy has drastically changed the treatment of patients with HCV infection. With DAA therapy, SVR was achieved in 95–97% of patients with compensated cirrhosis [8,9,10] and 85–90% of those with disease at more advanced stages [21,22]. With DAA-SVR, the 1-year HCC occurrence rate ranged from 0% to 2.2% [23,24,25,26]. The HCC occurrence rate was lower for patients who achieved DAA-SVR than for those without treatment for HCV infection or with non-SVR [24,27] and was not significantly different from the rate obtained with IBT-SVR [28,29]. As such, DAAs are now administered to patients with HCV in the absence of special circumstances [12]. Therefore, in the future, it will be important not to compare outcomes with and without DAA-SVR [11,12,30] and to study DAA-SVR cases in detail. In this study, an alcohol abuse status at the time of HCC diagnosis was found to be an independent risk factor for HCC recurrence in patients who achieved DAA-SVR.
Excess alcohol consumption is one of the major causes of HCC occurrence [31]. Previous studies have advocated that alcohol consumption had a synergistic effect on HCC development in patients with chronic viral hepatitis [31,32] and increased the HCC risk even in patients after IBT- and/or with DAA-SVR [33,34]. In this study, no difference in tumor-related variables or pathological examination data was found, and the serum transferase levels were higher in patients with alcohol abuse than in those without alcohol abuse. On the basis of this evidence, even after the achievement of DAA-SVR, continuous alcohol abuse might induce multicentric occurrence [35], rather than intrahepatic recurrence [36]. However, whether abstinence could reduce postoperative recurrence in patients with HCC detected after achieving DAA-SVR is controversial. Furthermore, there was no difference in post-recurrence survival between patients with and without alcohol abuse, which may be due to the lack of differences in Child–Pugh class and tumor-related variables, as described by Facciorusso, et al. [18].
In this study, a tumor size ≥2.0 cm was an independent risk factor for postoperative recurrence. As regards tumor-related variables, tumor size, microvascular invasion, and multiple tumors were risk factors for HCC recurrence after liver resection [37,38,39], all of which affect the tumor stage [17]. This study excluded patients with major vascular invasion. In addition, patients who received DAA therapy are generally followed routinely, leading to the detection of small HCCs (median size, 2.0 cm). Microvascular invasion and multiple tumors were not a risk for recurrence. Berardi et al. [40] reported that a tumor diameter >2 cm increased the recurrence risk. According to the UICC classification, HCCs ≤2 cm are considered “early HCC” and are classified as T1a tumors. Therefore, even after achieving DAA-SVR, a close follow-up is necessary to detect HCCs even with a small diameter, in addition to liver function tests and the analysis of tumor markers.
This study has several limitations. First, this study has a retrospective design. Second, the occurrence rate of HCC after DAA-SVR was low, and the coverage period from insurance in Japan is short; thus, the number of patients in the cohort was small. Third, no patients had stage III/IV disease, likely because the patients who received DAA therapy attended routine follow-up evaluations. Thus, the effects of DAA-SVR on advanced HCC after liver resection could not be assessed.
5. Conclusions
Alcohol abuse and tumor size appeared as independent risk factors for postoperative recurrence of HCV-related HCC after DAA-SVR. Liver function was worse in patients with alcohol abuse than in those without alcohol abuse or with abstinence. However, more studies are needed to investigate whether abstinence could reduce the postoperative recurrence rates.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bray F. Ferlay J. Soerjomataram I. Siegel R.L. Torre L.A. Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries CA Cancer J. Clin.20186839442410.3322/caac.2149230207593 · doi ↗ · pubmed ↗
- 2Enomoto H. Ueno Y. Hiasa Y. Nishikawa H. Hige S. Takikawa Y. Taniai M. Ishikawa T. Yasui K. Takaki A. The transition in the etiologies of hepatocellular carcinoma-complicated liver cirrhosis in a nationwide survey of Japan J. Gastroenterol.20215615816710.1007/s 00535-020-01748-x 33219410 PMC 7862502 · doi ↗ · pubmed ↗
- 3Nakano M. Yatsuhashi H. Bekki S. Takami Y. Tanaka Y. Yoshimaru Y. Honda K. Komorizono Y. Harada M. Shibata M. Trends in hepatocellular carcinoma incident cases in Japan between 1996 and 2019 Sci. Rep.202212151710.1038/s 41598-022-05444-z 35087153 PMC 8795252 · doi ↗ · pubmed ↗
- 4Enomoto H. Akuta N. Hikita H. Suda G. Inoue J. Tamaki N. Ito K. Akahane T. Kawaoka T. Morishita A. Etiological changes of liver cirrhosis and hepatocellular carcinoma-complicated liver cirrhosis in Japan: Updated nationwide survey from 2018 to 2021 Hepatol. Res.20245476377210.1111/hepr.1404738638067 · doi ↗ · pubmed ↗
- 5Koda M. Tanaka S. Takemura S. Shinkawa H. Kinoshita M. Hamano G. Ito T. Kawada N. Shibata T. Kubo S. Long-term prognostic factors after hepatic resection for hepatitis C virus-related hepatocellular carcinoma, with a special reference to viral status Liver Cancer 2018726127610.1159/00048690230319984 PMC 6170901 · doi ↗ · pubmed ↗
- 6Shindoh J. Hasegawa K. Inoue Y. Ishizawa T. Nagata R. Aoki T. Sakamoto Y. Sugawara Y. Makuuchi M. Kokudo N. Risk factors of post-operative recurrence and adequate surgical approach to improve long-term outcomes of hepatocellular carcinoma HPB 201315313910.1111/j.1477-2574.2012.00552.x 23216777 PMC 3533710 · doi ↗ · pubmed ↗
- 7Kubo S. Nishiguchi S. Hirohashi K. Tanaka H. Shuto T. Yamazaki O. Shiomi S. Tamori A. Oka H. Igawa S. Effects of long-term postoperative interferon-alpha therapy on intrahepatic recurrence after resection of hepatitis C virus-related hepatocellular carcinoma. A randomized, controlled trial Ann. Intern. Med.200113496396710.7326/0003-4819-134-10-200105150-0001011352697 · doi ↗ · pubmed ↗
- 8Lawitz E. Makara M. Akarca U.S. Thuluvath P.J. Preotescu L.L. Varunok P. Morillas R.M. Hall C. Mobashery N. Redman R. Efficacy and safety of ombitasvir, paritaprevir, and ritonavir in an open-label study of patients with genotype 1b chronic hepatitis C virus infection with and without cirrhosis Gastroenterology 2015149971980 e 97110.1053/j.gastro.2015.07.00126170136 · doi ↗ · pubmed ↗