Propofol Total Intravenous Anesthesia for Pediatric Proton Radiotherapy and Its Effect on Patient Outcomes
Pascal Owusu-Agyemang, Julie Mani, Techecia Idowu, Acsa Zavala, January Tsai, Ravish Kapoor, Olakunle Idowu, Jose Galdamez Melara, Pallavi Muraleedharan, Clara Francis, Lei Feng, Juan Cata

TL;DR
This study found that using propofol anesthesia for children's proton radiotherapy does not affect survival but increases the risk of unplanned hospital visits.
Contribution
The study is the first to investigate the impact of repeated propofol anesthesia on survival and hospital visits in pediatric proton radiotherapy patients.
Findings
Propofol-based anesthesia did not affect overall survival rates in children undergoing proton beam therapy.
Children receiving propofol anesthesia were 38 times more likely to have unplanned hospital admissions or emergency room visits.
Patients with propofol anesthesia were younger and had more treatment interruptions and chemotherapy history.
Abstract
To facilitate the safe and accurate delivery of radiotherapy, children undergoing proton beam therapy may require multiple anesthetic exposures over a period of 6 to 8 weeks. Research suggests the choice of anesthetic agent may influence cancer progression. To date, the influence of this many anesthetic exposures on the short- and long-term outcomes of children undergoing radiotherapy is unknown. In this retrospective study, multiple anesthetic exposures with propofol-based total intravenous anesthesia did not influence the survival of children undergoing proton beam therapy. However, compared to children who completed proton beam therapy without anesthesia, those who were undergoing treatment with propofol-based anesthesia were 38 times more likely to require an unplanned admission or emergency room visit. Further studies involving the use of other anesthetic agents may guide…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
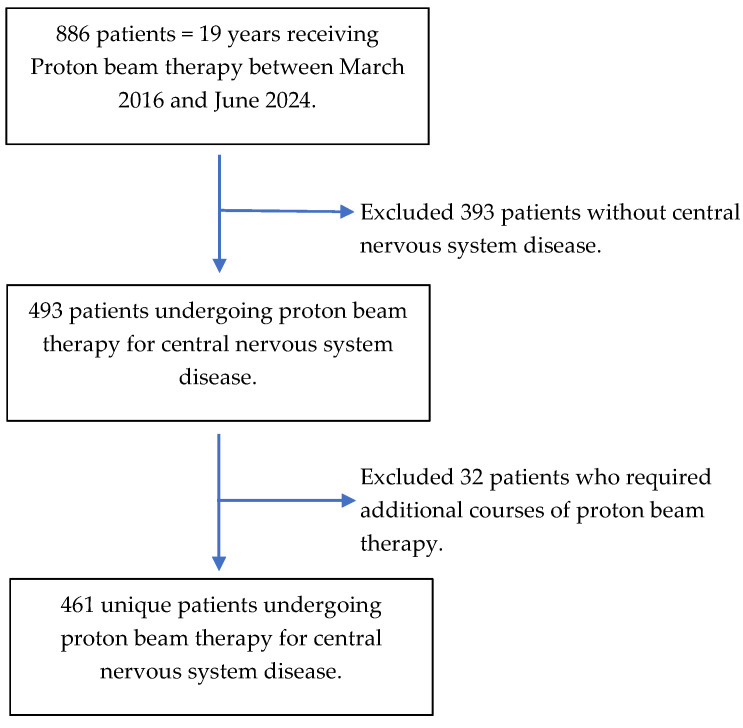 Figure 1
Figure 1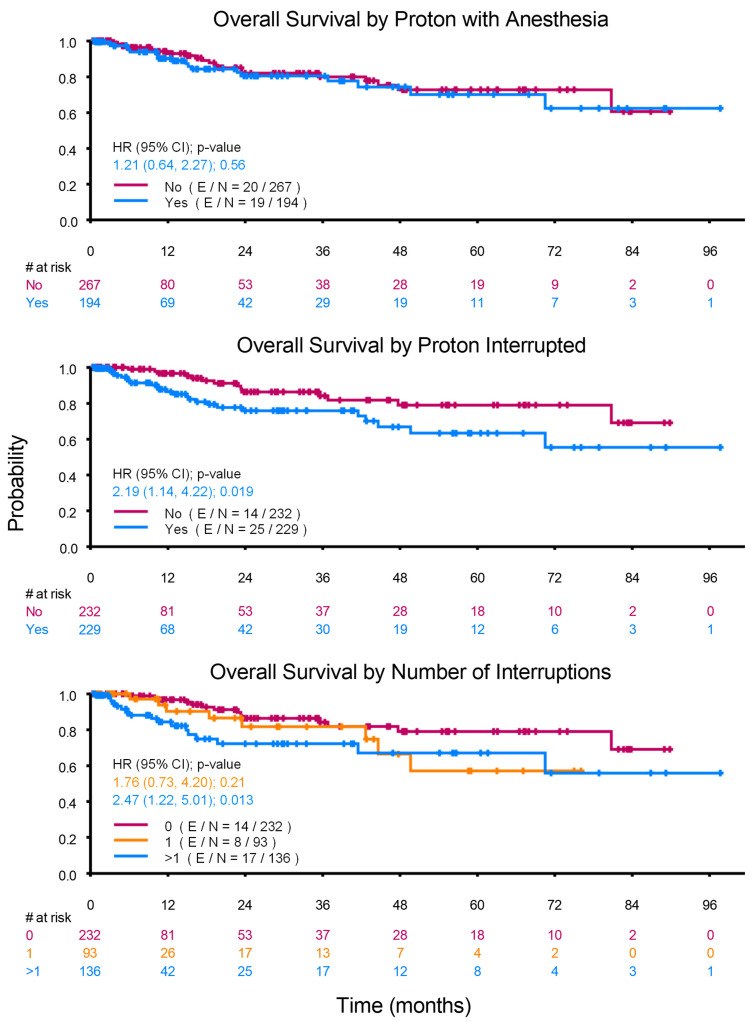 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer, Stress, Anesthesia, and Immune Response · Anesthesia and Sedative Agents · Anesthesia and Neurotoxicity Research
1. Introduction
Preclinical studies suggest the choice of anesthetics may impact oncologic outcomes [1,2]. Among these studies, the effects of volatile anesthetics and opioids have often been described as pro-metastatic, whereas propofol is mostly described as anti-oncogenic and anti-metastatic. However, the results of large randomized clinical trials on this subject have not shown any relevant differences in cancer-specific survival, making the clinical impact of the preclinical data unclear [3,4,5,6,7,8].
There are several probable explanations as to why the preclinical findings have not consistently translated into clinical results [1]. An important example is the very high doses of anesthetics that are necessary for any significant oncogenic or anti-oncogenic effects to be observed during in vitro studies [1,2]. For example, the anti-oncogenic effects of propofol have been consistently demonstrated after long periods of exposure (more than 24 h), with the most significant effects observed at doses of 10 µg/mL or higher, doses that are much higher than those used clinically [1].
It is also becoming increasingly evident that cancer-specific outcomes after exposure to volatile anesthetics or propofol may be comparable [9]. However, due to clinical limitations, few studies have been able to assess whether the oncologic outcomes of patients exposed to anesthetics differ from those of patients who did not require anesthesia for similar procedures [10,11]. Taken together, these limitations significantly impact the interpretation of available studies on anesthesia and cancer outcomes. Additional insight may be gained by studying oncologic outcomes after procedures where patients may or not require multiple general anesthetic exposures over a period of time. Hypothetically, exposure to multiple anesthetics over a period of time may serve as a surrogate for prolonged periods of exposure, and comparisons to the outcomes of patients who are able to complete their treatments without anesthesia may provide added information into assessing whether exposure to anesthetics does indeed impact oncologic outcomes.
Patient immobility is critical to ensuring the accuracy and safety of proton beam therapy. In adults and older children, this is normally achieved without anesthesia or sedation. However, attaining this degree of immobility and compliance in younger children is difficult. As a result, some children undergoing proton beam radiotherapy (PBT) may require up to 30 treatments under general anesthesia over a period of 6 to 8 weeks, with each of these treatments lasting up to 60 min [12]. This patient population provides an opportunity to assess the oncologic impact of repeated exposures to anesthetics and to compare the outcomes of children who complete their treatments with the aid of general anesthesia to those who complete them without anesthesia. In addition, it also provides an opportunity to assess the impact of multiple anesthetic exposures on the short-term outcomes of children undergoing PBT.
To this end, we conducted a single-institution retrospective study with the primary objective of comparing the survivals of children who had undergone PBT for central nervous system (CNS) malignancies under propofol-based total intravenous anesthesia (TIVA), which is the standard technique at our institution, to those of children who completed their PBT for CNS malignancies without anesthesia. Our secondary objective was to assess whether there was any association between undergoing PBT under propofol-based TIVA and the occurrence of an unplanned admission or emergency room (ER) visit within 30 days of the start of treatment. Based on the available preclinical data, our hypothesis was that children undergoing PBT under propofol TIVA would benefit from improved accuracy of radiotherapy and the potential anti-oncogenic effects of repeated infusions of propofol and thus achieve oncologic outcomes that are superior to those of children who completed their treatments without anesthesia [13,14].
2. Methods
This retrospective study was approved by the institutional review board (IRB) of The University of Texas MD Anderson Cancer Center (IRB # PA 16-0160). The requirement for written informed consent was waived by the IRB, and the findings are reported according to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines.
2.1. Study Population
Children (≤19 years of age) who had undergone PBT for central nervous system (CNS) malignancy at our comprehensive cancer center between March 2016 and June 2024 (N = 493) were included in this study. Our comprehensive cancer center is devoted exclusively to cancer patient care, research, education, and prevention. To limit the potential confounding influence of recurrent disease, only the index-prescribed course of PBT visits was considered for analysis (N = 461). The patient selection process is illustrated in Figure 1.
2.2. Study Covariates
Study covariates were extracted from subsections of the institutional electronic data warehouse and stored on the Research Electronic Data Capture web platform hosted by the University of Texas MD Anderson Cancer Center. Patient demographics, including age, gender, race, and ethnicity, were recorded. In addition, patient diagnoses and the potentially confounding oncologic variables of a prior history of chemotherapy, number of chemotherapy agents used, concurrent chemotherapy, PBT timing (date of PBT minus date of tumor surgery), PBT field of treatment (brain, spine, or craniospinal), interruptions to the prescribed course of PBT (number of days), and the reasons for interruption were recorded. The reasons for treatment interruption were classified as medical, non-medical, or unknown (when no reason was recorded). The endpoints necessary for calculating overall survival (OS) including the start date of PBT, current status (alive or deceased), and date of last follow-up alive, or date of death, were also recorded.
Regarding the secondary objectives of the study, any inpatient admission or emergency room visit within thirty days of the start of PBT, as well as the symptoms and diagnosis reported at admission, were recorded.
2.3. Anesthetic Management and Exposure Variable
At our institution, the current practice for managing patients who require anesthesia for PBT is propofol-based TIVA with spontaneous ventilation. Unless contraindicated, ondansetron is routinely administered for the prophylaxis of postoperative nausea and vomiting, and dexmedetomidine boluses are administered to children who exhibit severe emergence delirium. Children who choose to undergo PBT without anesthesia do not receive any sedatives or anesthetics from the medical team.
The exposure variable of interest was propofol-based TIVA, and patients were divided into two groups: those who completed PBT with the aid of propofol-based TIVA (propofol anesthesia group) and those who completed their treatments without anesthesia (no anesthesia group).
2.4. Statistical Analysis
Patients’ demographics, treatment, and clinical outcomes were summarized through descriptive statistics. Wilcoxon rank sum test was used to compare location parameters of continuous distributions between patient groups. The chi-square test or Fisher’s exact test was used to evaluate the association between two categorical variables. Overall survival was calculated from the start of PBT to the date of death. Patients who were alive at the time of this study were censored at the last follow-up date. The Kaplan–Meier method was used to estimate OS. Median OS time in months with 95% confidence interval was calculated. The Log-rank test was used to evaluate the difference in OS between patient groups. Cox proportional hazards models were used for multivariable analysis. Collinearity diagnostics were performed and indicated no collinearity problem. The Schoenfeld residual was used to check the proportional hazards assumption.
A multivariate logistic regression model was fitted to evaluate the association between study covariates and the status of an unplanned admission or ER visit. The full model included the covariates with p-value < 0.10 from the univariate analysis, and a backward selection method was used. The final model (number of events/number of patients [E/N] = 27/461) included the covariates with p-value less than 0.15.
To adjust for selection bias, we conducted a propensity score matching analysis of unplanned admissions/ER visits. The propensity score is the conditional probability of status (patients who underwent PBT with propofol anesthesia) conditional on a set of observed covariates. In this analysis, we included the following prognostic covariates in the multicovariable logistic model to estimate the propensity scores: chemotherapy history and the field of PBT. These covariates were significantly imbalanced between the group of patients who had propofol anesthesia and the group of patients who did not have anesthesia (p value < 0.0001, 0.0003).
The Greedy 5 → 1 digit match algorithm was used to match the baseline covariates, so that the two groups (propofol anesthesia vs. no anesthesia) would have similar propensity scores. A total of 148 patients who had propofol anesthesia and had non-missing values for the covariates were matched on a 1:1 ratio to 148 patients who did not have anesthesia and had non-missing values for the covariates. As shown in Supplemental Table S1, the standardized differences for all covariates were <0.1% in the post-matching cohort, suggesting a substantial reduction in bias between the two groups. To evaluate how strong a relationship between a confounder not represented in the analysis would need to be to result in a disruption of the observed effect of TIVA on unplanned admissions, an E-value analysis was performed. Statistical software SAS 9.4 (SAS, Cary, NC, USA) and S-Plus 8.2 (TIBCO Software Inc., Palo Alto, CA, USA) were used for all the analyses.
3. Results
3.1. Baseline Characteristics
A total of 461 children were included in this study. Their median age (Interquartile range [IQR]) was 9 years [IQR, 5–13] and 261/461 (56.6%) were male. The majority (267/461 [57.9%]) completed their course of PBT without anesthesia (no anesthesia group) and 194/461 (42.1%) completed their treatments with the aid of propofol-TIVA (propofol anesthesia group). Compared to the no anesthesia group, the propofol anesthesia group was younger (median age [IQR]; 4 years [IQR, 3–6] versus 12 years [10,11,12,13,14,15]; p < 0.001), and had higher proportions of children who had received prior chemotherapy (64/194 [33.0%] versus 18/267 [6.7%]; p < 0.001) or concurrent chemotherapy (37/194 [19.1%] versus 27/267 [10.1%]; p = 0.006). The propofol anesthesia group also had a significantly higher proportion of patients who had/or were receiving three or more chemotherapy agents (38/194 [19.6%] versus 12/267 [4.5%] in the no anesthesia group; p < 0.001) and a higher proportion of patients undergoing craniospinal radiation (55.7% versus 37.1%, p < 0.001). Interruptions to the prescribed course of PBT (Yes/No) were significantly higher in the propofol anesthesia group (111/194 [57.2%] versus 118/267 [44.2%]; p = 0.006), with a higher proportion of treatments in the propofol anesthesia group interrupted due to equipment failure or non-medical reasons (50/194 [25.8%] versus 34/267 [12.7%]; p < 0.001). Furthermore, the number of interruptions to the course of PBT was also significantly higher among the propofol anesthesia group, with 68/194 (35.1%) having more than one interruption, compared to 68/267 (25.5%) in the no anesthesia group, p = 0.019. Other baseline and clinical characteristics of the study population are shown in Table 1.
3.2. Oncological Outcome
The median follow-up time was 22.2 months (95% CI: 18.5~28.6 months). The median OS for the entire study population had not been reached. Beyond the median follow-up time of 22.2 months, there were 198 and 157 patients at risk at 24 and 36 months, respectively. The OS rates at 1, 2, and 3 years along with the 95% confidence intervals for all patients, as well as for each of the subgroups studied, are presented in Table 2.
As shown in Figure 2, the OS of the propofol anesthesia and no anesthesia groups were not significantly different (p = 0.558). Furthermore, the univariate Cox proportional hazards model did not demonstrate an association between age (as a continuous variable) and OS (Hazard Ratio, 0.961; 95% CI, 0.901–1.025; p = 0.227). Of the variables included, interruptions to the prescribed course of PBT (p = 0.019), a higher number of PBT interruptions (p = 0.033), and concurrent chemotherapy (p = 0.003) were each associated with worse survival.
3.3. Thirty-Day Unplanned Admissions or Emergency Room Visits
Of the 461 children included in this study, 27 (5.9%) had an unplanned admission or ER visit within 30 days of the start of PBT. Before propensity score matching (Table 3), the group of children who had an unplanned admission or ER visit was younger (median age [IQR], 4 years [2,3,4,5,6,7,8] versus 9 years [5,6,7,8,9,10,11,12,13]; p < 0.001) and had a higher proportion of children who had received propofol anesthesia (26/194 [13.4%] versus 1/267 [0.4%]; p < 0.001). In addition, higher proportions of children who had received previous chemotherapy (9/82 [11.0%] versus 18/379 [4.7%]; p = 0.029) and those who had interruptions to their prescribed course of PBT (19/229 [8.3%] versus 8/232 [3.4%]; p = 0.027) had an unexpected admission or ER visit. After propensity score matching (Table 3), a greater proportion of children who received propofol-TIVA required an unplanned admission/ER visit (17/148 [11.5%] versus 1/147 [0.7%] in the no anesthesia group; p < 0.001). The symptoms at readmission and the diagnoses at readmission are shown in Supplemental Tables S2 and S3, respectively.
In the multivariable analysis before propensity score matching, children who had undergone PBT with propofol-TIVA had significantly higher odds of requiring an unplanned admission or ER visit than those who completed their treatments without anesthesia (OR, 38.311; 95% CI, 5.139–285.580; p < 0.001). Interruptions to the course of PBT were not associated with an unexpected 30-day admission or ER visit (OR, 1.968; 95% CI, 0.819–4.727; p = 0.1300). After propensity score matching, PBT with propofol-TIVA (OR, 42.012; 95% CI, 5.322–331.632; p < 0.001; E-value = 83.52) and age (OR, 1.166; 95 CI, 1.003–1.357; p = 0.0461) were each associated with higher odds of an unplanned admission/ER visit. The observed E-value of 83.52 implies that considerable unmeasured confounding would be needed to explain away the effect of propofol-TIVA on unplanned admissions.
4. Discussion
In this retrospective study of 461 children who had undergone PBT for CNS disease, there was no significant difference in overall survival when comparing children who received propofol-based TIVA to those who underwent treatment without anesthesia. However, undergoing PBT under propofol-based TIVA was associated with more than a 38-fold increase in the odds of an unplanned admission or ER visit within thirty days of the start of PBT.
To date, there is limited data on the direct effect of propofol on tumors of CNS origin. The few available studies have focused on glioma and glioblastoma cells and have produced mixed results [14,15,16,17,18]. For example, in two separate in vitro studies, propofol was shown to suppress glioma cell proliferation and invasion via modulation of circular and micro-RNA expression [14,15]. However, in another in vitro study on glioma cells, Cen and colleagues showed that compared to sevoflurane, propofol significantly downregulated the potential tumor suppressors SERPINI1 and CAMK2A and upregulated the important immune checkpoint molecule CD274 (PDL 1), potentially resulting in the suppression of immune cell function and immune escape of glioma cells [16].
Furthermore, the results of the available retrospective studies suggest that the type of general anesthetic does not influence the survival of patients undergoing glioma or glioblastoma resection [17,18]. It remains unclear whether the contradictory results of the available in vitro studies have any influence on these findings. However, an often-cited limitation of retrospective studies has been the comparatively shorter duration of anesthetic exposure and the lower dose of anesthetics that are used in clinical settings. Regarding how these limitations relate to our study, it is plausible that although propofol infusions were administered on multiple consecutive days over a period of 6 to 8 weeks, the plasma levels attained in our patient population may not have been sufficient to observe any beneficial effect. It is also plausible that the pro- and anti-oncogenic effects of propofol may be effective concurrently, resulting in no influence on the survival of children undergoing radiotherapy for CNS disease. Lastly, the effect of propofol on tumors which have been exposed to multiple doses of radiotherapy and the anti-tumor effect of prolonged propofol exposure is unknown.
Similar to our findings, previous studies in adult patients have reported worse survival in patients who experienced interruptions to their course of radiotherapy [19,20]. For example, in a retrospective study of 35,845 patients with breast cancer, an increase in the number of days of interruption was associated with a corresponding increase in the likelihood of mortality [19]. Significantly, interruptions of as little as 2 days significantly impacted OS. In our study, 2 or more days of treatment interruption was associated with up to 15% decline in survival rates. It is notable that there was a significantly higher number of treatment interruptions in the propofol anesthesia group, with a significantly higher proportion related to malfunction of radiotherapy equipment or non-medical reasons. Cancelations of anesthesia cases on days when there was malfunction of radiotherapy equipment may have been related to scheduling constraints. Cancelations for non-medical reasons may have been related to anesthesia-related concerns such as violation of fasting guidelines.
To date, there is limited data on the rates of unexpected readmissions after pediatric radiotherapy. In a retrospective review of 1116 consecutive patients, the unexpected readmission rate among the 14 children included was similar to ours (5%) [21]. However, there were no comparisons between children who had received anesthesia for their treatments and those who had not. In our study, the reasons for the observed higher rates of readmission among children receiving anesthesia are not entirely clear. However, readmissions for fever and infectious complications were confined to the propofol anesthesia group. This may suggest that patients in the propofol anesthesia group were more prone to infection either due to their younger age or higher likelihood of prior and concurrent chemotherapy. In addition, propofol has been shown to suppress T-cell function, inhibit macrophage phagocytosis, and increase host susceptibility to microbial infection [22,23,24]. Thus, it is probable that our observation may suggest added immunosuppression from repeated exposure to propofol in the sub-group of children who received propofol-based TIVA for their treatments. It is also probable that frequent access of central venous lines and salient aspirations in the anesthesia group may have contributed to a higher incidence of infectious and pulmonary complications.
Regarding anesthetic technique for pediatric radiotherapy, there is currently limited data to suggest the superiority of propofol TIVA over anesthesia with volatile agents or vice versa. In a retrospective study of 739 pediatric external beam radiation procedures, anesthesia was maintained with sevoflurane and a laryngeal mask airway. The reported rate of complications was 15.7% and included nausea, vomiting, hypotension, laryngospasm, and aspiration [25]. Similar to our practice, other studies have described the use of propofol-TIVA with spontaneous ventilation and supplemental oxygen by nasal canula and reported lower complication rates (1.3%) [26]. However, further research is required to make definitive conclusions about the preferred anesthetic technique. It is notable that the risk of complications during propofol-TIVA increases with higher propofol dose, increased procedure duration, and the use of adjuncts such as benzodiazepines, opioids and ketamine [26].
There are several limitations to our study. Firstly, its retrospective nature and small sample size significantly limits the interpretation of our findings, especially those pertaining to the survival analysis. Secondly, serum propofol concentrations were not measured and it is unclear whether the concentrations attained were similar to those used during in vitro studies. Moreover, our study included children diagnosed with several tumor types, the anesthetic effects on many of which have not been studied. It is thus unclear whether the available preclinical and clinical data make for appropriate references or hypothesis creation. Lastly, our cancer center is located in an urban area with two other major children’s hospitals and their affiliate clinics. Thus, unexpected readmissions or ER visits to institutions outside our hospital network may not have been captured and could have resulted in an underestimation of unexpected readmissions.
5. Conclusions
In conclusion, in this single-institution study of children undergoing PBT, undergoing treatments with the aid of propofol-based TIVA did not impact survival but significantly increased the odds of an unexpected admission within thirty days of the start of treatment. The single-institution nature of our study and the small sample size limit the generalizability of these findings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Debel W. Ramadhan A. Vanpeteghem C. Forsyth R.G. Does the Choice of Anaesthesia Affect Cancer? A Molecular Crosstalk between Theory and Practice Cancers 20221520910.3390/cancers 1501020936612205 PMC 9818147 · doi ↗ · pubmed ↗
- 2Ramirez M.F. Gan T.J. Total intravenous anesthesia versus inhalation anesthesia: How do outcomes compare?Curr. Opin. Anaesthesiol.20233639940610.1097/ACO.000000000000127437338939 · doi ↗ · pubmed ↗
- 3Sessler D.I. Pei L. Huang Y. Fleischmann E. Marhofer P. Kurz A. Mayers D.B. Meyer-Treschan T.A. Grady M. Tan E.Y. Recurrence of breast cancer after regional or general anaesthesia: A randomised controlled trial Lancet 20193941807181510.1016/S 0140-6736(19)32313-X 31645288 · doi ↗ · pubmed ↗
- 4Yan T. Zhang G.H. Wang B.N. Sun L. Zheng H. Effects of propofol/remifentanil-based total intravenous anesthesia versus sevoflurane-based inhalational anesthesia on the release of VEGF-C and TGF-β and prognosis after breast cancer surgery: A prospective, randomized and controlled study BMC Anesth.20181813110.1186/s 12871-018-0588-3PMC 615119230243294 · doi ↗ · pubmed ↗
- 5Xu Q. Shi N.J. Zhang H. Zhu Y.M. Effects of combined general-epidural anesthesia and total intravenous anesthesia on cellular immunity and prognosis in patients with non-small cell lung cancer: A comparative study Mol. Med. Rep.2017164445445410.3892/mmr.2017.714428765974 PMC 5647004 · doi ↗ · pubmed ↗
- 6Kwon J.H. Kim J. Yeo H. Kim K. Rhu J. Choi G.S. Kim J. Joh J.W. Kim K. Kim M.J. Recurrence-free survival after hepatectomy using propofol-based total intravenous anaesthesia and sevoflurane-based inhalational anaesthesia: A randomised controlled study Anaesthesia 20258036637710.1111/anae.1648839776101 · doi ↗ · pubmed ↗
- 7Cao S.J. Zhang Y. Zhang Y.X. Zhao W. Pan L.H. Sun X.D. Jia Z. Ouyang W. Ye Q.S. Zhang F.X. Long-term survival in older patients given propofol or sevoflurane anaesthesia for major cancer surgery: Follow-up of a multicentre randomised trial Br. J. Anaesth.202313126627510.1016/j.bja.2023.01.02337474242 · doi ↗ · pubmed ↗
- 8Enlund M. Berglund A. Enlund A. Lundberg J. Wärnberg F. Wang D.X. Ekman A. Ahlstrand R. Flisberg P. Hedlund L. Impact of general anaesthesia on breast cancer survival: A 5-year follow up of a pragmatic, randomised, controlled trial, the CAN-study, comparing propofol and sevoflurane E Clinical Medicine 20236010203710.1016/j.eclinm.2023.10203737333664 PMC 10276257 · doi ↗ · pubmed ↗