The Co-Existence of mcr-1.1 and mcr-3.5 in Escherichia coli Isolated from Clinical Samples in Thailand
Panida Nobthai, Sirigade Ruekit, Dutsadee Peerapongpaisarn, Prawet Sukhchat, Brett E. Swierczewski, Nattaya Ruamsap, Paphavee Lertsethtakarn

TL;DR
This study reports the co-occurrence of two colistin resistance genes in E. coli from Thailand, raising concerns about the spread of antibiotic resistance.
Contribution
The co-existence of mcr-1.1 and mcr-3.5 on different plasmids in E. coli isolates is newly documented in this region.
Findings
Six E. coli isolates carried mcr genes, with two isolates carrying both mcr-1.1 and mcr-3.5.
mcr-1.1 was found on IncX4 plasmids, while mcr-3.5 was on IncFIB and IncFII plasmids.
The isolates belonged to ST410 and ST617 lineages, suggesting potential for widespread dissemination.
Abstract
The emergence of colistin resistance poses a significant threat to its efficacy as a last-line treatment against multidrug-resistant Gram-negative bacterial infections. In this study, 178 multi-drug resistant (MDR) Escherichia coli isolates collected from clinical samples at Queen Sirikit Naval Hospital, Chonburi, Thailand, were evaluated for colistin resistance. Of these, six were identified as mcr gene carriers, mediating colistin resistance. Specifically, mcr-1 was detected in three E. coli isolates, mcr-3 was detected in one E. coli isolate, and mcr-1 and mcr-3 were detected in two E. coli isolates, designated AMR-0220 and AMR-0361. Whole-genome sequencing and bioinformatics analysis revealed that AMR-0220 and AMR-0361 belonged to ST410 and ST617 lineages, respectively. Both isolates carried multiple plasmids, with mcr-1.1 located on an IncX4-type plasmid that is closely related to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
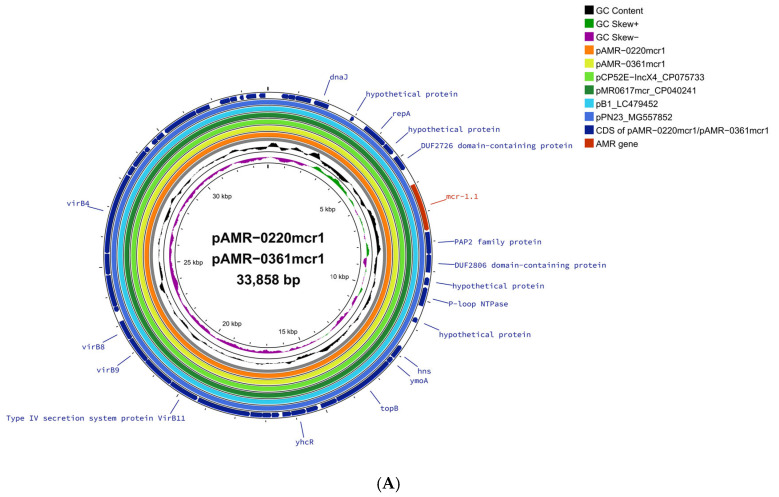 Figure 1
Figure 1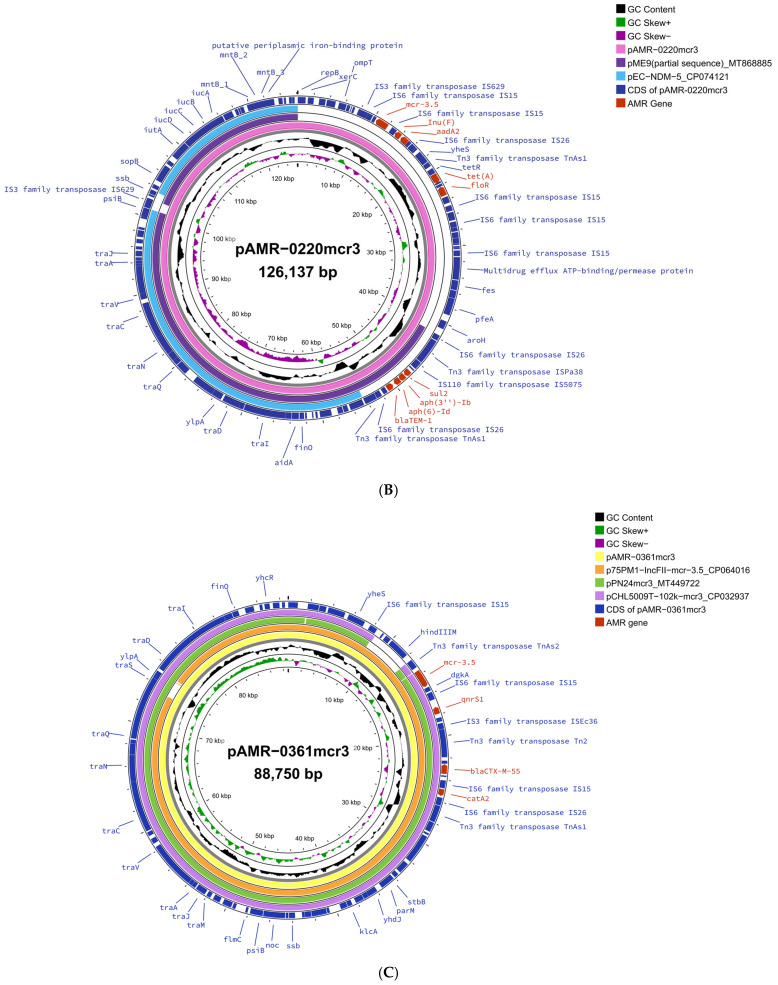 Figure 2
Figure 2- —Armed Forces Health Surveillance Division (AFHSD), Global Emerging Infections Surveillance (GEIS) Branch
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntibiotic Resistance in Bacteria · Escherichia coli research studies · Salmonella and Campylobacter epidemiology
1. Introduction
Antimicrobial resistance (AMR) in Enterobacteriaceae has become a global health concern. One of the main causes of increasing AMR is the overuse of antibiotics coupled with the lack of development of new antibiotics [1]. Older drugs, such as colistin, are considered last-line antibiotics for the treatment of infections caused by multidrug-resistant (MDR) pathogens that are resistant to three or more different antimicrobial drug classes. However, the overuse or misuse of colistin among humans and animals has led to the emergence of colistin-resistant pathogens [2]. Southeast Asia, including Thailand, is recognized as a global hotspot for AMR [3]. Between 2020 and 2022, resistance to carbapenems and third-generation cephalosporin in clinical E. coli isolates declined, while colistin resistance notably increased from 5.8% to 19.9%, highlighting a growing public health concern in Thailand [4]. Since the first report of the plasmid-mediated mobilized colistin-resistant gene (mcr-1) among Escherichia coli (E. coli) isolates in China in late 2015 [5], several other mcr genes (mcr-2 to mcr-10) and their variants have been reported worldwide [6]. As of October 2024, 37 mcr-1 variants have been submitted to the NCBI National Database of Antibiotic Resistant Organisms (NDARO) (https://www.ncbi.nlm.nih.gov/pathogens/antimicrobial-resistance/, accessed on 24 October 2024), while mcr-1 has remained prevalent and continues to be detected worldwide in various bacterial species and sources.
In Thailand, the first report of mcr-1 was isolated from E. coli in an asymptomatic individual in 2016 [7]. To date, seven mcr genes (mcr-1, mcr-2, mcr-3, and mcr-6 to mcr-9) have been detected in Enterobacteriaceae isolated from animal and human sources [7,8,9,10]. Although uncommon, the co-occurrence of different mcr genes within a single bacterial isolate has been recently reported in E. coli from clinical samples in China [11] and New Zealand [12], and from livestock in China [13], Spain [14], and France [15]. In Thailand, the co-existence of mcr genes has been reported in Klebsiella pneumoniae (K. pneumoniae) from a healthy individual [16] and in E. coli from both healthy individuals and livestock [17]. However, the co-occurrence has rarely been reported in E. coli from clinical samples. This study reports the genomic characterization of antimicrobial resistance genes and susceptibility profiles of six colistin-resistant E. coli isolated from clinical samples in Thailand. Notably, two clinical E. coli isolates, AMR-0220 and AMR-0361, were found to co-carry mcr-1.1 and mcr-3.5 genes on distinct plasmids. This co-occurrence in clinical isolates highlights the risk of enhanced resistance and plasmid-mediated spread, underscoring the need for ongoing surveillance in healthcare settings.
2. Results and Discussion
Of the 178 MDR E. coli isolates, six colistin-resistant isolates (AMR-0201, AMR-0220, AMR-0251, AMR-0354, AMR-0361, and AMR-0429) were identified and were characterized further. These six isolates were susceptible to carbapenems, nitrofurantoin, and piperacillin–tazobactam. Five isolates were intermediately resistant to tobramycin, whereas one isolate was susceptible (Table 1). All were resistant to colistin, amoxicillin–clavulanate, ampicillin, aztreonam, and tested cephems; however, resistance to cefoxitin was identified in only one isolate. Three isolates were resistant to ciprofloxacin, gentamicin, norfloxacin, trimethoprim, and trimethoprim–sulfamethoxazole (Table 1).
The six colistin-resistant E. coli isolates were initially screened for ESBL, carbapenemase, and colistin resistance genes (mcr-1 to mcr-9) using conventional and real-time PCR assays. Each isolate was found to carry at least one mcr gene, together with one or more β-lactamase genes, including blaTEM, blaCMY, or blaCTX-M. Specifically, the mcr-1 gene was identified in three isolates (AMR-0201, AMR-0251, and AMR-0354), the mcr-3 gene was identified in one isolate (AMR-0429), and the coexistence of the mcr-1 and mcr-3 genes was identified in two isolates (AMR-0220 and AMR-0361). None of the isolates carried carbapenemase genes (blaKPC, blaNDM, blaOXA-48-like, blaIMP, and blaVIM).
To further investigate the molecular characteristics of six mcr-carrying E. coli isolates, whole-genome sequencing (WGS) was performed using Illumina short-read sequencing. In addition, two isolates (AMR-0220 and AMR-0361) carrying both mcr-1 and mcr-3 were subjected to long-read sequencing using the PacBio RS II platform. The sequencing results revealed the presence of acquired resistance genes, including mcr-1.1, mcr-3.4, or coexistence of mcr-1.1 and mcr-3.5, all of which related to colistin resistance (Table 2). Furthermore, all isolates harbored genes for beta-lactam antibiotic resistance, with blaCTX-M-55 found in all isolates. In addition, blaTEM-1 was identified in three isolates, while blaCTX-M-15 and blaCMY-2 were identified in one isolate each. Genes conferring resistance to aminoglycosides, phenicols, and sulfonamides were present in five isolates, whereas AMR-0354 isolate lacked AMR genes from these categories. Additional AMR genes, conferring resistance to quinolone, macrolide, lincosamide, tetracycline, and rifampin, were also identified, as shown in Table 2.
In silico multilocus sequence typing (MLST) revealed five distinct sequence types (STs): ST410 (n = 2), ST10, ST38, ST46, and ST617 (Table 2). According to a previous study, ST410 has been reported worldwide as an MDR lineage that causes intestinal, urinary tract, and bloodstream infections in humans [18]. We found that isolates AMR-0201 and AMR-0220 both belonged to the ST410 lineage and carried genes associated with resistance to nine antibiotic classes (Table 2). Notably, ST410 is one of the most frequently identified sequence types among clinical E. coli-harboring mcr genes reported across Asia, Europe, and the Americas [19]. AMR-0251 and AMR-0361 belong to ST10 and ST617, respectively. Both isolates are members of the ST10 complex, which has been reported as the predominant lineage among clinical mcr-positive E. coli, particularly in Asia and Europe [19]. These isolates also carried genes associated with resistance to more than seven antibiotic classes. The whole-genome sequences were deposited in GenBank under BioProject No. PRJNA814829 [20].
Comparative analysis of the mcr-1.1-carrying plasmid pAMR-0220mcr1 and pAMR-0361mcr1 to reference plasmids showed that there was 100% nucleotide identity and 100% coverage with the following plasmids: pMR0617mcr (GenBank accession no. CP024041) of K. pneumoniae QS17-0029 cultured from a clinical sample from Thailand [21], pCP52E-Inc-X4 (GenBank accession no. CP075733) of E. coli isolated from healthy humans in Thailand [22], pB1 (GenBank accession no. LC479452) of E. coli B1 isolated from a wastewater sample from Japan [23], and pPN23 (GenBank accession no. MG557852) of E. coli PN23 isolated from a duck in Thailand [24], as shown in Figure 1A. The IncX4 plasmid is reported to be one of the most common plasmids carrying the mcr-1 gene, as it has been identified globally including in Thailand among human isolates [25,26]. The sequence of pAMR-0361mcr1 and pAMR-0220mcr1 was identical to pAMR0617mcr, which was carried by a K. pneumoniae isolate that we previously isolated from different clinical samples in the same hospital in 2017 [21]. These results suggest that it is possible that this IncX4-mcr-1.1 plasmid has been circulating in Enterobacteriaceae among patients in this hospital for some time, likely driven by horizontal gene transfer. The detection of an identical plasmid across different isolates raises public health concerns, as it may facilitate the silent spread of colistin resistance within healthcare settings and beyond.
pAMR-0220mcr3 was identified as a ~126 kb IncFIB plasmid carrying mcr-3.5 based on BLAST analysis (BLASTN V2.16.0). As of Oct 2024, no exact match was found in the NCBI database (Figure 1B). The sequence showed high similarity but with low coverage when compared to reference plasmids pME9 (GenBank accession no. MT868885) and pEC16-NDM-5 (GenBank accession no. CP074121). Notably, neither of those reference plasmids contained the mcr-3.5 gene. pAMR-0220mcr3 exhibited over 99% similarity with 61% coverage to the pME9 plasmid of E. coli isolated from a water source in France, which harbored four similar resistance genes, aph(3″)-Ib, aph(6)-Id, sul2, and blaTEM-1B, to pAMR-0220mcr3. However, since pME9 was deposited in Genbank as a partial sequence, the actual identity and coverage could not be further investigated. pEC16-NDM-5 was carried by an E. coli isolate from a patient in China [27]. pAMR-0220mcr3 showed 48% sequence coverage and over 99% identity with pEC19-NDM-5 (~146 kb). However, resistance genes on pEC16-NMD-5 including blaNDM-5, dfrA12, aadA2, sul1, aac(3)-IV, and aph(4)-Ia were not found on pAMR-0220mcr3. The AMR genes found on pAMR-0220mcr3 were aadA2, aph(3”)-Ib, aph(6)-Id, blaTEM-1B, floR, Inu(F), mcr-3.5, sul2, and tet(A) (Figure 1B).
The IncFII plasmid, pAMR-0361mcr3 (~89 kb), showed >99% nucleotide similarity with ≥95% coverage when compared to other IncFII plasmids, including p75M1-IncFII-mcr-3.5 (GenBank accession no. CP064016), which carries mcr-3.5; pCHL5009T-102k-mcr3 (GenBank accession no. CP032937); and pPN24 (GenBank accession no. MT449722), both carrying mcr-3.1 (Figure 1C). A previous study reported that IncFII was one of the predominant plasmids that carried mcr-3 [28]. These four IncFII plasmids shared a common plasmid backbone (>95% identity) with gene-encoding resistance to colistin (mcr-3), quinolone (qnrS1), beta-lactam (blaCTX-M-55), and chloramphenicol (catA2). p75M1-IncFII-mcr-3.5 (~88 kb) was detected in E. coli isolated from a farm pig in Thailand in 2023 [17]. pCHL5009T-102k-mcr3 (~102 kb) was detected in E. coli that was isolated from a patient in New Zealand who had traveled to Thailand prior to a hospitalization in 2017 [12]. pPN24 (~97 kb) was detected in E. coli that was isolated from a duck in Thailand in 2021 [29]. Of note, pPN24 was previously reported to harbor mcr-1 in an E. coli isolate by Yang Q. et al. [24], but was later found to also harbor mcr-3.1 by Tansawai U. et al. [29]. These findings suggest that IncFII-type plasmids may play an important role in the transmission of mcr-3 variants between human and animal sources. The IncF plasmid family, including IncFII, is a significant contributor for the dissemination of antibiotic resistance genes, especially ESBL genes, genes encoding carbapenemase, genes encoding aminoglycoside-modifying enzymes, and plasmid-mediated quinolone resistance (PMQR) genes in E. coli [30]. mcr-3-carrying IncFII plasmids have been reported to transfer efficiently via conjugation, resulting in increased colistin resistance in recipient strains [29]. The detection of mcr gene variants in both clinical and animal isolates highlights the potential for dissemination among human and animal populations. This raises public health concerns and underscores the need for ongoing surveillance.
Furthermore, the minimum inhibitory concentration (MIC) by the six E. coli isolates to colistin (4 µg/mL) revealed that the co-existence of mcr-1.1 and mcr-3.5 did not confer an increased resistance to colistin compared to isolates that carry only a single copy of the mcr gene. This finding is similar to a previous report that the co-existence of mcr-1.1 and mcr-3.5 might not provide more resistant to colistin [31].
3. Material and Methods
3.1. Bacterial Strains and Antibiotic Susceptibility Testing
A surveillance study was performed at Queen Sirikit Naval Hospital (QSH) between 2017 and 2018 to identify and characterize MDR bacterial strains from clinical samples [20]. A total of 178 MDR E. coli isolates were identified and transferred to the Walter Reed Army Institute of Research–Armed Forces Research Institute of Medical Sciences (WRAIR-AFRIMS) in Bangkok, Thailand, for further analysis. Biochemical identification and antimicrobial susceptibility testing were performed using the BD PhoenixTM 50 with NMIC/ID-4 and NMIC/ID-95 panels (BD Diagnostic Systems, Sparks, MD, USA), following the CLSI guideline 2017 for interpretation [32]. Colistin broth microdilution (BMD) was performed according to the CLSI guideline M07 (11th Edition) for method preparation and M100 (33rd Edition) for antimicrobial susceptibility testing (AST) interpretation [33,34]. E. coli ATCC 25922 was used as a quality control strain, with a testing range of 0.5 to 256 µg/mL.
3.2. Detection of Extended Spectrum Beta-Lactamase (ESBL), Carbapenemase, and Colistin Resistance Genes
Following the manufacturer’s recommendations, the whole nucleic acid of 178 MDR E. coli isolates was extracted using the QIAGEN DNeasy Blood and Tissue Kit (Germantown, MD, USA). Detection of ESBL, carbapenemase, and colistin resistance (mcr-1 to mcr-9) genes was performed using conventional multiplex PCR and real-time PCR as described previously [20].
3.3. Short- and Long-Read Whole-Genome Sequencing
Six colistin-resistant E. coli isolates were subjected to short-read sequencing on the Illumina MiSeq Benchtop sequencer as described previously (Illumina Inc., San Diego, CA, USA) [21]. Two of the strains carrying both mcr-1 and mcr-3 genes were additionally subjected to long-read sequencing on the Pacific Bioscience RSII (PacBio) platform (Pacific Biosciences, Menlo Park, CA, USA) [21].
3.4. Analysis of Whole-Genome Sequencing Data
The whole-genome sequencing (WGS) analysis was conducted as described previously [21]. Geneious v10.2.6 (Biomatters, Auckland, New Zealand) was used to perform a comparative genomic analysis. The hybrid de novo assembly of short- and long-read sequence data of AMR-220 and AMR-0361 was conducted by using Unicycler in the Genome Assembly service of the Bacterial and Viral Bioinformatics Resource Center (BV-BRC) server (https://www.bv-brc.org, accessed on 3 October 2023) [35]. In the Genome Assembly Service, the assembled genomes were polished using Pilon (v1.23.) or Racon (v1.4.20.), and the assembled graphs were plotted using Bandage (v0.8.1.). The assembly statistics of the assembled genomes were generated using QUAST (v5.0.2.) and SAMtools (v1.17). The complete genome annotation was performed using RASTtk in the Genome Annotation Service in the BV-BRC server.
Acquired AMR genes were predicted using ResFinder V4.1, the presence of plasmid types was identified with PlasmidFinder 2.1, and the sequence types (STs) of E. coli isolates, based on the Achtman scheme, were defined using the MLST 2.0 on the Center for Genomic Epidemiology (CGE) server (http://www.genomicepidemiology.org, accessed on 24 October 2024). Comparative analyses of plasmids carrying the mcr gene, with closely related reference plasmids, were generated using the circular genome viewer (CGview v1.1.2), with annotation using Prokka (v1.1.0), and the CARD resistant gene identifier (v1.2.0) on the Proksee server (https://proksee.ca/, accessed on 24 October 2024).
4. Conclusions
The colistin-resistant genes mcr-1 and mcr-3 were detected in six E. coli isolates, with two isolates carrying both genes. While the co-existence of mcr-1 and mcr-3 on distinct plasmids is commonly found in animal-derived bacteria, it remains rare in clinical isolates [8,17,28]. We identified co-existing mcr-1.1 and mcr-3.5 in 1.1% (2/178) of MDR E. coli isolates from Queen Sirikit Naval Hospital, consistent with a 2017 report of clinically isolated E. coli carrying mcr-1.1 and mcr-3.5 in Thailand [10]. Notably, one of these isolates belonged to ST410, a globally disseminated high-risk clone associated with multidrug resistance. The identification of an ST410 E. coli isolate co-harboring two mcr genes in a clinical setting is concerning, given that ST410 was recognized for its capability to acquire and disseminate AMR genes [18], suggesting a heightened potential for horizontal gene transfer facilitating the spread of colistin resistance. These findings underscore the critical need for ongoing genomic surveillance and the strengthening of existing infection control strategies to limit the spread of colistin resistance within and beyond clinical settings. Further analysis, including plasmid characterization through conjugation and transformation assays, is crucial for understanding the mechanisms of the co-existence and transmission of these mcr genes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ventola C.L. The antibiotic resistance crisis: Part 1: Causes and threats Pharm. Ther.201540277283 PMC 437852125859123 · pubmed ↗
- 2El-Sayed Ahmed M.A.E. Zhong L.L. Shen C. Yang Y. Doi Y. Tian G.B. Colistin and its role in the Era of antibiotic resistance: An extended review (2000–2019)Emerg. Microbes Infect.2020986888510.1080/22221751.2020.175413332284036 PMC 7241451 · doi ↗ · pubmed ↗
- 3Zellweger R.M. Carrique-Mas J. Limmathurotsakul D. Day N.P.J. Thwaites G.E. Baker S. Southeast Asia Antimicrobial Resistance Network A current perspective on antimicrobial resistance in Southeast Asia J. Antimicrob. Chemother.2017722963297210.1093/jac/dkx 26028961709 PMC 5890732 · doi ↗ · pubmed ↗
- 4HPSR-AMR Highlights Thailand One Health Report 2022: Antimicrobial Consumption and Antimicrobial Resistance 2025 Available online: https://www.thaiamrwatch.net/materials/92(accessed on 30 April 2025)
- 5Liu Y.Y. Wang Y. Walsh T.R. Yi L.X. Zhang R. Spencer J. Doi Y. Tian G. Dong B. Huang X. Emergence of plasmid-mediated colistin resistance mechanism MCR-1 in animals and human beings in China: A microbiological and molecular biological study Lancet Infect. Dis.20161616116810.1016/S 1473-3099(15)00424-726603172 · doi ↗ · pubmed ↗
- 6Hussein N.H. AL-Kadmy I.M.S. Taha B.M. Hussein J.D. Mobilized colistin resistance (mcr) genes from 1 to 10: A comprehensive review Mol. Biol. Rep.2021482897290710.1007/s 11033-021-06307-y 33839987 · doi ↗ · pubmed ↗
- 7Olaitan A.O. Chabou S. Okdah L. Morand S. Rolain J.M. Dissemination of the mcr-1 colistin resistance gene Lancet Infect. Dis.20161614710.1016/S 1473-3099(15)00540-X 26711360 · doi ↗ · pubmed ↗
- 8Phuadraksa T. Wichit S. Arikit S. Songtawee N. Yainoy S. Co-occurrence of mcr-2 and mcr-3 genes on chromosome of multidrug-resistant Escherichia coli isolated from healthy individuals in Thailand Int. J. Antimicrob. Agents 20226010666210.1016/j.ijantimicag.2022.10666236007781 · doi ↗ · pubmed ↗