Leukocyte-Rich Platelet-Rich Plasma’s Clinical Effectiveness in Arthroscopic Rotator Cuff Repair: A Meta-Analysis of Randomized Controlled Trials
Peiyuan Tang, Meihui Huang, Wenfeng Xiao, Ting Wen, Pavel Volotovsky, Mikhail Gerasimenko, Shiyao Chu, Shuguang Liu, Kai Zhang, Yusheng Li

TL;DR
This study finds that using leukocyte-rich platelet-rich plasma during rotator cuff surgery can reduce pain and improve shoulder function in patients.
Contribution
The study provides a meta-analysis showing clinical benefits of leukocyte-rich PRP in arthroscopic rotator cuff repair.
Findings
LR-PRP improves Constant Score, ASES score, and UCLA score after rotator cuff repair.
LR-PRP reduces postoperative pain as measured by the Visual Analog Scale.
No significant effect on the Simple Shoulder Test score.
Abstract
Background: Arthroscopic rotator cuff repair faces high retear risks in multi-tendon injuries due to insufficient biological healing; leukocyte-rich PRP may enhance tendon–bone integration through inflammatory modulation and growth factor release. Methods: Four databases including PubMed, Embase, Cochrane Library, and Web of Science were searched until March 2025. Literature screening, quality evaluation, and data extraction were performed according to inclusion and exclusion criteria. GRADE was used to grade the strength of the evidence and the results. Results: The main finding of this study was that leukocyte-rich platelet-rich plasma combined with arthroscopic surgery for rotator cuff injuries can improve the Constant Score (MD = 1.13, 95% CI: 0.19, 2.07, p = 0.02, I2 = 47%), American Shoulder and Elbow Surgeons score (MD = 6.02, 95% CI: 4.67, 7.36, p < 0.01, I2 = 0%), and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
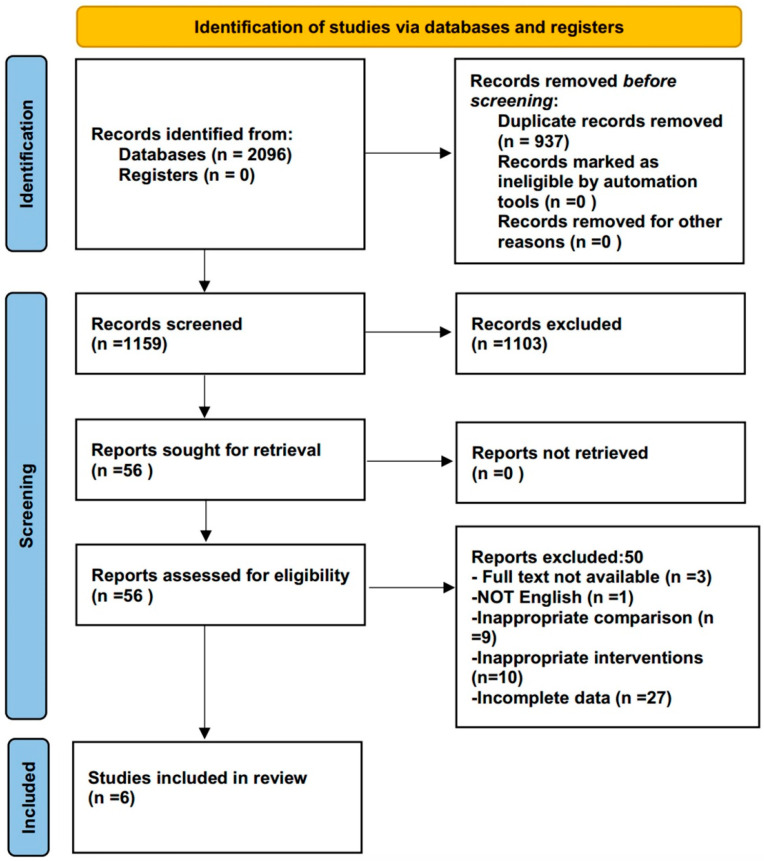 Figure 1
Figure 1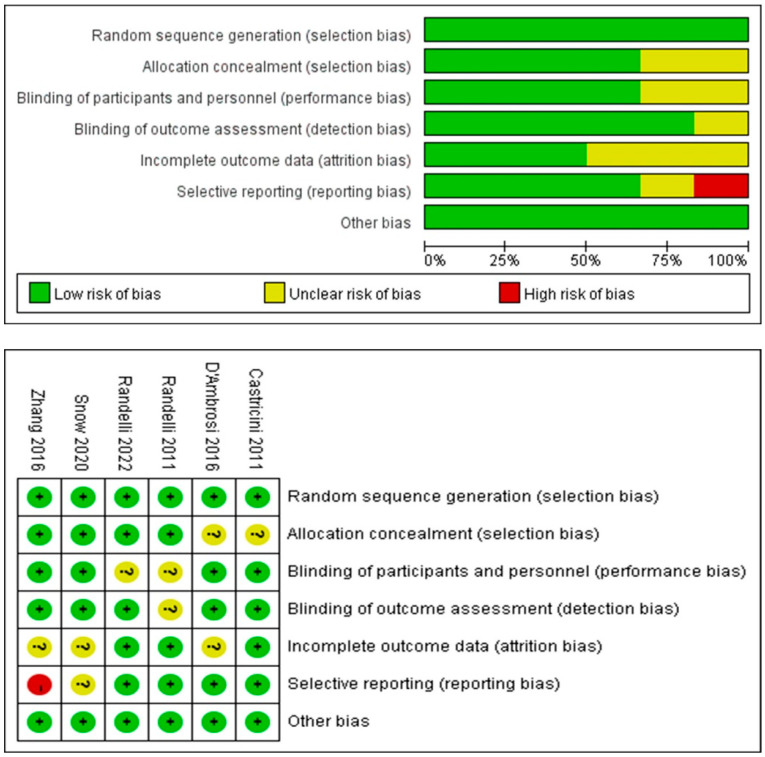 Figure 2
Figure 2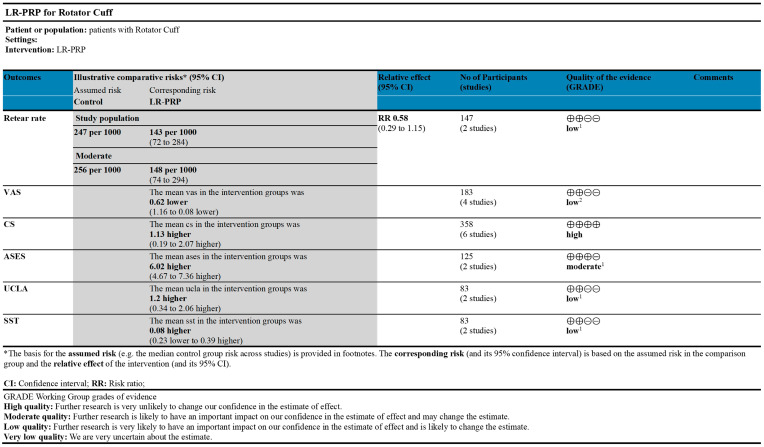 Figure 3
Figure 3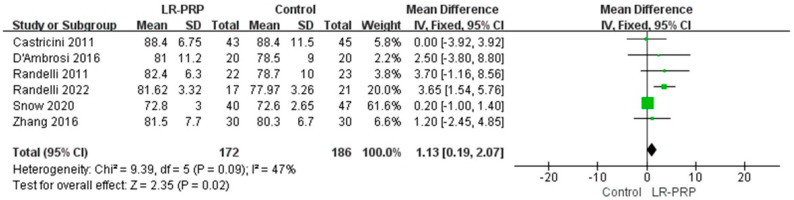 Figure 4
Figure 4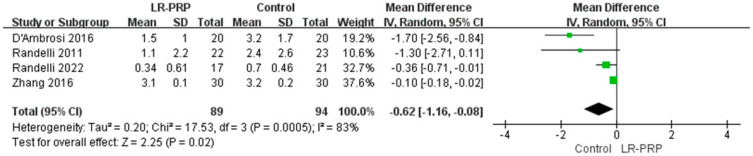 Figure 5
Figure 5- —National Key R&D Program of China
- —National Natural Science Foundation of China
- —Projects of International Cooperation and Exchanges NSFC
- —Hunan Provincial Science Fund for Distinguished Young Scholars
- —National Clinical Research Center for Geriatric Disorders
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsShoulder Injury and Treatment · Shoulder and Clavicle Injuries · Sports injuries and prevention
1. Introduction
Rotator cuff injuries are a common shoulder ailment that are often caused by trauma, excessive shoulder movement, or degenerative disease [1]. Shoulder discomfort, decreased strength, and restricted shoulder joint motion are typical signs of a rotator cuff injury [2]. Rotator cuff injuries affect a patient’s ability to perform daily activities, including employment, mobility, and sleep. Regarding the current therapeutic landscape of rotator cuff injuries, arthroscopic surgery is preferred, as it allows patients to quickly recover with few complications [3]. However, the procedure’s reliance on scar-mediated tendon-to-bone healing introduces a critical paradox: although single-tendon repairs achieve satisfactory healing rates, multi-tendon involvement correlates with escalating retear risks due to inadequate biological integration at the fibrovascular interface [4]. In response to this biomechanical–biological divide, platelet-rich plasma (PRP) therapy has emerged as a promising biologic adjunct.
Concentrated platelet solution taken from autologous whole blood is known as PRP [5]. Compared to whole blood, PRP has three to six times the concentration of platelets [6,7]. Clinically, PRP is exclusively prepared from a patient’s own blood (autologous) to avoid immunogenicity. PRP possesses the capability to unleash a diverse array of growth factors [8]. Therefore, PRP has the ability to promote tendon regeneration in cases of injury or degeneration [9]. Leukocyte-rich PRP (LR-PRP), a specialized subset of PRP, retains physiologic or supra-physiologic concentrations of neutrophils, monocytes, and lymphocytes—a critical distinction from standard PRP preparations that exclude leukocytes during centrifugation. While leukocytes in LR-PRP may theoretically impede healing in certain contexts, their role in orchestrating stage-specific inflammatory signaling is critical for tendon–bone interface repair [10]. Growth factors and cytokines can also be released by white blood cells, which are crucial for cell signaling [11]. These biological signals are essential for stimulating cell proliferation, matrix synthesis, and tissue remodeling [12].
The aim of this meta-analysis was to evaluate the clinical efficacy of LR-PRP in rotator cuff repairs by synthesizing data from randomized controlled trials (RCTs). Our hypothesis is that LR-PRP can lessen postoperative pain and enhance postoperative functional scores.
2. Materials and Methods
This article has been reported in line with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) and AMSTAR (Assessing the methodological quality of systematic reviews) guidelines (Supplementary Material S1) [13,14]. In addition, the methodological guidelines of the Cochrane Handbook of Systematic Reviews were followed in the conduct of this systematic review and meta-analysis [15,16]. This systematic review has been registered with PROSPERO (Registration ID: CRD42024498165).
2.1. Search Strategy
Four databases were searched: Embase, PubMed, Web of Science, and Cochrane Library, up until March 2025. Two authors searched the databases independently, while a third author helped reach a consensus on any differences. The search process used the mode of combining subject terms and free terms. The main keywords used in the search process were as follows: Rotator Cuff, Teres Minor, Subscapularis, Platelet-rich Plasma, and Infraspinatus. The specific retrieval process and details can be referred to in Supplementary Material S2.
2.2. Eligibility Criteria
The eligibility criteria for the systematic review and meta-analysis were based on the PICOS question: P: Patients with rotator cuff tear undergoing arthroscopic repair; I: LR-PRP; C: Standard arthroscopic repair without LR-PRP augmentation (with injection of conventional autologous blood); O: Function score; and S: RCT.
The inclusion criteria were as follows: (1) Partial-thickness injuries classified as Ellman grade II-III involving <50% tendon thickness, or full-thickness injuries ≤3 cm in the sagittal dimension involving 1–2 tendons. (2) More than 150,000 platelets prior to surgery. (3) Preoperative hemoglobin must be at least 11.0 g/dL. (4) The production of PRP adhered to the European Union’s regulatory framework for Substances of Human Origin (SoHO) as outlined in the Directive and its subsequent amendments. (5) The control groups in all included studies underwent standard arthroscopic rotator cuff repair without LR-PRP augmentation. In most trials, the control patients received the conventional autologous blood to maintain blinding. (6) No contagious illnesses.
The exclusion criteria were as follows: (1) Unrepaired tear of subscapular muscle. (2) Patients with osteoarthritis. (3) Prior surgery on the shoulder.
2.3. Data Extraction and Quality Assessment
Two authors separately extracted the data and evaluated its quality, while a third author helped to reach a consensus on any differences. Information such as author, number of patients, results, average age, and sex ratio were extracted. The main outcome indicators extracted in this study are as follows: (1) The Constant Score (CS) is a 100-point shoulder-specific evaluation quantifying pain (15 points), activities of daily living (20 points), active range of motion (40 points), and strength (25 points). Scores ≤55 indicate poor function, scores in the range of 56–70 suggest moderate function, scores in the range of 71–85 signify good function, and scores ≥86 reflect excellent outcomes. (2) The Visual Analog Scale (VAS) is a 10 cm continuum (0 = no pain; 10 = worst imaginable pain) assessing pain severity. Clinically significant improvement was defined as a ≥2-point reduction. (3) The Simple Shoulder Test (SST) comprises 12 binary (yes/no) items evaluating basic shoulder functions. Higher affirmative responses (scores in the range of 0–12) reflect better functional capacity. (4) The American Shoulder and Elbow Surgeons score (ASES) is a combination of 50% patient-reported pain (VAS) and 50% physician-assessed function (10 activities). Total scores ≥75 represent satisfactory outcomes. (5) The UCLA Score is a multidimensional 35-point scale grading pain (10), function (10), active forward flexion (5), strength (5), and satisfaction (5). Scores ≤24 denote unsatisfactory results. The Cochrane risk of bias assessment method was used to examine all randomized trials [17].
2.4. Grading the Evidence
We graded the strength of the evidence for the outcomes using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) guidelines [18]. The evidence was rated on the basis of the following five points: risk of bias, inconsistency, indirectness, imprecision, and publication bias. Finally, the strength of the evidence was divided into high, medium, low, and very low.
2.5. Statistical Analyses
Review Manager 5.4 was used for all meta-analyses, and a two-sided p value below 0.05 was deemed significant. The results of the continuous variables are summarized and represented as a mean difference (MD) with the corresponding 95% confidence interval (CI). The results of the binary variables are summarized and represented as Relative Risk (RR) with the corresponding 95% CI. If considerable heterogeneity was found, the pooled effect sizes were calculated using the random-effect model. If not, a fixed-effect model was used. The amount of heterogeneity among the included studies that could not be entirely attributed to sampling error was assessed using Cochran’s Q statistics and I^2^ statistics. The interpretation of I^2^ values was as follows: low (I^2^: <25%), low to moderate (I^2^: 25–50%), moderate to substantial (I^2^: 50–75%), or substantial (I^2^: >75%). Finally, sensitivity analysis was used to explain the possible heterogeneity of the study.
3. Results
3.1. Search Results
A total of 2096 articles were originally obtained using the search strategy, 937 of which were excluded after removing duplicates, and 1103 were excluded following strict inclusion and exclusion criteria when reading abstracts and titles. Lastly, after reading the full text, 50 more studies were excluded (Supplementary Material S3), resulting in a total of 6 studies that were included. Figure 1 depicts the literature screening procedure.
3.2. Study Characteristics
All studies included in this article are RCTs. All studies compared the effects of using and not using LR-PRP after arthroscopic surgery. Five studies lasted for longer than 12 months [19,20,21,22,23]. The average age of the patients in the experimental and control groups was provided in every study. The patients included in this study were mainly older people over 55 years old. The level of evidence for all included studies was II. The proportion of male and female patients included in this paper is basically the same. Table 1 contains the essential features of every study.
3.3. Quality Evaluation
A total of six RCTs were included, all of which described suitable random sequence generation and randomization methods. However, one study had reporting bias [21]. One study was of medium quality, while the other five were of high quality. (Figure 2).
3.4. GRADE Results
The GRADE rating results of each outcome indicator are shown in Figure 3. GRADE evidence was classified into three levels: high (CS), medium (ASES), and low (UCLA, VAS, and SST).
3.5. Results of Meta-Analysis
3.5.1. Constant Score
A total of six RCTs reported a CS [19,20,21,22,23,24]. An analysis using a fixed-effect model showed differences between the LR-PRP and control groups that were statistically significant (MD = 1.13, 95% CI: 0.19, 2.07, p = 0.02, I^2^ = 47%) (Figure 4).
3.5.2. Visual Analog Scale
A total of four RCTs reported VAS [20,21,23,24]. An analysis using a random-effect model showed differences between the LR-PRP and control groups that were statistically significant (MD = −0.62, 95% CI: −1.16, −0.08, p = 0.02, I^2^ = 83%) (Figure 5).
3.5.3. Other Results
The meta-analysis results of other outcome indicators are as follows: ASES (MD = 6.02, 95% CI: 4.67, 7.36, p < 0.01, I^2^ = 0%), UCLA (MD = 1.20, 95% CI: 0.34, 2.06, p < 0.01, I^2^ = 0%), and SST (MD = 0.08, 95% CI: −0.23, 0.39, p = 0.61, I^2^ = 5%). Although there was a statistical difference between the ASES score and the UCLA score, when we combined the minimum clinically significant difference, we found that these results had no practical clinical significance. In addition, there was no significant difference in SST score (Supplementary Material S4).
4. Discussion
This study’s primary conclusions are that compared with the control group, LR-PRP combined with arthroscopic surgery can improve the CS, ASES, and UCLA after treatment, and reduce the postoperative VAS score of rotator cuff injury patients. However, the experimental and control groups did not show a statistically significantly difference in terms of SST scores. VAS outcome indicators had significant heterogeneity, so we performed a sensitivity analysis on them. After excluding the studies of Zhang [21] and Randelli et al. [23], a fixed-effect model analysis showed statistically significant differences between the LR-PRP and control groups (MD = −1.59, 95% CI: −2.33, −0.85, p < 0.01, I^2^ = 0%). The reason for the heterogeneity of the results in Zhang et al. [21] is that the patients received inconsistent doses of LR-PRP. The source of heterogeneity in the results of Randelli et al. [23] is the difference in follow-up time. The results were consistent with our initial hypothesis. After arthroscopic surgery, LR-PRP can reduce postoperative pain or enhance postoperative functional scores in patients with rotator cuff injuries.
This study’s findings were compared with those of previous studies. According to Yinghao Li et al. [25], PRP therapy decreased pain and enhanced functional outcomes. According to Wennan Xu et al. [26], patients’ retear rate and shoulder discomfort were dramatically decreased, and their long-term shoulder function was enhanced following arthroscopic rotator cuff surgery coupled with PRP. Fu-An Yang and colleagues reported that it is advantageous to administer PRP to the bone–tendon interface during surgery [27]. Although the above study did not classify PRP, it still came to conclusions that are similar to ours. However, other researchers have come to conclusions that are the opposite of ours. According to a research study by Pietro Feltri et al. [28], using PRP as an enhancer during arthroscopic surgery for rotator cuff injuries did not significantly improve clinical results. In another study, You-zhi Cai et al. [29] discovered no meaningful statistical difference in clinical outcome scores between treatment with PRP and treatment without PRP in full-layer rotator cuff repair. Jia-Guo Zhao et al. reported similar clinical outcomes in the PRP and control groups [30]. Upon a thorough review of these studies, it was observed that a significant portion of the original research included in these studies concentrated on studying the effects of LP-PRP. These outcomes after surgery in rotator cuff injuries may be a function of LP-PRP rather than LR-PRP.
The meta-analysis revealed substantial heterogeneity in follow-up durations and PRP administration protocols across studies. Specifically, the Randelli P et al. [20] and Randelli PS et al. [23] cohorts represent longitudinal data from the same patient population at 2-year and 10-year intervals. While pooling these datasets introduces temporal heterogeneity, it provides unique insights into the sustained effects of LR-PRP. Nevertheless, the inclusion of overlapping cohorts may inadvertently amplify treatment effect estimates. Additionally, methodological variations in PRP delivery could differentially modulate biologic activity. Snow M et al. [22] administered LR-PRP 10–14 days postoperatively, diverging from intraoperative applications in other trials. This protocol discrepancy may attenuate the regenerative potential of LR-PRP due to delayed inflammatory phase engagement.
Considering the aforementioned studies related to LR-PRP, we suppose that the mechanisms of LR-PRP in patients with rotator cuff injuries is as follows: 1. LR-PRP is rich in growth factors such as platelet-derived growth factor (PDGF), transforming growth factor-beta (TGF-β), vascular endothelial growth factor (VEGF), and epidermal growth factor (EGF) [31]. These factors can promote the proliferation and differentiation of tenocytes and fibroblasts, which are crucial for tendon repair and regeneration. 2. The presence of growth factors like VEGF in LR-PRP could stimulate angiogenesis, which is the formation of new blood vessels [32]. This is critical for supplying nutrients and oxygen to the healing rotator cuff tissues, thereby accelerating the repair process. 3. Growth factors within LR-PRP may also play a role in modulating pain through the inhibition of nociceptive (pain-sensing) pathways, providing symptomatic relief to patients [33]. 4. Factors within LR-PRP can stimulate the synthesis of collagen, an essential component of tendon tissue [34]. Increased collagen synthesis can improve the structural integrity of the repaired tendon.
Another issue is the cost of LR-PRP. When considering the adoption of a medical technology, its value depends on whether it can improve clinical outcomes. The application of LR-PRP in arthroscopic rotator cuff repair has been shown to potentially reduce postoperative discomfort and improve postoperative functional scores, particularly for individuals with rotator cuff injuries. This is highly significant, as it suggests the opportunity for a faster recovery and an improved quality of life for the patients. Therefore, the cost-effectiveness of LR-PRP is not solely about immediate outcomes but is also about long-term patient health. Given that LR-PRP can enhance recovery by lessening postoperative pain and improving postoperative functional scores, it can potentially lead to lower long-term healthcare costs resulting from ongoing concerns or complications. Therefore, the use of LR-PRP in arthroscopic rotator cuff repair can be viewed as a worthwhile expenditure in the pursuit of improved patient outcomes and long-term health benefits.
This study has several limitations. First, only articles written in English were included in this study. Second, there was insufficient data for subgroup analysis. Third, the sample size included in most randomized controlled trials is limited, which reduces the statistical ability to detect clinically significant differences and increases the risk of type II errors. Randomized controlled trials with larger sample sizes are needed in future studies. Fourth, the included studies did not stratify outcomes by clinical risk factors such as diabetes mellitus and smoking status. Finally, the included studies did not address the use of PRP in immunodeficient patients or those with coagulation disorders, which are populations that may require modified biologic strategies. Certain limitations must also be considered when interpreting and drawing conclusions from the data. Therefore, these limitations need to be carefully weighed when interpreting the findings and incorporating them into a comprehensive analysis of the results.
5. Conclusions
Based on the current evidence, the use of LR-PRP in arthroscopic rotator cuff repair could lessen postoperative pain and improve postoperative functional scores in individuals with rotator cuff injuries.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Teunis T. Lubberts B. Reilly B.T. Ring D. A systematic review and pooled analysis of the prevalence of rotator cuff disease with increasing age J. Shoulder Elb. Surg.2014231913192110.1016/j.jse.2014.08.00125441568 · doi ↗ · pubmed ↗
- 2Goodman R.S. Abnormal findings on magnetic resonance images of asymptomatic shoulders J. Bone Jt. Surg. Am.19967863310.2106/00004623-199604000-000208609145 · doi ↗ · pubmed ↗
- 3Arce G. Bak K. Bain G. Calvo E. Ejnisman B. Di Giacomo G. Gutierrez V. Guttmann D. Itoi E. Ben Kibler W. Management of disorders of the rotator cuff: Proceedings of the ISAKOS upper extremity committee consensus meeting Arthroscopy 2013291840185010.1016/j.arthro.2013.07.26524041864 · doi ↗ · pubmed ↗
- 4Giuseppe M. NiccolòV. Giuseppe F. Maristella F.S. Rationale of Tendon-to-Bone Healing Fundamentals of the Shoulder Springer International Publishing Cham, Switzerland 20226174
- 5Kirschner J.S. Cheng J. Hurwitz N. Santiago K. Lin E. Beatty N. Kingsbury D. Wendel I. Milani C. Ultrasound-guided percutaneous needle tenotomy (PNT) alone versus PNT plus platelet-rich plasma injection for the treatment of chronic tendinosis: A randomized controlled trial Pm R 2021131340134910.1002/pmrj.1258333644963 · doi ↗ · pubmed ↗
- 6Anitua E. Sánchez M. Nurden A.T. Nurden P. Orive G. Andía I. New insights into and novel applications for platelet-rich fibrin therapies Trends Biotechnol.20062422723410.1016/j.tibtech.2006.02.01016540193 · doi ↗ · pubmed ↗
- 7Zhang C. Wu J. Li X. Wang Z. Lu W.W. Wong T.-M. Current Biological Strategies to Enhance Surgical Treatment for Rotator Cuff Repair Front. Bioeng. Biotechnol.2021965758410.3389/fbioe.2021.65758434178957 PMC 8226184 · doi ↗ · pubmed ↗
- 8Dohan Ehrenfest D.M. Rasmusson L. Albrektsson T. Classification of platelet concentrates: From pure platelet-rich plasma (P-PRP) to leucocyte- and platelet-rich fibrin (L-PRF)Trends Biotechnol.20092715816710.1016/j.tibtech.2008.11.00919187989 · doi ↗ · pubmed ↗